Page 13 of 23
IM10.17-22 | AKI and CKD Management — SDL Guide
Learning Objectives
- Communicate diagnosis, treatment plan, and follow-up to patients with AKI and CKD
- Counsel patients on a renal diet tailored to AKI and CKD stage
- Outline the priorities in AKI management including volume management, drug dose alteration, monitoring, and dialysis indications
- Describe supportive therapy in CKD including antihypertensives, glycaemic agents, anaemia, dyslipidaemia, hyperkalaemia, hyperphosphataemia, and secondary hyperparathyroidism
- Describe the indications for renal dialysis and renal replacement therapy
INSTRUCTIONS
This management module integrates pharmacological, nutritional, and procedural approaches for both AKI and CKD. It covers the full breadth of IM10.17–10.22 and is the companion to the diagnostic modules you have already completed. Management decisions flow directly from the clinical evaluation and diagnostic findings.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 307–308 — AKI and CKD management (textbook)
- API Textbook of Medicine, 10th ed., Ch. Nephrology — Management of Renal Failure (textbook)
- KDIGO 2012 AKI Clinical Practice Guideline (guideline)
- KDIGO 2012 CKD Clinical Practice Guideline — Evaluation and Management (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Anitha is a general medicine registrar seeing two patients on the same afternoon. The first is Ramu, a 62-year-old farmer with AKI Stage 2 from dehydration and NSAID use, now admitted and haemodynamically stable. Ramu's family is anxious — they want to know if the kidneys will recover, how long he will need to stay, and what he can eat. The second patient is Meena, a 54-year-old housewife with CKD G4 (eGFR 22) from diabetic nephropathy. Meena has come with a list of twelve medications prescribed by four different doctors, including two NSAIDs and metformin, none of which she should be taking. Her phosphate is 7.2 mg/dL, her haemoglobin is 8.3 g/dL, and her HbA1c is 9.1%. Both patients need a management plan today — not eventually, not after a nephrology consultation next week, but today. The management of renal failure at the final-year MBBS level is not a catalogue of drugs and doses to memorise — it is a coherent therapeutic strategy, built from the understanding of why each complication develops and how each intervention addresses the underlying mechanism. This module gives you that strategy.
WHY THIS MATTERS
Renal failure management is a final-year clinical competency assessed at multiple levels: communicating the diagnosis and plan to patients (IM10.17, SH), providing dietary counselling (IM10.18, SH), prioritising AKI management steps (IM10.19, KH), managing CKD complications medically (IM10.20, KH), and knowing when to refer for dialysis (IM10.21–10.22, KH). In the Indian context, management is further complicated by cost constraints, access to specialist care, traditional medication use, and high rates of diabetic nephropathy — all of which require culturally-sensitive, practical communication skills alongside technical medical knowledge.
RECALL
Before proceeding, recall the AEIOU indications for emergency dialysis from the AKI Foundations module: Acidosis (pH <7.1), Electrolytes (refractory hyperkalaemia), Intoxication (dialysable toxins), Overload (pulmonary oedema), Uraemia (pericarditis, encephalopathy, bleeding). Recall also the CKD-MBD cascade: reduced GFR → phosphate retention → ↑FGF-23 → ↓calcitriol → ↑PTH (secondary hyperparathyroidism). And recall the target Hb range for ESA therapy in anaemia of CKD: 10–11.5 g/dL. These form the framework within which the management interventions described in this module operate.
Communicating Diagnosis and Plan to Patients with Renal Failure
Effective patient communication in renal failure is a clinical skill with direct consequences for adherence, anxiety management, and outcomes. Patients and families confronting a diagnosis of AKI or CKD are commonly overwhelmed, frightened, and confused — they may misinterpret 'kidney failure' as immediately terminal or may minimise the severity because they feel well despite advanced disease. The clinician's task is to provide clear, accurate, proportionate information calibrated to the patient's health literacy, cultural context, and emotional state.
Provided image
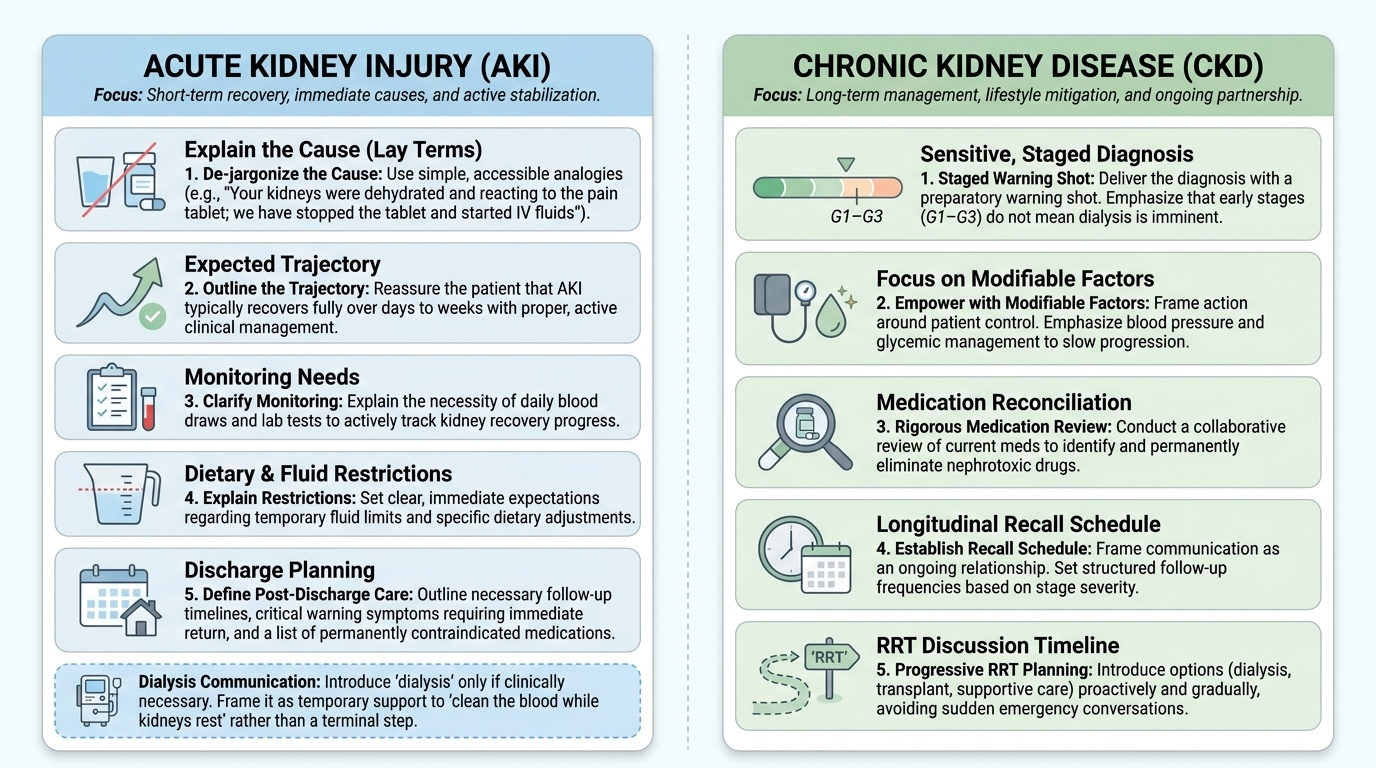
For AKI, the key communication points are: (1) explain the cause clearly and in lay terms ('Your kidneys were not getting enough blood because of the dehydration and the pain tablet you were taking — we have stopped the tablet and are giving you fluids'); (2) explain the expected trajectory — most AKI from pre-renal or early ATN causes recovers fully with treatment, typically over days to weeks; (3) explain monitoring needs ('We will check your blood tests daily to track the recovery'); (4) explain restrictions ('For now, we are restricting fluids and some foods — I will explain the diet in detail'); (5) explain discharge planning — what follow-up is needed, what symptoms should prompt urgent return, and what medications to avoid permanently. The word 'dialysis' should be introduced only if clinically necessary, and when it is, the physician must explain it as a support measure ('It cleans your blood temporarily while your kidneys recover') rather than as a terminal intervention.
For CKD, communication is a longitudinal relationship, not a single consultation. Key principles: (1) deliver the diagnosis sensitively — many patients discover CKD incidentally and are shocked; use a 'warning shot' ('I want to talk to you about something important I found in your blood tests'); (2) explain the staged nature of CKD and that G1–G3 does not necessarily mean dialysis in the near future; (3) focus on modifiable factors — 'the single most important thing you can do today is control your blood pressure and sugar; that will slow the kidney damage significantly'; (4) address medication reconciliation explicitly — many patients with CKD have contraindicated medications that must be stopped today, not when they next see a specialist; (5) use a structured recall system — 'I will see you in 3 months; between now and then, take these tablets, eat this diet, and come back immediately if you develop swelling, breathlessness, or reduced urine.' Shared decision-making around renal replacement therapy, when that becomes relevant, requires multiple conversations, ideally with the patient's family and a nephrologist, and must respect patient preferences and cultural values.
Renal Diet Counselling — AKI and CKD Specific Guidance
Dietary management in renal failure is not a single 'low-protein diet' prescription — it is a nuanced, stage-specific intervention that addresses protein, potassium, phosphate, sodium, and fluid intake, with the content varying significantly between AKI and different stages of CKD. The physician must be able to explain the rationale of each dietary restriction to the patient in practical terms, and must work with a renal dietitian when possible for individualised guidance.
Provided image
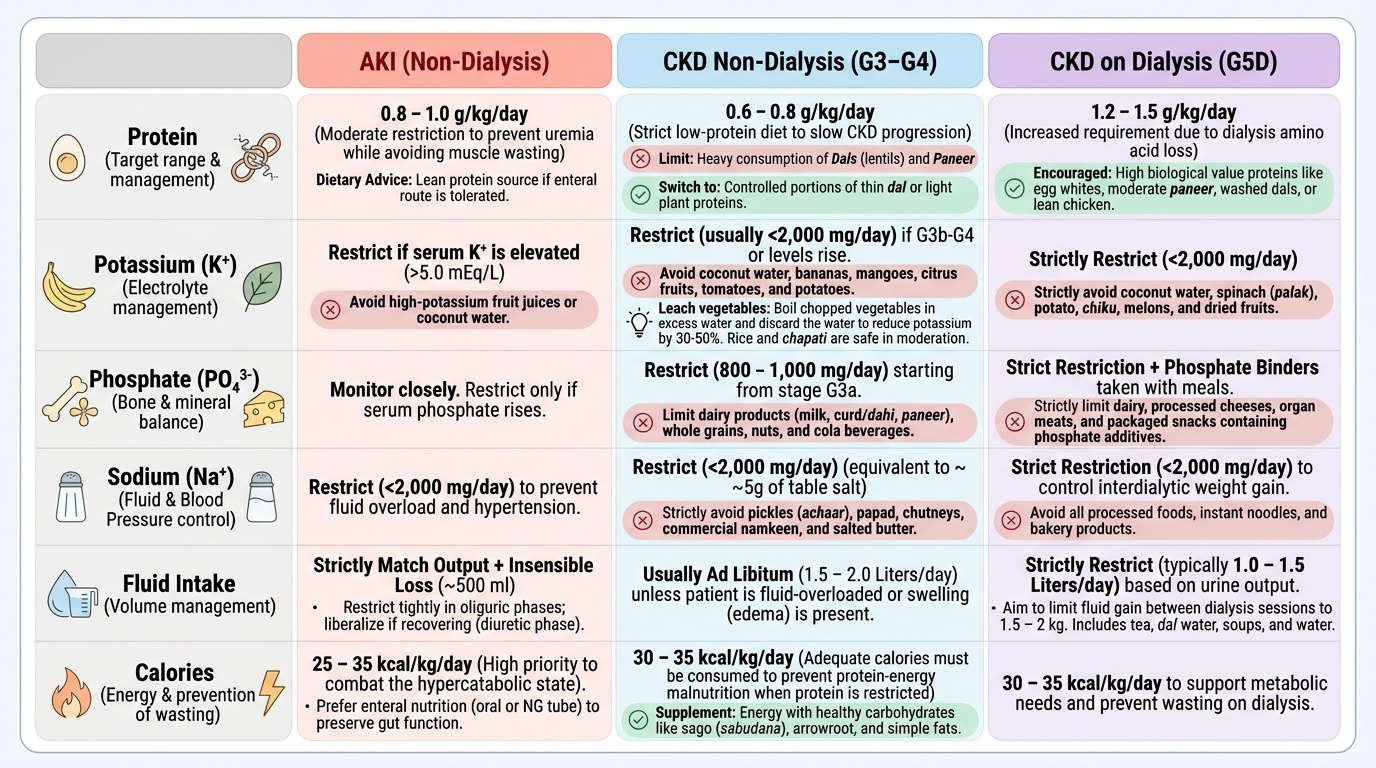
Protein intake in AKI: AKI generates a hypercatabolic state with increased protein breakdown. Restricting protein too severely worsens malnutrition and delays recovery. Current recommendations (KDIGO 2012): non-dialysed AKI = 0.8–1.0 g/kg/day protein; AKI on continuous renal replacement therapy (CRRT) = 1.5–1.7 g/kg/day (CRRT removes amino acids and augments protein loss); parenteral nutrition if enteral not tolerated. Total calorie goal: 25–35 kcal/kg/day. Preferred source: enteral route (NG tube if necessary); avoid parenteral nutrition unless GI tract completely non-functional.
Protein intake in CKD: The evidence for low-protein diets (LPD) in slowing CKD progression is strongest in G3b–G4: the MDRD study and subsequent meta-analyses support a target of 0.6–0.8 g/kg/day (LPD) for non-dialysed CKD patients with proteinuria. However, this must be balanced against the risk of protein-energy malnutrition, which is common in CKD and independently worsens outcomes. In practice, a target of 0.8 g/kg/day with adequate caloric supplementation is commonly recommended. In dialysis patients (G5D), protein must be INCREASED to 1.2–1.5 g/kg/day because dialysis removes amino acids.
Potassium restriction: Indicated when serum potassium is above the normal range or when the patient has CKD G3b–G5 with high dietary potassium intake. High-potassium foods to avoid or limit: bananas, oranges, mangoes, coconut water, potatoes, tomatoes, dried fruits, nuts, and legumes. In practice, advise patients to boil vegetables and discard the water (leaching reduces potassium content by 30–50%). Indian dietary staples like rice and chapati are lower in potassium than legumes and leafy greens and can generally be continued in moderation.
Phosphate restriction: Indicated in CKD G3a onwards when phosphate begins to rise. High-phosphate foods: dairy products (milk, cheese, curd/yoghurt — advise moderate restriction), nuts, seeds, whole grains, and most importantly processed foods with phosphate additives (packaged snacks, cola drinks, processed meats — phosphate additives from these are 100% bioavailable, unlike organic phosphate from natural foods which is only 30–60% absorbed). Phosphate binders taken WITH meals trap intestinal phosphate and must be counselled as 'taken with food, not after' — calcium carbonate 500–1000 mg or sevelamer carbonate 800 mg with each meal.
Sodium restriction: Reduces hypertension and oedema in CKD; particularly important in anuric dialysis patients. Target <2 g sodium/day (5 g NaCl/day). Practical advice: avoid adding salt at the table, limit pickles, papads, salted snacks, processed foods. Low-sodium salt substitutes (potassium chloride) must NOT be used in CKD patients as they are high in potassium.
Fluid restriction: Required in oliguric AKI (maintenance = insensible losses 500–800 mL + previous day urine output), anuric dialysis patients, and volume-overloaded CKD. Standard advice in dialysis patients: fluid allowance = 500–750 mL/day + previous day urine output; weigh daily; report weight gain >1 kg/day.
SELF-CHECK
A 60-year-old woman with CKD G4 and serum potassium 6.1 mEq/L asks about her diet. Which dietary advice is CORRECT for this patient?
A. Use potassium chloride salt substitute instead of sodium chloride to reduce her blood pressure
B. She may eat coconut water freely as it is a natural product with no processing
C. Boil vegetables and discard the cooking water to reduce potassium content
D. Increase fruit intake as the antioxidants will protect her kidneys
Reveal Answer
Answer: C. Boil vegetables and discard the cooking water to reduce potassium content
Boiling vegetables and discarding the water (leaching) reduces potassium content by 30–50% and is a practical, evidence-based dietary strategy for CKD patients. Potassium chloride salt substitutes are dangerous in CKD — they are high in potassium and can precipitate life-threatening hyperkalaemia. Coconut water is extremely high in potassium (approximately 600 mg per cup) and must be avoided in CKD with hyperkalaemia. Increasing fruit intake in a patient with K 6.1 mEq/L would further raise potassium — fruits like bananas and oranges are high in potassium and should be restricted.
AKI Management Priorities — Diet, Volume, Drugs, Monitoring, Dialysis
The management of established AKI is organised around five priority domains that should be addressed simultaneously in every patient, with the intensity of each domain scaled to the KDIGO stage and the underlying category of AKI. These priorities are the practical operationalisation of the diagnostic and pathophysiological knowledge from the earlier modules, and they are the content of IM10.19 at the KH level.
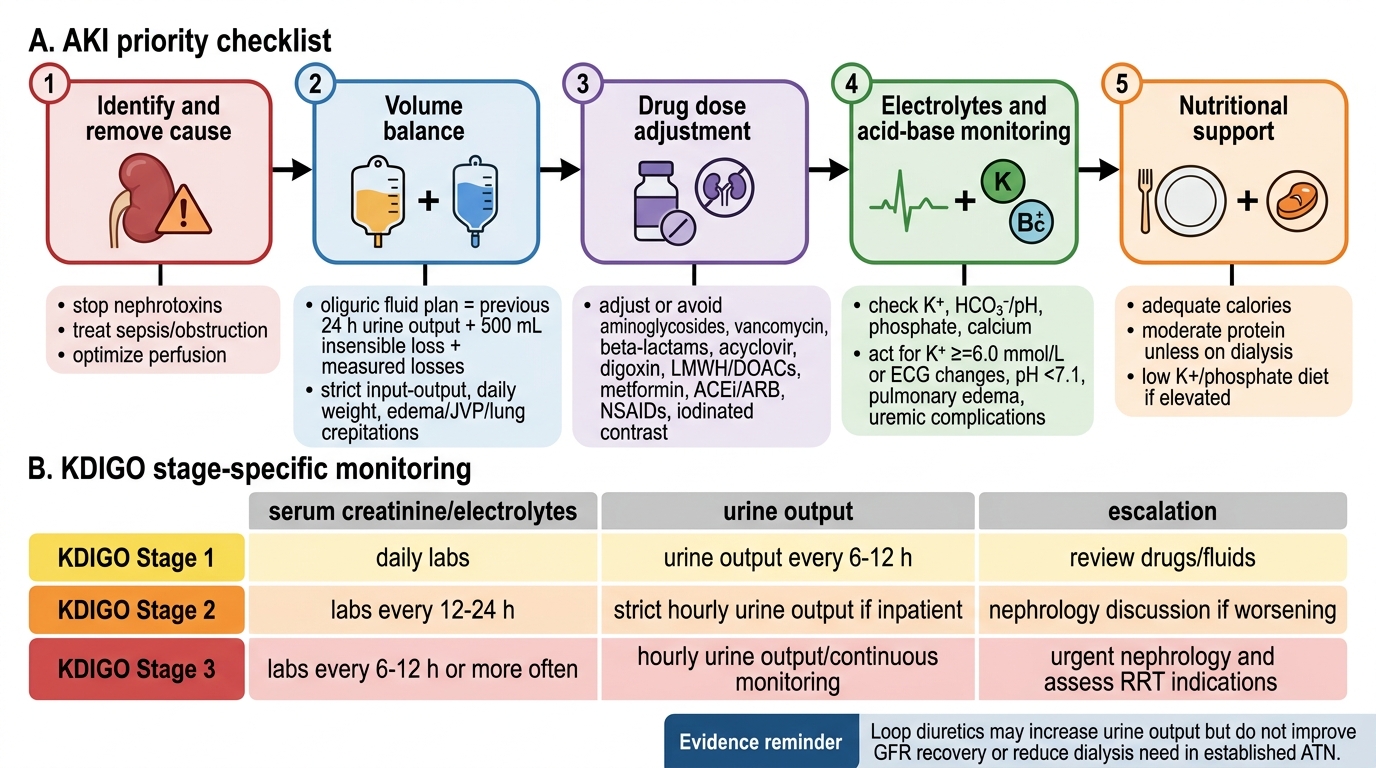
Priority 1 — Identify and remove the cause: Every AKI management plan begins with addressing the aetiology. Stop all nephrotoxic medications (NSAIDs, aminoglycosides, contrast agents — never give contrast to an AKI patient without a risk-benefit discussion). Restore volume in pre-renal AKI (isotonic saline or Hartmann's solution, titrated to clinical response — JVP, urine output, blood pressure). Relieve obstruction in post-renal AKI (urethral catheter, nephrostomy). Immunosuppression for severe glomerulonephritis if biopsy-confirmed. Treat the underlying illness driving the AKI (sepsis management, treatment of leptospirosis with benzylpenicillin or doxycycline, treatment of malaria with appropriate antimalarials — in India, consider these infective causes actively).
Priority 2 — Volume and fluid balance management: In the oliguric maintenance phase of AKI, daily fluid allowance = insensible losses (approximately 500–800 mL/day) + previous 24-hour urine output + measurable extrarenal losses (vomiting, diarrhoea, wound drainage). Daily weights are mandatory — a weight gain of more than 0.5 kg/day indicates fluid accumulation beyond insensible losses. Strict intake-output charting must be maintained. Avoid excessive fluid loading — aggressive fluid resuscitation that was appropriate in the initiation phase may cause pulmonary oedema in the maintenance phase. Loop diuretics (furosemide) do NOT improve recovery from ATN or reduce the need for dialysis — they may convert oliguric to non-oliguric AKI (improving fluid management) but should not be used in the hope that diuresis means recovery.
Priority 3 — Drug dose adjustment: This is one of the most practically important and most frequently neglected aspects of AKI management. Every renally cleared drug must be reviewed and adjusted. Critical examples: aminoglycosides (monitor trough levels; extend dosing interval — once-daily dosing preferred in AKI); vancomycin (monitor trough levels, extend interval); metformin (STOP — risk of lactic acidosis, resume only when creatinine has returned to baseline and eGFR >45); digoxin (reduce dose — renal clearance impaired, narrow therapeutic window); NSAIDs (ABSOLUTELY CONTRAINDICATED — worsen AKI by blocking prostaglandin-mediated afferent arteriolar dilation); enoxaparin/LMWH (reduce dose and monitor anti-Xa levels — accumulation causes bleeding risk); methotrexate (STOP — nephrotoxic and renally cleared). A systematic medication review using the current eGFR or creatinine clearance (Cockcroft-Gault for dosing decisions) must be performed within the first 24 hours.
Priority 4 — Electrolyte and acid-base monitoring: Check serum potassium, bicarbonate, sodium, calcium, and phosphate every 4–6 hours in Stage 2–3 AKI or any oliguric patient. Manage hyperkalaemia as previously described (calcium gluconate → insulin/dextrose → loop diuretic if urine present → Resonium → dialysis if refractory). Manage metabolic acidosis: oral or IV sodium bicarbonate for HCO₃⁻ <15 mEq/L in a non-oliguric patient who can tolerate the sodium load; dialysis for HCO₃⁻ <10 mEq/L or pH <7.1. Manage hypocalcaemia cautiously — in rhabdomyolysis, do not correct hypocalcaemia with IV calcium unless the patient is symptomatic or has ECG changes, because correction during the acute phase risks calcium precipitation in injured muscle.
Priority 5 — Nutritional support: As covered in the diet section above: protein 0.8–1.0 g/kg/day; caloric target 25–35 kcal/kg/day; enteral route preferred; dietitian referral early in established AKI.
Monitoring in AKI: In KDIGO Stage 1 — daily creatinine, BMP, urine output (hourly catheter if oliguric); Stage 2 — as above plus twice-daily potassium, ECG monitoring if K >5.5; Stage 3 — intensive monitoring, ICU consideration, nephrology referral, prepare for potential RRT. Endpoints of recovery: rising urine output, falling creatinine, improving electrolytes — but monitor for the diuretic phase with associated electrolyte depletion.
AKI Management Priority Checklist
SELF-CHECK
A patient with AKI Stage 2 from gentamicin ATN is haemodynamically stable and producing 40 mL/h of urine. His creatinine is 3.2 mg/dL and rising. His physician prescribes furosemide 80 mg IV to 'drive the kidneys.' Which statement about this decision is CORRECT?
A. Furosemide will accelerate GFR recovery by flushing tubular casts
B. Furosemide may increase urine output but will not improve GFR recovery or reduce the need for dialysis
C. Furosemide should be given together with mannitol for maximum effect in ATN
D. Furosemide is contraindicated in any form of AKI
Reveal Answer
Answer: B. Furosemide may increase urine output but will not improve GFR recovery or reduce the need for dialysis
Multiple randomised trials (including the FACTT trial and meta-analyses) have confirmed that furosemide does not improve GFR recovery in established ATN and does not reduce mortality or the need for dialysis. It may convert oliguric to non-oliguric ATN (making fluid management easier) but has no nephroprotective effect. Furosemide + mannitol has no evidence base in ATN and mannitol can worsen osmotic nephropathy. Furosemide is not absolutely contraindicated in AKI — it is used for fluid overload management — but using it with the expectation of renal recovery is incorrect and reflects a common misconception.