Page 2 of 23
IM10.1-3 | AKI Foundations — SDL Guide (Part 2)
Natural History and Clinical Phases of AKI
The natural history of AKI — particularly ischaemic ATN — follows a characteristic progression through four recognisable clinical phases. Understanding this trajectory is essential for clinical management, because the therapeutic priorities differ at each phase, and conflating them leads to errors such as pushing fluids in the diuretic phase or withholding dialysis in the oliguric phase.
Phase 1 — Initiation (hours to days): The precipitating insult occurs (ischaemia, nephrotoxin). GFR is falling but creatinine has not yet risen appreciably — the creatinine lags by 24–48 hours because it takes time for creatinine to accumulate in the extracellular fluid once production exceeds elimination. This is the window for prevention: correcting hypotension, removing nephrotoxins, and ensuring adequate hydration. Urine output may still be normal. The initiation phase may be clinically silent, which is why AKI is often detected late.
Phase 2 — Extension (hours to 1–2 days): Ischaemia and inflammation continue. Tubular injury is propagated by inflammatory cytokines (TNF-α, IL-6, IL-18), continued vasoconstriction, and neutrophil infiltration of the peritubular capillaries. This is where pre-renal AKI transitions to established ATN. The GFR continues to fall, creatinine rises rapidly, and oliguria becomes established. The therapeutic window for simple fluid correction closes here.
Phase 3 — Maintenance (typically 1–2 weeks, range days to weeks): This is the established oliguric phase. GFR is at its nadir. The tubular epithelium is necrotic and sloughed. Uraemia accumulates, necessitating monitoring and — when indicated — dialysis. Key complications during maintenance: hyperkalaemia (from oliguria + cell lysis + acidosis-driven K⁺ shift), metabolic acidosis (bicarbonate reabsorption fails and acid accumulates), hyponatraemia (if excessive hypotonic fluids given), fluid overload (pulmonary oedema, hypertension), and uraemia-related pericarditis and encephalopathy. This is the phase where fluid intake is restricted to insensible losses plus the previous day's urine output.
Phase 4 — Recovery (diuretic phase, weeks to months): As tubular cells regenerate (the tubular basement membrane, if intact, serves as the scaffold), the GFR begins to recover. The newly regenerated tubular cells initially lack full reabsorptive capacity, producing a diuretic phase — urine output climbs, sometimes dramatically (>3–4 L/day), even while GFR is still below normal. This brisk diuresis is not a sign that the kidney has fully recovered; it is driven by tubular immaturity plus the osmotic diuresis from the accumulated urea. A critical management error is to stop monitoring creatinine or to discharge the patient because 'urine is flowing' — the creatinine may still be falling and electrolyte depletion during the diuretic phase can be severe. Full GFR recovery may take weeks to months; incomplete recovery (residual CKD) occurs in approximately 10–30% of ATN survivors, depending on the severity and duration of injury.
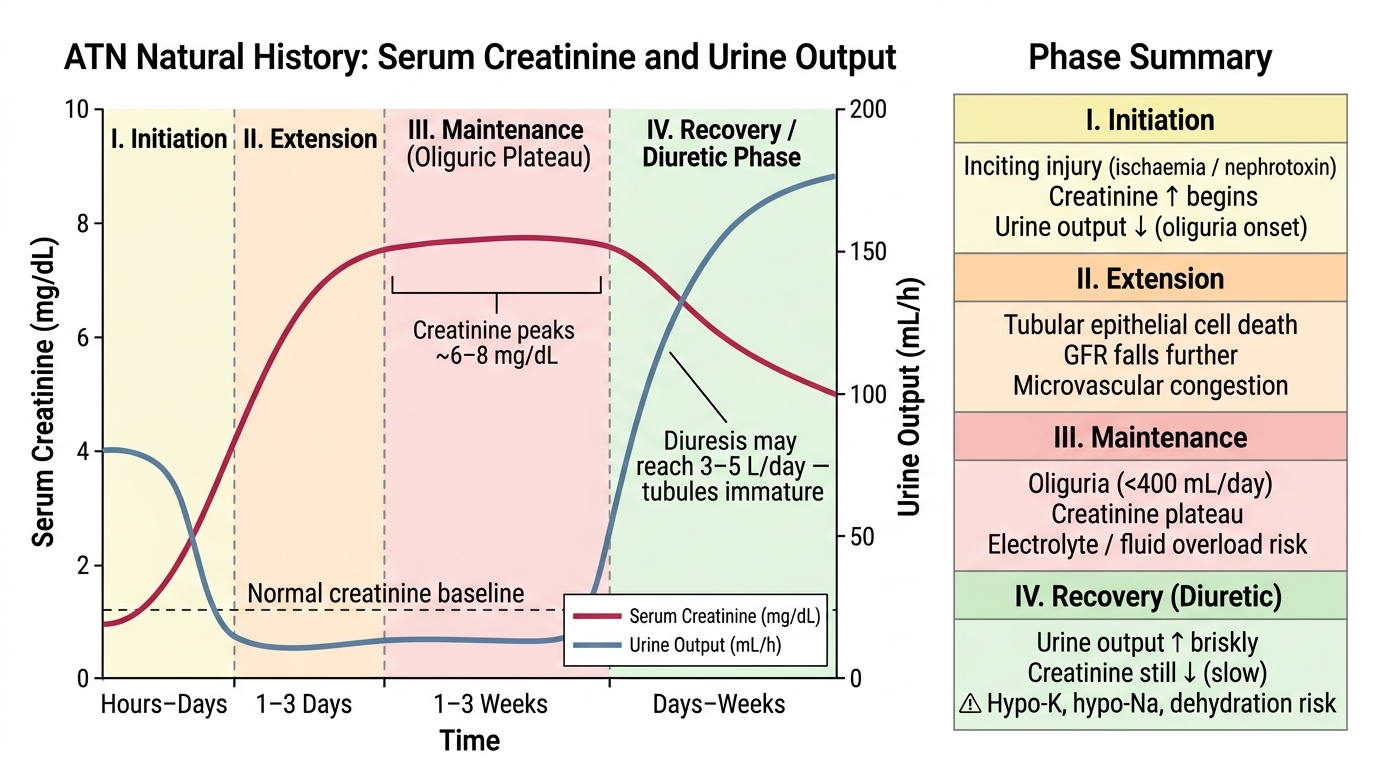
Natural History of Acute Tubular Necrosis: Creatinine and Urine Output Across Four Phases
SELF-CHECK
A patient with ischaemic ATN from septic shock has been oliguric for 10 days. Today his urine output has suddenly increased to 2.8 L in 24 hours. His creatinine is still 3.2 mg/dL (was 4.1 mg/dL yesterday). Which of the following management steps is MOST important at this point?
A. Restrict fluid intake to 500 mL/day as oliguria has resolved
B. Stop all monitoring since the diuresis indicates renal recovery
C. Carefully replace urine losses and monitor electrolytes for hypokalaemia and hyponatraemia
D. Initiate haemodialysis because creatinine remains elevated above normal
Reveal Answer
Answer: C. Carefully replace urine losses and monitor electrolytes for hypokalaemia and hyponatraemia
The patient has entered the diuretic (recovery) phase of ATN. The brisk diuresis is caused by immature tubular cells that cannot fully reabsorb the filtrate — not because the kidney is fully recovered. Creatinine is still falling (from 4.1 to 3.2 mg/dL), confirming progressive but incomplete recovery. The danger in this phase is electrolyte depletion (hypokalaemia, hyponatraemia, hypomagnesaemia) and dehydration from unreplaced urine losses. Fluid restriction would cause volume depletion. Stopping monitoring is dangerous — creatinine is still elevated. Haemodialysis is not indicated when the trend is improving.
Initial Management Priorities in AKI
The management of AKI is centred on five priority actions that should be executed simultaneously in any patient identified to have AKI. These priorities apply regardless of the final aetiology and should be initiated before the full cause is established. The pneumonic AEIOU captures the classical indications for emergent dialysis; the broader management framework addresses everything that precedes the decision to dialyse.
Priority 1 — Identify and correct the cause. The pre-renal/intrinsic/post-renal classification must be established urgently: assess volume status (mucous membranes, JVP, skin turgor, postural BP drop, capillary refill), review the medication list for nephrotoxins, review fluid balance charts, and obtain renal ultrasound to exclude obstruction. Nephrotoxins (aminoglycosides, NSAIDs, contrast, herbal preparations) must be stopped immediately. If obstruction is present, relieve it promptly (catheter for bladder outlet obstruction; nephrostomy or ureteric stent for upper tract obstruction). If volume depletion is the cause, begin isotonic crystalloid resuscitation (normal saline or Hartmann's solution — colloids offer no advantage). However, avoid blind fluid loading in the patient who is already euvolaemic or oedematous — pre-renal AKI in heart failure or liver disease requires careful diuresis, not fluids.
Priority 2 — Manage hyperkalaemia. Hyperkalaemia is the most immediately life-threatening electrolyte complication of AKI. Monitor serum potassium every 4–6 hours in established AKI. A potassium >6.5 mEq/L, or any elevation with ECG changes (peaked T-waves, widening QRS, sine-wave pattern, ventricular fibrillation), is a medical emergency. The treatment sequence is: (a) membrane stabilisation — calcium gluconate 10% 10 mL IV over 3 minutes (does not lower potassium but protects the myocardium within minutes); (b) shift into cells — insulin 10 units IV + 50% dextrose 50 mL (onset 15–30 min), sodium bicarbonate in acidaemic patients (shifts K⁺ into cells), salbutamol nebulisation (β₂-agonist stimulates Na/K-ATPase); (c) remove from body — loop diuretics if urine output present, Resonium (sodium polystyrene sulfonate) orally or per rectum, or dialysis if refractory or in severe AKI.
Priority 3 — Volume management. In oliguric AKI, daily fluid allowance = insensible losses (~500–800 mL/day for average adult) + previous day's urine output + extrarenal losses (vomiting, diarrhoea, fever). Excessive fluid administration causes pulmonary oedema and worsens outcomes. Daily weights and strict intake-output charting are mandatory.
Priority 4 — Dose-adjust medications. Renally excreted drugs require dose reduction or extended dosing intervals: aminoglycosides, vancomycin, metformin (must be stopped to prevent lactic acidosis), digoxin, methotrexate, NSAIDs (absolutely contraindicated). Prescribing an unchanged dose of a renally cleared drug in AKI is one of the most preventable medication errors in clinical practice.
Priority 5 — Nutritional support. AKI generates a hypercatabolic state. Protein intake is restricted but NOT eliminated: in non-dialysis AKI, protein 0.8–1.0 g/kg/day; in patients on dialysis, protein 1.2–1.5 g/kg/day (because dialysis removes amino acids). Total caloric intake should be 25–35 kcal/kg/day. Caloric supplementation with carbohydrates and fats. Enteral route preferred over parenteral. A renal dietitian referral should be made early in established AKI.
The AEIOU indications for emergency dialysis are: Acidosis (metabolic, pH <7.1, refractory to bicarbonate); Electrolyte disturbance (hyperkalaemia refractory to medical management, or Na <115 or >165 mEq/L); Intoxication (dialysable poisons: salicylates, methanol, ethylene glycol, lithium — use activated charcoal for organophosphate overdose, not dialysis); Overload (pulmonary oedema refractory to diuretics); Uraemia (pericarditis, encephalopathy with asterixis/seizures, bleeding from uraemic platelet dysfunction, serum urea >100–150 mg/dL with uraemic symptoms).
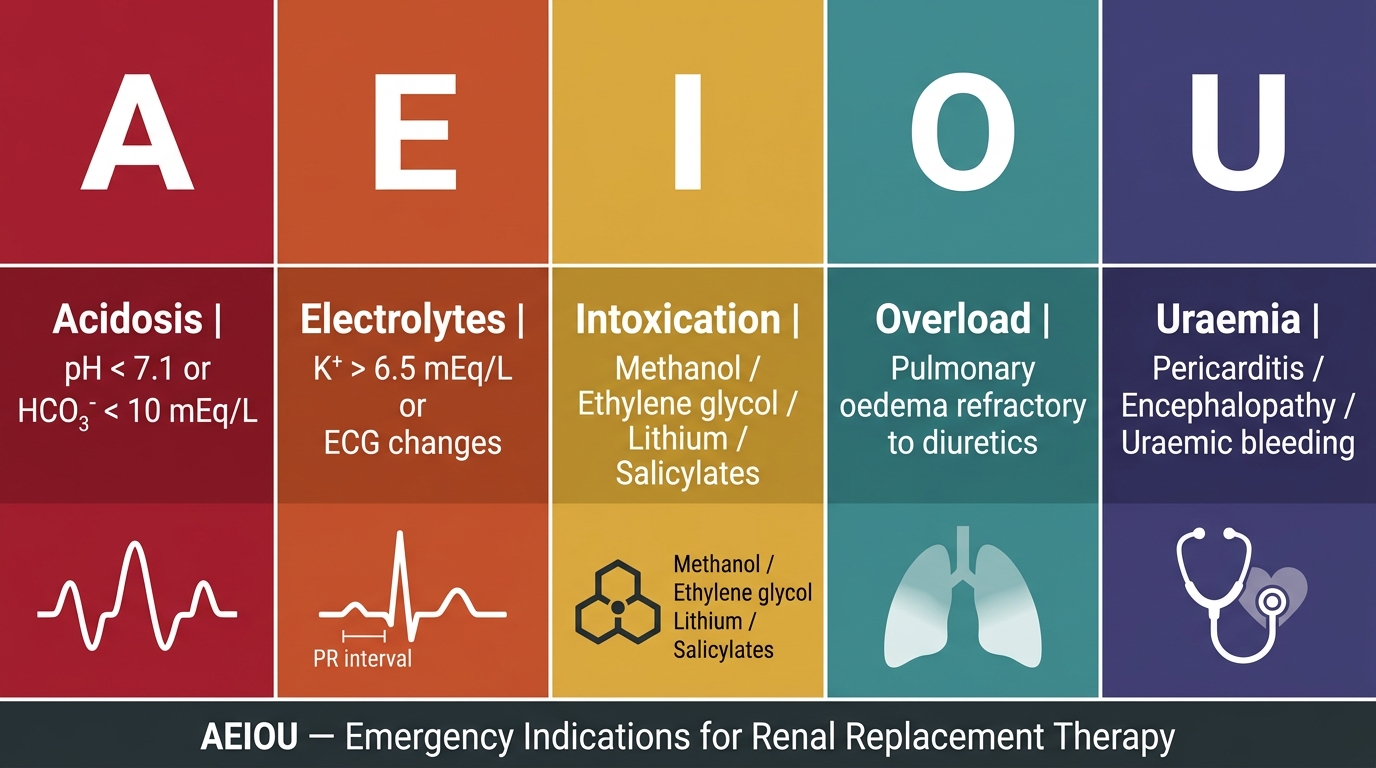
AEIOU Mnemonic — Emergency Indications for Renal Replacement Therapy
SELF-CHECK
A patient with Stage 3 AKI has serum potassium of 7.1 mEq/L. His ECG shows peaked T-waves and a PR interval of 240 ms. Which of the following should be given FIRST?
A. Sodium bicarbonate 50 mEq IV
B. Insulin 10 units + 50% dextrose IV
C. Calcium gluconate 10% 10 mL IV
D. Sodium polystyrene sulfonate (Resonium) orally
Reveal Answer
Answer: C. Calcium gluconate 10% 10 mL IV
In hyperkalaemia with ECG changes, the immediate priority is membrane stabilisation to prevent ventricular arrhythmia. Calcium gluconate does not lower serum potassium but directly antagonises the cardiac membrane toxicity of hyperkalaemia within 1–3 minutes — it is the most immediately life-saving intervention. Insulin + dextrose shifts potassium into cells (onset 15–30 min) and is given next. Sodium bicarbonate can also shift potassium intracellularly and is appropriate in metabolic acidosis. Resonium (kayexalate) removes potassium from the body over hours and is the slowest-acting option — important for sustained clearance, not for acute emergency.
CLINICAL PEARL
The serum creatinine is a lagging indicator of GFR — it does not rise until approximately 50% of nephron function is lost, and there is a further 24–48 hour lag before the accumulated creatinine equilibrates in the body water. This means that a patient can have severe ongoing AKI with a creatinine that looks 'mildly elevated'. The converse is equally dangerous: in a frail, elderly woman with low muscle mass, a creatinine of 1.4 mg/dL may represent a GFR of only 25–30 mL/min — well within Stage 3 AKI territory. Always contextualise creatinine against the patient's baseline and against urine output. An elderly woman with creatinine rising from 0.6 to 1.4 mg/dL in 24 hours with oliguric urine output represents a critical emergency, not a 'mild' creatinine elevation.
Self-Assessment: AKI Case Integration
By this point in the module you have covered the KDIGO definition and staging, the three-category classification, the pathophysiology of ATN in both its ischaemic and nephrotoxic forms, the four clinical phases and their management implications, and the priority management steps including the AEIOU indications for dialysis. The self-assessment scenarios below test your ability to integrate this knowledge in a clinically realistic way, applying the framework rather than recalling isolated facts. For each scenario, work through the reasoning before reading the analysis — this active retrieval practice deepens retention more effectively than passive re-reading. The three scenarios are deliberately chosen to span the full classification — nephrotoxic intrinsic AKI, contrast-induced ATN in a euvolaemic patient, and obstructive post-renal AKI — because the single most common error in AKI management is treating all three as if they were pre-renal volume depletion and giving fluids indiscriminately. Each scenario requires you to determine the KDIGO stage, identify the category, select the most critical intervention, and anticipate complications of recovery.
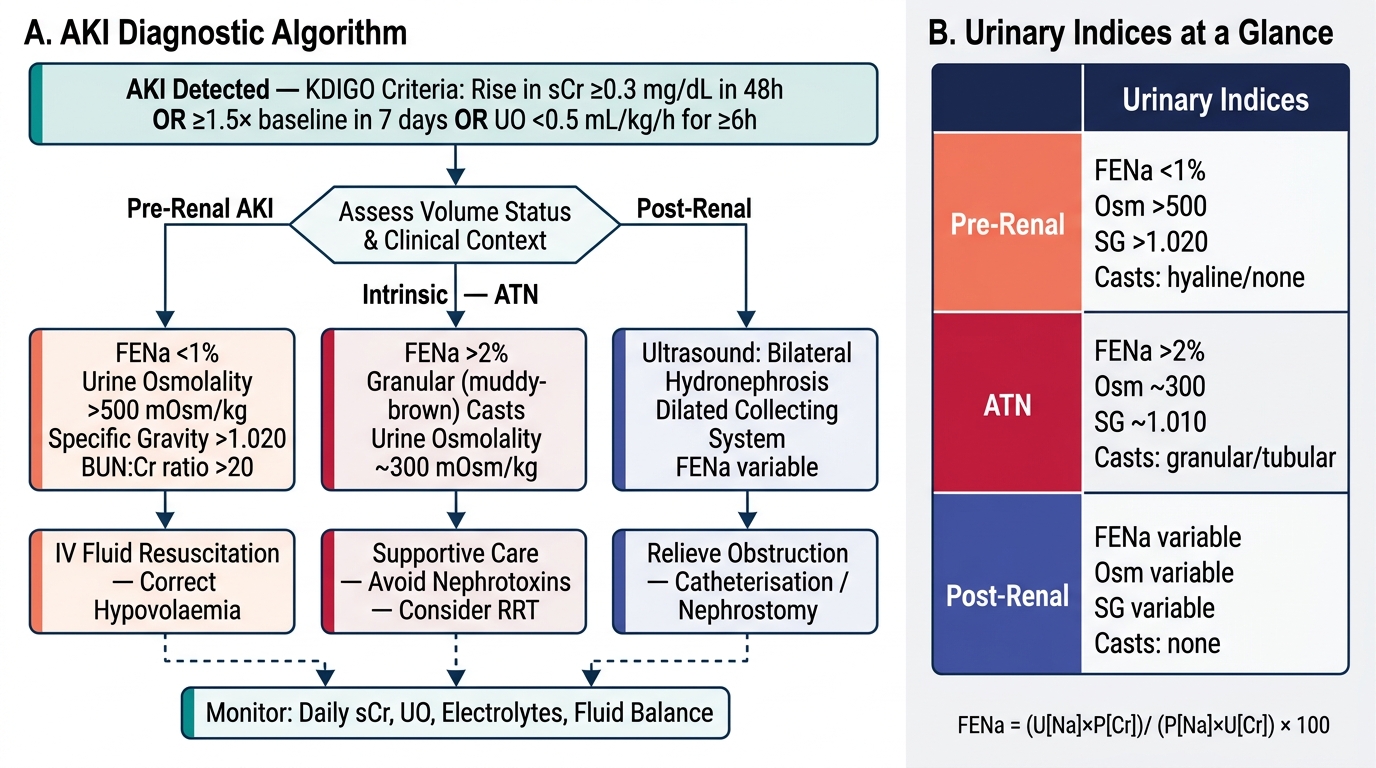
AKI Diagnostic Algorithm and Urinary Indices
Scenario A: A 45-year-old man was admitted 2 days ago for community-acquired pneumonia and started on gentamicin. Today his creatinine has risen from 0.9 to 2.3 mg/dL. BP is 120/80 mmHg, he is euvolaemic, and urine output is 40 mL/h. Urinalysis shows granular casts and tubular epithelial cell casts. What is the diagnosis, KDIGO stage, and most critical management step?
Analysis: KDIGO Stage 2 (creatinine 2.3 vs baseline 0.9 = 2.6× baseline). Euvolaemic excludes pre-renal; granular and tubular epithelial casts = ATN. Cause = nephrotoxic ATN from gentamicin. Most critical step = STOP GENTAMICIN immediately. Switch to an alternative antibiotic. Do not add further nephrotoxins (avoid NSAIDs, contrast). Supportive management: fluid balance, electrolyte monitoring, dose adjustment of other medications. Nephrology consult for monitoring.
Scenario B: A 65-year-old diabetic woman presents with 48 hours of decreased urine output after a CT angiogram with iodinated contrast. Her creatinine has risen from 1.2 to 3.5 mg/dL. She has no peripheral oedema, her JVP is normal, and her urine shows muddy-brown casts with fine granular casts. Should she receive IV fluids?
Analysis: KDIGO Stage 2–3 (3.5/1.2 = 2.9×). Post-contrast ATN — mechanism is medullary vasoconstriction + tubulotoxicity. Euvolaemic on examination — NOT appropriate to give aggressive IV fluids. Management: strict fluid balance (replace estimated insensible losses plus urine output), avoid further nephrotoxins, hold ACE inhibitors and NSAIDs, check electrolytes and manage hyperkalaemia if present, monitor for complications. If creatinine continues to rise with oliguria, consider nephrology input for potential CRRT. Prevention of CI-AKI: isotonic saline pre- and post-procedure in future contrast exposures, N-acetylcysteine (evidence limited).
Scenario C: A 60-year-old man with previously unknown BPH is found to have a serum creatinine of 6.8 mg/dL and bilateral hydronephrosis on ultrasound. He is alert but nauseated. His potassium is 5.2 mEq/L and his ECG shows no changes. What is the management plan?
Analysis: Post-renal AKI from bladder outlet obstruction. Immediate: urethral catheterisation. If catheter placement fails due to urethral stricture, consult urology for suprapubic catheter. After relief of obstruction, monitor closely for post-obstructive diuresis (can be 3–5 L/day) — replace urinary losses with IV saline to prevent severe dehydration and electrolyte depletion. Monitor creatinine and potassium daily. If creatinine does not recover within 1–2 weeks, consider renal biopsy to assess for superimposed intrinsic disease. Given the high creatinine, also screen for complications: repeat potassium, check acid-base status, and consider nephrology referral.