Page 11 of 23
IM10.12-16 | Renal Failure Diagnostic Testing — SDL Guide (Part 2)
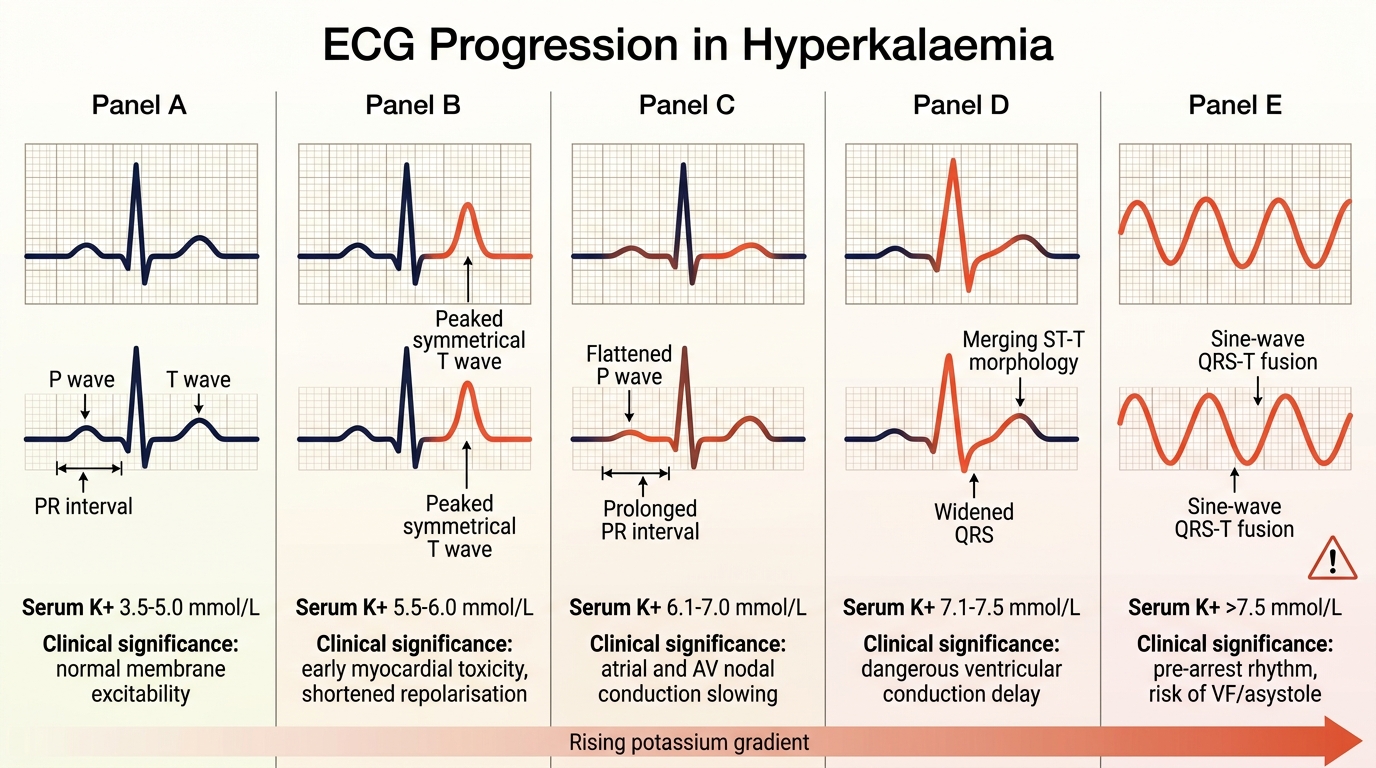
ECG Changes in Hyperkalaemia — Recognition and Severity
The recognition of ECG changes in hyperkalaemia is a life-saving skill — the ECG provides real-time information about the cardiac membrane toxicity of elevated potassium that the serum potassium level alone cannot provide. Two patients with identical potassium levels may have vastly different ECG findings depending on the rate of rise, the calcium level, and the acid-base status, which is why the ECG must be obtained simultaneously with the serum potassium in any patient with AKI/CKD and suspected hyperkalaemia.
The ECG changes in hyperkalaemia follow a progressive sequence as the serum potassium rises, though this progression is not entirely linear and individual variation exists. Understanding the mechanistic basis helps you predict and recognise each change: high extracellular potassium depolarises the resting membrane potential, slows phase 0 upstroke (conduction), shortens repolarisation (paradoxically sharpens T-waves initially), and ultimately leads to conduction block and ventricular fibrillation.
Sequence of ECG changes with rising potassium:
- K⁺ 5.5–6.0 mEq/L — Peaked T-waves: The earliest and most reliable ECG sign. T-waves become narrow-based (short duration), tall, and symmetric ('tent-shaped' or 'peaked'). Best seen in precordial leads V2–V4. This is caused by accelerated repolarisation as high extracellular K⁺ shortens the action potential duration. The height of the T-wave exceeds the R-wave in several leads. Importantly, peaked T-waves can also occur in early MI (de Winter pattern) and in normal young athletes — context matters.
- K⁺ 6.0–7.0 mEq/L — PR interval prolongation and P-wave flattening: As the atrial myocardium is affected, the PR interval lengthens (first-degree AV block), and P-waves become progressively lower in amplitude and then disappear (because atrial conduction fails — 'P-sine wave' pattern).
- K⁺ 6.5–7.5 mEq/L — QRS widening: The His-Purkinje system and ventricular myocardium begin to conduct slowly. The QRS complex broadens beyond 120 ms (normal <100 ms). This is an ominous sign indicating impending conduction failure.
- K⁺ >7.5–8.0 mEq/L — Sine-wave pattern: The widened QRS merges with the peaked T-wave to create a biphasic 'sine-wave' — a pre-terminal rhythm that is virtually pathognomonic of severe hyperkalaemia. This pattern requires IMMEDIATE membrane stabilisation with calcium gluconate and emergency dialysis.
- K⁺ >8.0–9.0 mEq/L — Ventricular fibrillation / asystole: The terminal event. The heart depolarises chaotically and the QRS becomes indistinguishable from baseline.
The threshold for immediate treatment (calcium gluconate) is any ECG change beyond peaked T-waves alone, or a K⁺ >6.5 mEq/L regardless of ECG findings. Any QRS widening = emergency — treat immediately without waiting for further investigation results. The absence of ECG changes at K⁺ 7.0 does not mean the patient is safe — ECG changes can develop suddenly and precipitously.
ECG Progression in Hyperkalaemia
SELF-CHECK
An ECG is obtained for a 65-year-old with AKI. It shows peaked, narrow-based, symmetric T-waves in leads V2–V4, with QRS duration of 140 ms and no identifiable P-waves. His potassium result is pending. Which is the MOST appropriate immediate action?
A. Wait for potassium result before acting
B. Start sodium bicarbonate 50 mEq IV
C. Give calcium gluconate 10% 10 mL IV immediately
D. Obtain repeat ECG in 30 minutes
Reveal Answer
Answer: C. Give calcium gluconate 10% 10 mL IV immediately
QRS widening (140 ms, normal <100 ms) and absent P-waves in a patient with AKI are diagnostic of severe hyperkalaemia with cardiac membrane toxicity — this is a cardiac emergency. Waiting for the potassium result is dangerous; treatment must precede it. Calcium gluconate 10% 10 mL IV is the first-line treatment — it does not lower potassium but immediately stabilises the cardiac membrane potential within 1–3 minutes. Sodium bicarbonate is an adjunct that helps shift K⁺ into cells but takes 15–30 minutes — it is not the first-priority action. Repeating the ECG delays life-saving treatment.
Renal Ultrasound, Urinalysis, and ABG Interpretation
Several key investigations beyond the serum biochemistry panel deserve detailed discussion for their interpretation at the bedside and in the examination setting. Each of the three investigations covered in this section — renal ultrasound, urinalysis with microscopy, and the arterial blood gas — answers a different and non-overlapping clinical question: the ultrasound establishes anatomy and chronicity; the urinalysis identifies the intrinsic renal compartment affected; and the ABG quantifies the acid-base disturbance and oxygenation. Together they form an essential complement to the serum biochemical panel, and their integration — not their individual results in isolation — is what allows the clinician to classify the AKI category definitively, assess severity, and make urgent management decisions. Each investigation must be actively ordered based on the clinical hypothesis, and each result must be interpreted in the context of all other available information.
Renal ultrasound is the single most informative imaging investigation in renal failure. It should be obtained in every patient with AKI of uncertain cause and in all patients with newly discovered CKD. The key ultrasound findings and their clinical significance are:
- Kidney size: Normal adult kidney length = 9–12 cm (approximately 3 lumbar vertebrae heights). Small kidneys (<9 cm) with increased echogenicity and thinned cortex = chronic irreversible damage — confirms CKD. Normal or enlarged kidneys in AKI = consistent with AKI (kidneys may be oedematous and swollen), but also with infiltrative conditions: diabetes (normal or mildly enlarged kidneys even in diabetic nephropathy), amyloidosis (bilateral renal enlargement), and polycystic kidney disease (bilateral cystic enlargement — often dramatically so, kidneys may reach 20–30 cm).
- Cortical echogenicity: Normal = less echogenic than the adjacent liver or spleen. Increased cortical echogenicity = loss of normal corticomedullary differentiation = interstitial fibrosis and tubular atrophy = chronic damage. Bilaterally small, hyperechoic kidneys = CKD (irreversible).
- Hydronephrosis: Dilatation of the renal pelvis and calyces (grade 1–4 by severity) = obstruction to urine outflow. Presence of bilateral hydronephrosis in an anuric patient confirms post-renal AKI. Unilateral hydronephrosis = obstructed single kidney or contralateral non-functional kidney. Important: the absence of hydronephrosis does NOT exclude obstruction early in acute obstruction (the collecting system has not had time to dilate).
- Urinary bladder assessment: A distended bladder on ultrasound (post-void residual >100–150 mL or bladder full despite apparent anuria) confirms bladder outlet obstruction.
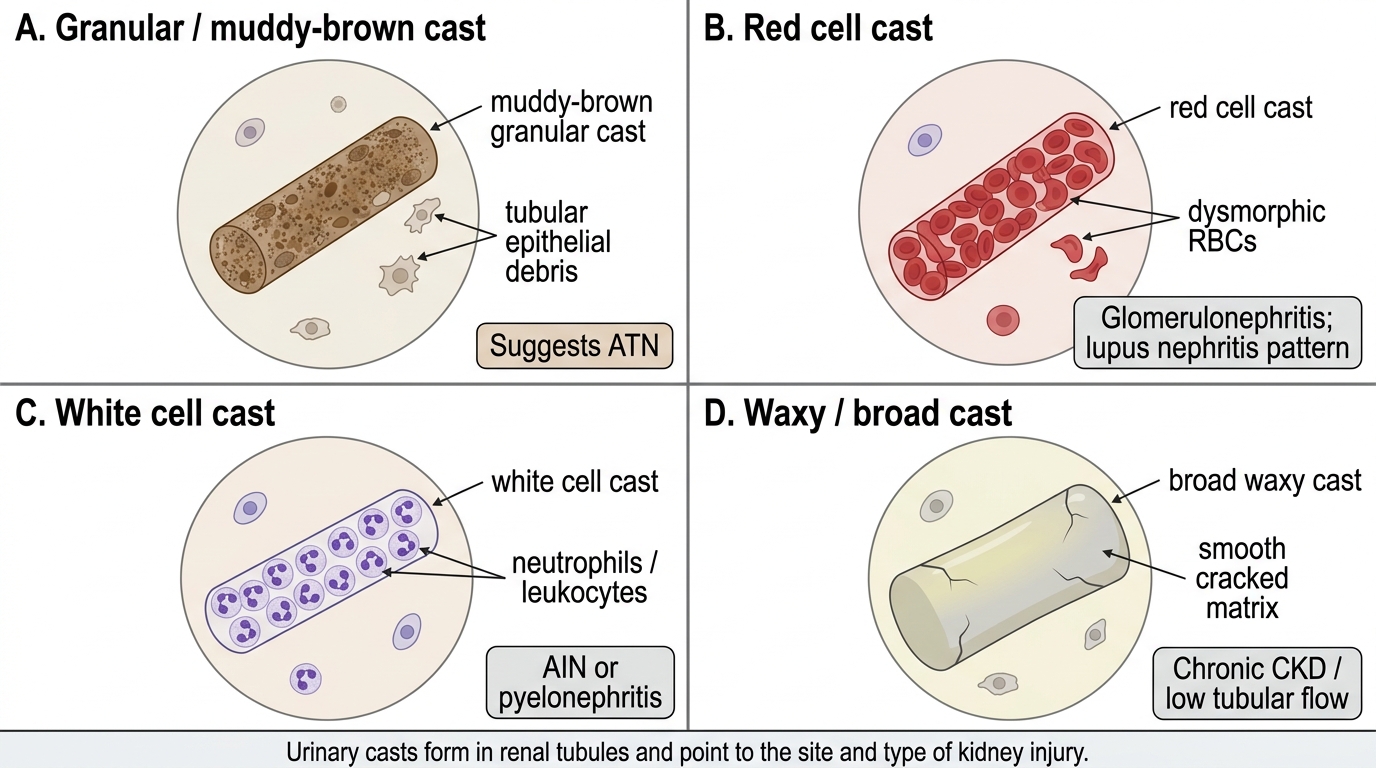
Urinalysis with microscopy provides critical information about the nature of the intrinsic renal injury:
- Granular casts (muddy brown casts): composed of degenerated tubular epithelial cells and cellular debris; classic for ATN. The presence of these casts in a patient with AKI and a clinical picture of nephrotoxin exposure or prolonged hypotension confirms intrinsic tubular injury.
- Red cell casts: pathognomonic of glomerulonephritis. Red cells pass through the damaged glomerular basement membrane and are moulded into casts in the Tamm-Horsfall protein matrix of the distal tubule. Their presence mandates immunological workup for GN.
- White cell casts and eosinophiluria: suggests acute interstitial nephritis (AIN) or pyelonephritis. Eosinophiluria detected by Hansel stain supports drug-induced AIN, though its sensitivity and specificity are limited.
- Waxy casts and broad casts: composed of highly inspissated material; indicate chronic severe tubular atrophy and are a marker of advanced CKD (renal failure casts).
- Proteinuria: quantified by ACR; ≥3.5 g/24 h (or ACR ≥3500 mg/g) = nephrotic range. Massive proteinuria with haematuria and casts = nephritic-nephrotic overlap (membranoproliferative GN, lupus).
Arterial blood gas (ABG) interpretation in renal failure: The ABG provides pH, PaCO₂, PaO₂, bicarbonate, and calculated base excess. In AKI/CKD the expected finding is metabolic acidosis (low pH, low HCO₃⁻) with appropriate respiratory compensation (low PaCO₂ — the Kussmaul breathing drives CO₂ down). The Winter formula predicts the expected PaCO₂ for a pure metabolic acidosis: expected PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2. If the actual PaCO₂ is higher than expected, there is superimposed respiratory acidosis (the patient cannot compensate adequately — signalling respiratory failure). If the actual PaCO₂ is lower than expected, there is a superimposed respiratory alkalosis (sepsis, anxiety, PE). The ABG also reveals hypoxia (PaO₂ <60 mmHg = type 1 respiratory failure — often from pulmonary oedema in volume-overloaded AKI) and the oxygen saturation in haemoglobin (SpO₂) with greater precision than the oximeter in acidaemic, cold, or poorly perfused patients.
Urinary Cast Identification in Kidney Disease
SELF-CHECK
A 50-year-old woman with known SLE develops AKI. Urinalysis microscopy shows dysmorphic red blood cells and red cell casts. Her complement C3 is low. Which diagnosis does this investigation pattern MOST strongly support?
A. Acute tubular necrosis from nephrotoxic drug
B. Obstructive uropathy from retroperitoneal lymphadenopathy
C. Lupus nephritis (proliferative glomerulonephritis)
D. Acute interstitial nephritis from NSAID use
Reveal Answer
Answer: C. Lupus nephritis (proliferative glomerulonephritis)
Red cell casts on urinalysis are pathognomonic of glomerulonephritis — they indicate that red blood cells have crossed the damaged glomerular filtration barrier and been moulded into casts. In the context of known SLE, dysmorphic RBCs + red cell casts + low C3 (complement consumption in immune complex-mediated GN) strongly confirms lupus nephritis (class III/IV proliferative GN). ATN produces granular (muddy brown) casts, not red cell casts. Obstructive uropathy produces no casts. AIN may produce white cell casts and eosinophiluria. The combination of red cell casts + low C3 in a lupus patient mandates urgent renal biopsy for class determination and immunosuppression.
Applied Practice — Procedural Skills: ABG and IV Catheter
Two practical procedural competencies — arterial blood gas sampling (IM10.15) and peripheral intravenous catheter insertion (IM10.16) — are embedded within the renal failure management context and are assessed at the P (Practical skill) level. These skills must be learned and practised in the clinical skills laboratory and on supervised clinical placements.
Provided image
Arterial Blood Gas Sampling (IM10.15 — Procedural):
The ABG is sampled from a peripheral artery — most commonly the radial artery at the wrist (preferred because of its accessibility and collateral circulation via the ulnar artery). Less commonly the brachial artery (no reliable collateral — higher risk) or femoral artery (used in emergency when peripheral arteries are not palpable) are used. Before sampling from the radial artery, the Allen's test should be performed to confirm ulnar collateral flow: compress both radial and ulnar arteries at the wrist; ask the patient to open and close the fist rapidly until the palm blanches (blood expelled); release the ulnar artery only; normal Allen's test = palm flushes within 5–10 seconds (adequate ulnar collateral). A positive Allen's test (flush within 5–10 s) confirms it is safe to use the radial artery.
Procedure: palpate the radial artery at the wrist with the wrist dorsiflexed over a roll of gauze; clean with antiseptic; insert a pre-heparinised syringe (dedicated ABG syringe with pre-filled heparin to prevent clotting) at a 45° angle (some practitioners use 30–60°) with the bevel up, advancing until arterial flashback (bright red pulsatile blood) enters the syringe. Collect 1–2 mL. Remove needle; apply firm pressure for at least 5 minutes (longer in patients on anticoagulants or with thrombocytopenia). Transport the syringe on ice (or analyse within 30 minutes) to prevent cellular oxygen consumption from falsely lowering the measured PaO₂. Document the FiO₂ at the time of sampling (arterial PO₂ cannot be interpreted without knowing the inspired oxygen fraction).
Indications for ABG in renal failure: dyspnoea or SpO₂ <92%, Kussmaul breathing (to quantify acidaemia), confusion of uncertain cause, and pre-dialysis assessment.
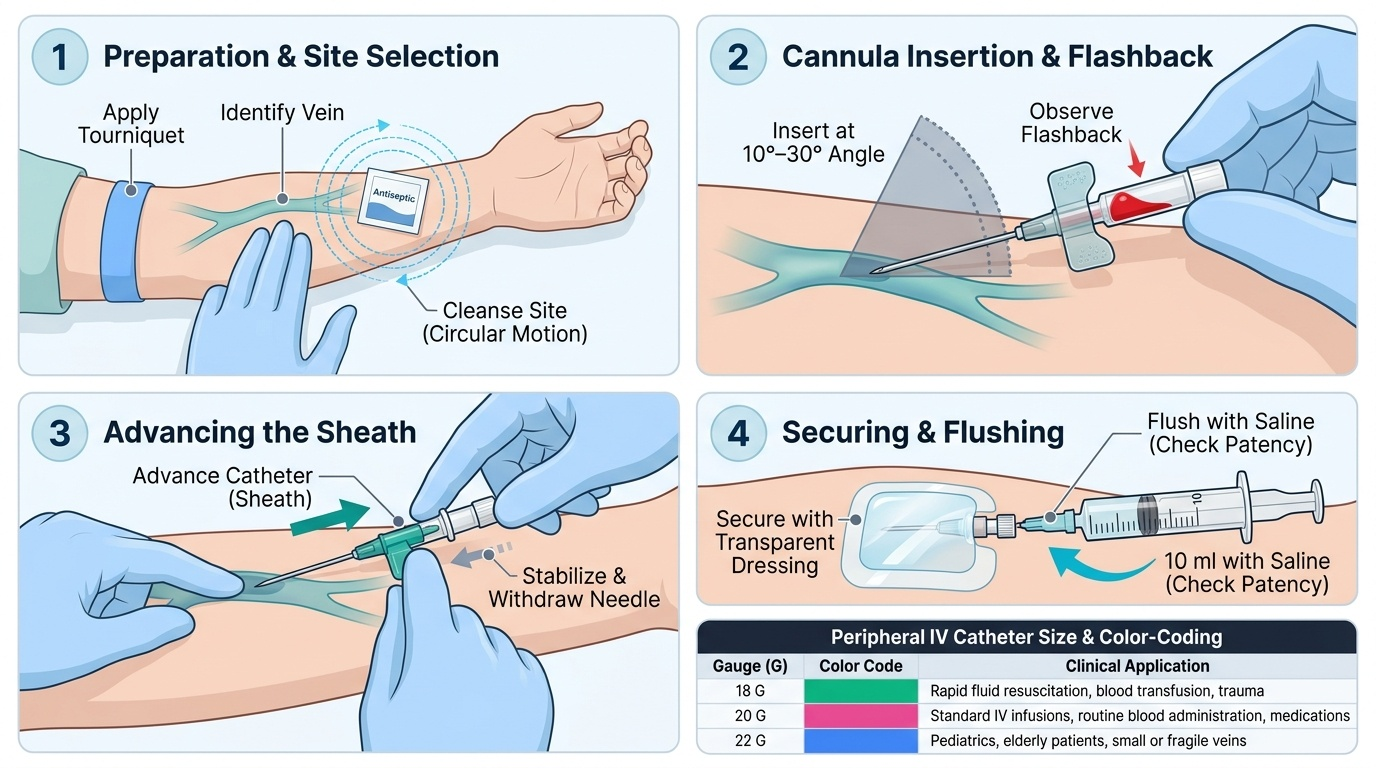
Peripheral IV Catheter Insertion (IM10.16 — Procedural):
Peripheral IV access is essential in AKI management for: fluid resuscitation (isotonic crystalloid), IV medications (calcium gluconate, insulin-dextrose, IV furosemide, IV antibiotics), and blood sampling when venepuncture sites are exhausted. Preferred sites in order: dorsum of hand (24G or 22G for non-urgent access), antecubital fossa (18G or 20G, for rapid fluid administration or blood products), and forearm cephalic or basilic vein. Avoid sites near infected skin, previous thrombophlebitis, the ipsilateral arm after axillary node dissection, and the arm with an existing AV fistula in a dialysis patient (occlusion can be catastrophic for vascular access).
Procedure: apply a tourniquet proximal to the site; clean with 70% isopropyl alcohol swab; introduce the cannula at a 10–30° angle (bevel up); advance until flashback is seen in the cannula hub; lower the angle and advance the cannula (sheath) over the needle into the vein while holding the needle still; release tourniquet; withdraw the needle while applying pressure distal to the tip; attach IV tubing or a needleless connector cap; secure with a transparent dressing. Confirm patency with a 5–10 mL saline flush — check for free flow and absence of swelling (which would indicate extravasation into subcutaneous tissue).
Size selection: 18G (green) for rapid fluid administration; 20G (pink) for routine medications; 22G (blue) for elderly or fragile veins. Cannulas must be resited every 72–96 hours (or earlier if signs of phlebitis — pain, redness, induration along the vein course).
CLINICAL PEARL
The FENa is powerful but has a critical caveat that many clinicians overlook: it is invalid when the patient has recently received a loop or thiazide diuretic. Diuretics force sodium excretion, raising the urine sodium and FENa to >2% even in a volume-depleted patient with pre-renal AKI — giving the false impression of ATN. In this situation, use the fractional excretion of urea (FEUrea): FEUrea = [(urine urea × plasma creatinine) / (plasma urea × urine creatinine)] × 100. Urea reabsorption is not directly affected by diuretics. An FEUrea <35% indicates pre-renal AKI (avid proximal tubular urea reabsorption) even in the diuretic-treated patient. This distinction determines whether to give IV fluids (pre-renal → give), or continue supportive management for ATN (withhold excess fluids). Getting it wrong in a volume-overloaded diuretic-treated patient who actually has ATN — and giving fluids because the FENa says >2% — results in pulmonary oedema.
Self-Assessment — Diagnostic Integration Scenarios
The self-assessment scenarios below require you to integrate multiple investigation results and generate a coherent interpretation — linking each result to its clinical significance, the underlying mechanism, and the management implication it triggers. This is the synthesis skill assessed in the IM10.12–10.16 competency domain. For each scenario, work through the investigation interpretation systematically before reading the analysis. Remember that no single test should be interpreted in isolation — the pattern of results, read against the clinical background, is what makes the diagnosis. The three scenarios below are deliberately chosen to span the full range: Scenario A tests the FENa calculation and pre-renal identification; Scenario B tests ATN recognition from granular casts plus ABG acid-base analysis; and Scenario C tests life-threatening hyperkalaemia ECG recognition in CKD. In each case, the clinical action that follows from the investigation interpretation is as important as the interpretation itself — the test exists to change management, not merely to classify. Work methodically: classify the AKI category, calculate any derived index, read the ECG pattern, apply the Winter formula where appropriate, and identify the two most urgent management actions before reading the analysis.
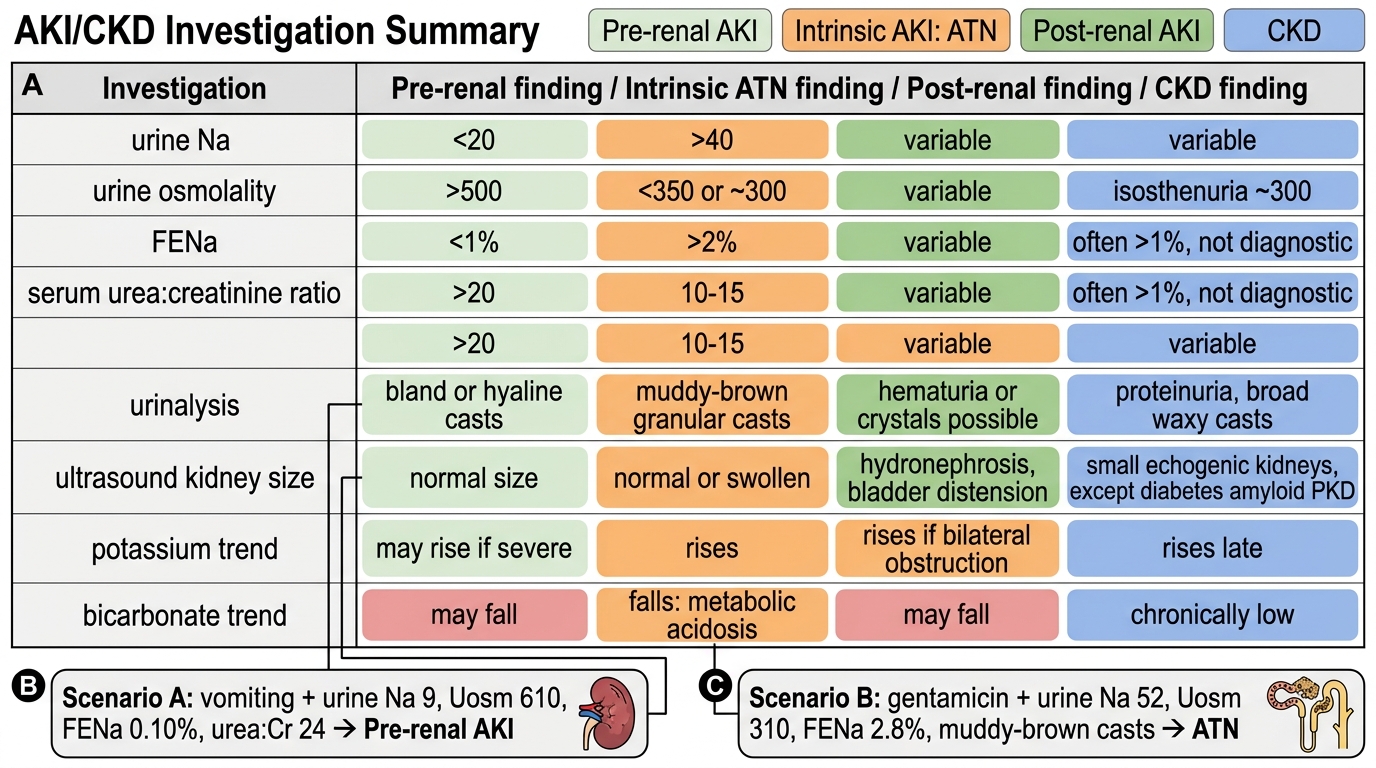
AKI and CKD Investigation Summary
Scenario A: A 55-year-old man with three-day history of vomiting is found to have creatinine 2.8 mg/dL. Results: urine Na 9 mEq/L, urine osmolality 610 mOsm/kg, serum Na 142 mEq/L, serum creatinine 2.8 mg/dL, urine creatinine 180 mg/dL. Urea:creatinine ratio (serum) = 24. ECG: peaked T-waves in V3–V4, normal QRS, P-waves present, PR 160 ms. Potassium 5.8 mEq/L.
Analysis: FENa = [(9 × 2.8) / (142 × 180)] × 100 = [25.2 / 25,560] × 100 = 0.10% → pre-renal AKI. High urine osmolality and low urine Na confirm intact tubular conservation. Urea:creatinine ratio 24 (>20) = pre-renal. Potassium 5.8 with peaked T-waves (no QRS widening, P-waves present) = Stage 1 hyperkalaemia on ECG — monitor, restrict dietary K⁺, treat cause (volume resuscitation). Management: IV isotonic saline to restore volume; reassess creatinine and potassium in 4–6 hours; stop any nephrotoxic drugs.
Scenario B: A 68-year-old man post-sigmoid colectomy (Day 3) has creatinine rising from 0.9 to 3.4 mg/dL. He received gentamicin for perioperative prophylaxis. Urine Na 52 mEq/L, urine osmolality 310 mOsm/kg, FENa 2.8%. Urinalysis: granular muddy-brown casts +++. ABG: pH 7.23, HCO₃⁻ 12 mEq/L, PaCO₂ 28 mmHg. K⁺ 5.9 mEq/L. ECG: peaked T-waves only.
Analysis: FENa >2% + granular casts = established ATN from gentamicin nephrotoxicity. High urine Na + low osmolality = tubular dysfunction confirmed. ABG: metabolic acidosis (low pH, low HCO₃⁻); expected PaCO₂ = 1.5 × 12 + 8 = 26 ± 2 → measured 28 = adequate respiratory compensation, pure metabolic acidosis. Anion gap = Na − (Cl + HCO₃⁻) — need Cl to calculate, but HCO₃⁻ 12 indicates significant acidaemia. Management: STOP gentamicin; supportive care; strict fluid balance; monitor K⁺ and ECG; consider bicarbonate supplementation if HCO₃⁻ falls below 12; nephrology consult for potential RRT if pH falls below 7.1.
Scenario C: A 72-year-old with CKD G4 has the following results: K⁺ 7.2 mEq/L, HCO₃⁻ 14 mEq/L, calcium 7.8 mg/dL (corrected 8.4), phosphate 7.1 mg/dL, PTH 680 pg/mL, Hb 8.6 g/dL. ECG shows broad QRS (150 ms), absent P-waves, and merged QRS-T (sine-wave morphology). What are the two most urgent actions?
Analysis: (1) Immediate calcium gluconate 10% 10 mL IV — sine-wave pattern on ECG with K⁺ 7.2 = life-threatening hyperkalaemia requiring immediate membrane stabilisation. (2) Emergency haemodialysis — the combination of severe hyperkalaemia refractory to medical management (sine-wave ECG), metabolic acidosis driving further K⁺ elevation, and a CKD G4 patient without residual diuresis = AEIOU met for E (electrolyte) and A (acidosis). The chronic CKD-MBD findings (high phosphate, high PTH, high Ca×PO₄ product, anaemia) require management but are not the immediate priorities in this crisis presentation.