Page 14 of 23
IM11.19-20 | Diabetes Patient Skills and Counselling — SDL Guide (Part 2)
Interpretation of Findings and Common Counselling Scenarios
Interpreting the findings from insulin technique assessment and SMBG in clinical practice requires pattern recognition and the ability to connect a clinical sign (e.g., lipohypertrophy, erratic fasting glucose) to its underlying technical cause. This section covers the most clinically important counselling scenarios arising from these two skills, building the applied practice competency required at final-year level.
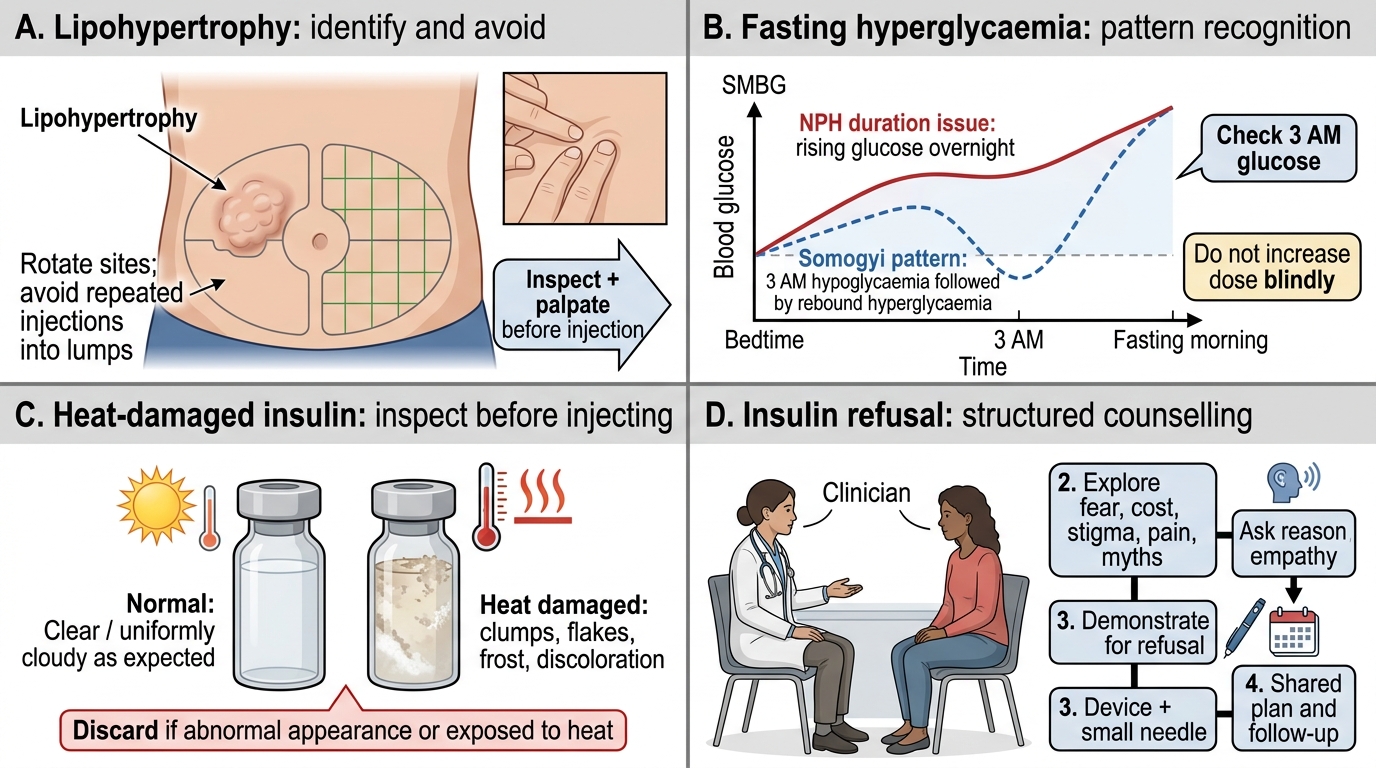
Counselling Scenario 1 — Discovering Lipohypertrophy:
You examine a patient's injection sites and find a firm, doughy area on the right lateral abdomen, approximately 5 × 4 cm, that the patient says is 'comfortable to inject into — it barely hurts.' This is the classic picture: lipohypertrophy is painless because the nerve endings within the fatty deposit are reduced, which perversely makes it the preferred injection site — exactly the wrong site to use. Counsel the patient that: (1) injecting into this area causes unpredictable insulin absorption and explains their erratic glucose readings; (2) this site must be completely avoided until the lump resolves (which can take 6–12 months); (3) a strict rotation protocol must be implemented immediately; and (4) when switching to healthy tissue, glucose may initially fall and insulin dose may need temporary reduction to prevent hypoglycaemia. Document the location, size, and texture of the lipohypertrophy.
Counselling Scenario 2 — Fasting Hyperglycaemia Despite Bedtime Insulin:
A patient on NPH 22 units at bedtime has consistently elevated fasting glucose (165–190 mg/dL) but good midday glucose. Two mechanisms can cause this: (1) Insufficient basal insulin: NPH action has worn off by the early morning (NPH duration only 12–18 hours); solution — switch to long-acting analogue (glargine, degludec) or split NPH dose. (2) Somogyi effect (rebound hyperglycaemia): Nocturnal hypoglycaemia (from peak NPH effect at 4–6 hours) triggers counter-regulatory hormone surge, causing rebound fasting hyperglycaemia; solution — check 3 am glucose to detect nocturnal hypoglycaemia; if present, reduce NPH dose. Distinguish these two by instructing the patient to check glucose at 3 am on two occasions: if 3 am glucose is low → Somogyi effect (reduce dose); if 3 am glucose is normal or high → insufficient insulin (increase dose or switch to analogue).
Counselling Scenario 3 — Unexplained Hyperglycaemia After Starting Insulin:
A patient reports that her glucose is not improving at all despite insulin. On history: she is injecting in the same site every time (no rotation); she stores her insulin in a bag that gets hot in the Chennai afternoon sun (above 37°C). Both errors — lipohypertrophy from no rotation AND heat-damaged insulin with reduced potency — can produce apparent insulin failure. Assessment: inspect injection sites; ask about storage; examine the insulin pen (has the insulin changed in appearance — cloudiness in a normally clear insulin = denaturation). Change the insulin vial/pen; institute rotation; teach cold-chain storage.
Counselling Scenario 4 — Patient Refusing Insulin:
A 62-year-old T2DM patient with HbA1c 10.2% refuses insulin citing fear of injections. Structured counselling approach: (1) Acknowledge the concern (injection anxiety is valid and very common — do not dismiss it); (2) Explain what insulin does and why it is needed now (his beta cells are exhausted, not that he has 'failed'); (3) Use the modern pen needle (4 mm, 32 gauge) — demonstrate on a willing patient or model if possible; (4) Discuss that many patients report injection is less painful than a mosquito bite with modern pen needles; (5) Offer to observe the first injection in clinic; (6) Explain that the goal is to avoid the serious complications of ongoing very high glucose (nerve damage, kidney failure, blindness) — these are far more disabling than an injection. Document the counselling conversation and the patient's reasons for refusal.
Applied Insulin Counselling: Technique, Patterns, Safety, and Refusal
Applied Practice: Integrating Technique with Clinical Outcomes
The applied practice level for insulin injection and SMBG skills requires you to integrate technical knowledge with clinical outcome data to identify and correct the cause of glycaemic failure, conduct a structured skills assessment of a patient's technique, and provide actionable counselling. These are not isolated procedural skills — they form the interface between the prescription and the clinical outcome, and bridging that interface is what distinguishes a clinician who prescribes from one who ensures the prescription actually works. In diabetes practice, unexpected glycaemic failure on insulin is one of the most common clinical situations you will encounter, and the instinctive response — increase the dose — is often wrong and sometimes dangerous. A systematic evaluation of the injection technique reveals the true cause in the majority of cases, as published studies have consistently found that 50–80% of insulin users have at least one identifiable technique error when their practice is formally observed. The framework below structures this evaluation into a logical, reproducible sequence that can be completed in a 10–15 minute clinical encounter, without any equipment beyond your own hands and a willingness to watch the patient actually perform the injection rather than accepting a verbal description of what they claim to do. Verbal descriptions of injection technique are notoriously unreliable — patients believe they are injecting correctly and will say so honestly; the error is in the execution, which they cannot self-identify without being shown.
Provided image
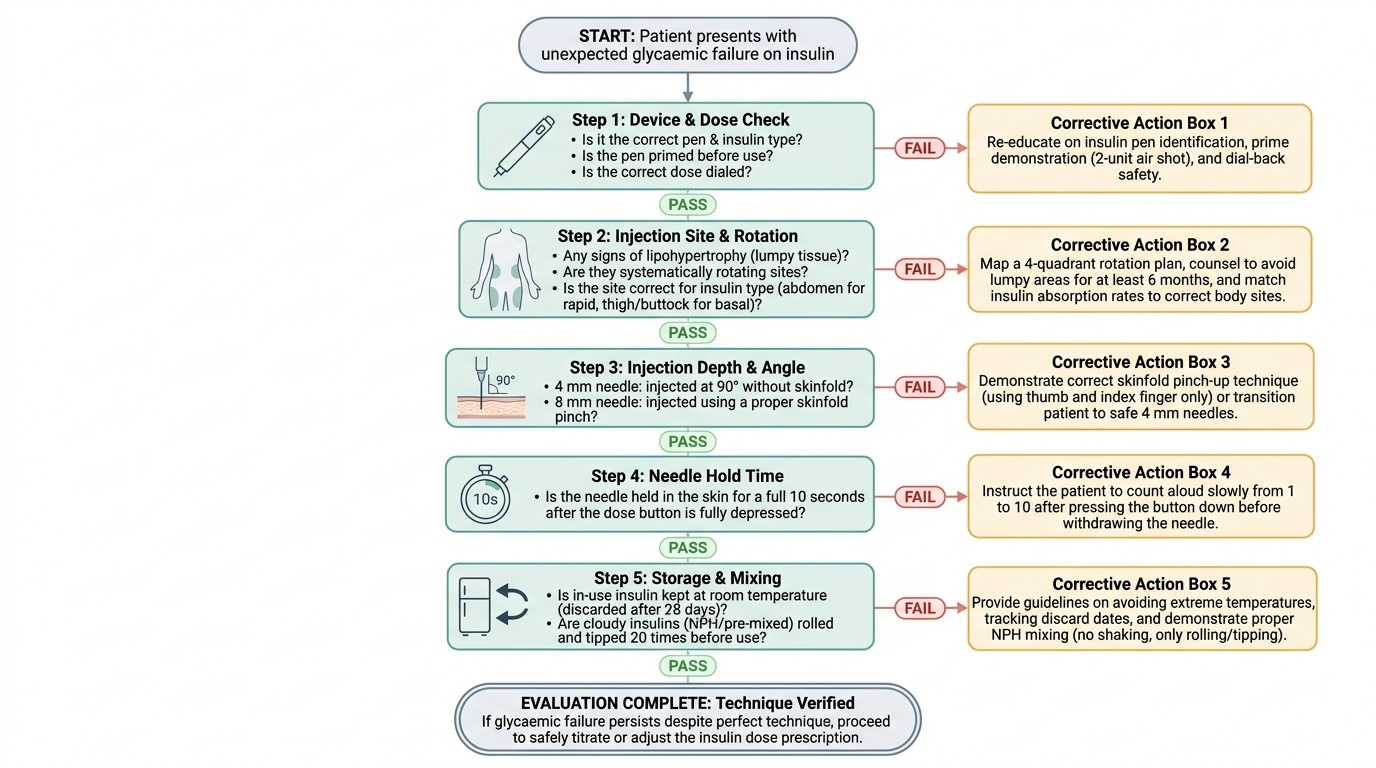
A framework for evaluating insulin technique failure:
When a patient's glucose control on insulin is unexpectedly poor, work through the following checklist before concluding that the dose needs to be increased:
1. Device check: Is the patient using the correct pen and correct insulin type? Have they primed the pen? Are they dialling the correct dose?
2. Injection site: Any lipohypertrophy? Are they rotating? Is the site appropriate for the insulin type (abdomen for rapid, thigh/buttock for basal)?
3. Injection depth: Are they using a skinfold with an 8 mm needle? Are they injecting at 90° with a 4 mm needle?
4. Hold time: Are they holding the needle in for 10 seconds after pressing the button fully?
5. Storage: Is insulin being stored correctly? Any exposure to heat or freezing? When was the vial/cartridge opened — is it past the 28-day in-use limit?
6. Mixing: If on NPH — are they rolling (not shaking) to resuspend? Are they mixing insulin types inappropriately?
A structured practical skills assessment session in clinic (10–15 minutes) using the above checklist will identify technique errors in the majority of patients with unexplained insulin failure. Studies show 50–80% of patients on insulin have detectable injection technique errors when formally assessed.
SMBG data review in clinic:
At every clinic visit for a patient on SMBG, review the logbook or glucometer download. Look for:
- Pattern of fasting glucose (guides basal insulin titration)
- Pattern of postprandial glucose (guides rapid-acting insulin dose or carbohydrate restriction)
- Frequency and timing of hypoglycaemia (<70 mg/dL) — raises the question of reducing SU or insulin dose
- Glucose variability (high variability despite good average HbA1c = patient is oscillating between hypo and hyper — common with NPH, erratic injection technique, irregular meals)
- 3 am checks if nocturnal hypoglycaemia is suspected
Transition from multiple daily injections to a simplified regimen:
For elderly, frail, or cognitively impaired patients who cannot manage a complex MDI regimen, a simplified approach may be more appropriate: once-daily basal insulin + oral agents, or twice-daily premixed insulin. Counselling must be tailored to the patient's capacity — simplified regimens with clear instructions and a caregiver involved in training are appropriate. Fixed-dose combinations (FDC pens combining GLP-1 RA + basal insulin, such as insulin degludec/liraglutide — IDegLira) reduce injection frequency to once daily while covering both basal and postprandial glucose, and are becoming available in India.
SELF-CHECK
A 50-year-old T2DM patient performs SMBG at home. She shows you her logbook: fasting glucose 88–102 mg/dL (excellent). However, post-dinner glucose is consistently 210–260 mg/dL. She is on metformin 1 g twice daily and basal insulin glargine 16 units at bedtime. What is the MOST appropriate next step?
A. Increase glargine to 20 units — the overall glycaemic control is suboptimal
B. Add a rapid-acting insulin analogue before dinner to control the postprandial spike
C. Switch to premixed 30/70 insulin twice daily to cover both fasting and meal glucose
D. Add an SGLT2 inhibitor — it will reduce postprandial hyperglycaemia without hypoglycaemia risk
Reveal Answer
Answer: B. Add a rapid-acting insulin analogue before dinner to control the postprandial spike
The SMBG pattern shows excellent fasting control (basal insulin is working well — no need to increase glargine) with persistent postprandial hyperglycaemia after dinner. This is a classic 'basal-adequate, prandial-inadequate' pattern. The appropriate next step is to add a rapid-acting insulin analogue (lispro, aspart, or glulisine) before the evening meal to cover the dinner carbohydrate load — this is the start of a basal-bolus regimen. Increasing glargine will lower overnight/fasting glucose further but cannot address postprandial spikes. Switching to premixed 30/70 changes the whole regimen unnecessarily. An SGLT2 inhibitor is reasonable but the magnitude of postprandial reduction is modest (10–15 mg/dL postprandially) compared to rapid-acting insulin which can reduce this spike by 50–80 mg/dL.
Self-Assessment: Applying Patient Skills Competencies
The patient skills competencies IM11.19 and IM11.20 are assessed in two ways in clinical practice: direct observation of the patient's technique (which you supervise and correct) and the ability to teach and counsel the patient correctly when errors are identified. The self-assessment scenarios below require you to apply both levels of this competency — diagnosis of the technical problem and the communication of the correction.
Scenario A: Vijay, a 35-year-old T1DM patient on a basal-bolus regimen, reports that his post-breakfast glucose is consistently high (200–240 mg/dL) despite what he says is '10 units of rapid-acting insulin before breakfast.' You ask him to demonstrate his injection technique. He dials the pen to 10 units, places the needle against his abdomen, presses the button fully, and immediately removes the pen. He then removes the needle cap from the pen and places the used needle back in the same cap. What are the two injection errors you have observed, and what are their consequences?
Analysis: Error 1: He removed the pen within 1–2 seconds of pressing the injection button — he did not wait the required 10 seconds. This results in leakage of insulin back out through the needle track after withdrawal, losing part of the dose. Consequence: systematic underdosing, explaining the persistent postprandial hyperglycaemia despite 'correct' dosing. Error 2: He recapped the used needle — needle reuse leads to blunting and barbing of the needle tip, increasing lipohypertrophy risk and pain with subsequent injections. Correction for error 1: demonstrate the 10-second hold with visible compression of the injection button; have him count aloud. Correction for error 2: use a new needle for every injection; dispose of used needles in sharps container.
Scenario B: Leela, a 65-year-old T2DM patient on once-daily glargine, brings her glucometer for you to review. Her glucose log shows: fasting glucose ranging from 78 to 195 mg/dL on different days — extremely variable — while her HbA1c is 8.2%. You examine her abdomen and find a single firm lipohypertrophic area on the right side (approximately 4 cm × 4 cm). She says she always injects 'in the same comfortable spot on the right.' What is the primary cause of the variability and how do you counsel her?
Analysis: The lipohypertrophic area causes variable insulin absorption — on injections into healthy tissue, glargine is absorbed predictably; on injections into the lipohypertrophic nodule, absorption is delayed and erratic. This explains the wide day-to-day fasting variability despite consistent dosing. Counselling: (1) explain the physiology of lipohypertrophy in plain terms (the tissue has been changed by repeated insulin injections and no longer absorbs insulin reliably); (2) instruct her to completely avoid the affected area; (3) teach the abdominal grid rotation system — divide the right and left abdomen into imaginary zones and use one zone per day in sequence; (4) warn that glucose may drop after switching to healthy tissue (insulin now absorbed better) — may need temporary dose reduction.
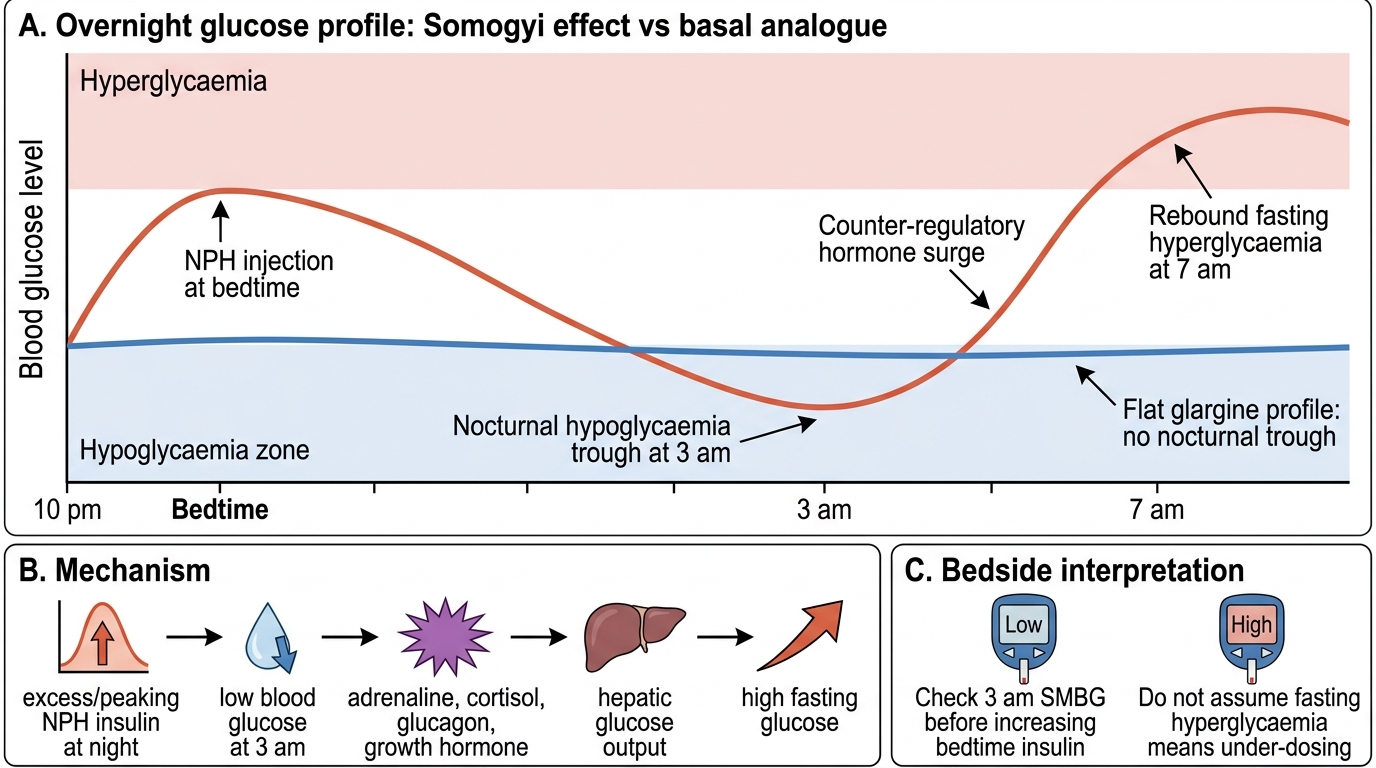
Scenario C: Raju, 48-year-old T2DM patient on insulin NPH 30 units at bedtime, checks glucose at 3 am on your instruction after you notice fasting glucose is consistently 180–200 mg/dL. His 3 am result is 42 mg/dL — he was asymptomatic. He then records fasting glucose of 195 mg/dL at 7 am. What phenomenon is occurring and what should you advise?
Analysis: This is the Somogyi effect (rebound hyperglycaemia from nocturnal hypoglycaemia): NPH peaks at 4–8 hours post-injection, causing hypoglycaemia at 3 am; the hypoglycaemia triggers a counter-regulatory hormone surge (glucagon, adrenaline, cortisol) causing rebound hyperglycaemia by 7 am. The patient was asymptomatic at 3 am because of hypoglycaemia unawareness. Management: reduce the NPH dose (by 10–20%), or switch to a long-acting basal analogue (glargine or degludec) which has no pronounced peak and eliminates this nocturnal peak-related hypoglycaemia.
Somogyi Effect: Overnight Glucose Curve
CLINICAL PEARL
Three high-yield clinical pearls for insulin technique and SMBG:
- Lipohypertrophy is painless and therefore undetected by the patient — always examine injection sites. A patient who says 'I inject in the same comfortable spot' has lipohypertrophy until proven otherwise. It is present in up to 30–40% of insulin-using patients in clinical audits, and is the most underdiagnosed cause of insulin failure. Examine and palpate injection sites at every annual review.
- The 10-second hold is the single most commonly performed injection error. Studies show that premature needle withdrawal (within 1–2 seconds) loses up to 30–40% of the injected dose. Teach this step explicitly and ask the patient to demonstrate it in front of you before leaving the clinic.
- Fasting hyperglycaemia despite insulin is NOT always a dose problem. Before increasing the dose, always exclude: lipohypertrophy (erratic absorption), insufficient NPH duration (switch to analogue), Somogyi effect (nocturnal hypo at 3 am), heat-damaged insulin, and incorrect injection technique. Increasing the dose without resolving the technical issue may cause severe hypoglycaemia once technique is corrected.