Page 4 of 17
IM12.4-7 | Thyroid Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit a structured and relevant thyroid history covering all major symptom domains including cardiovascular, metabolic, neuropsychiatric, gastrointestinal, and reproductive systems
- Perform a systematic clinical examination for thyroid disease including peripheral signs of thyrotoxicosis and hypothyroidism, correct bimanual thyroid palpation, and auscultation for bruit
- Demonstrate the correct posterior bimanual technique for thyroid palpation, assessing size, consistency, surface, nodularity, and mobility
- Generate a prioritised differential diagnosis for a patient with suspected thyroid disease based on history and clinical examination findings, distinguishing Graves disease from toxic nodular goitre, thyroiditis, and other causes
INSTRUCTIONS
This skills-based module covers the clinical evaluation of thyroid disease — history-taking, examination technique, sign interpretation, and differential diagnosis. It maps to NMC competencies IM12.4, IM12.5, IM12.6, and IM12.7 at the SH and KH levels. You are expected to be able to perform these skills in a supervised clinical encounter.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Clinical Approach to Thyroid Disease (textbook)
- API Textbook of Medicine, 10th ed. — Thyroid Examination and Clinical Skills (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed. — Examination of the Thyroid (textbook)
- American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism, 2016 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Meena, a final-year resident, calls you to the outpatient room. A 29-year-old woman has come in with a complaint she describes only as 'feeling restless and hot'. She is thin, fidgety, and her eyes appear to protrude slightly. Before any investigations are ordered, Dr Meena asks you to take a focused history and examine the patient. This is where clinical thyroidology begins — not with a blood test, but with a systematic conversation and a disciplined examination. By the time you finish examining this patient — her pulse rate, her hands, her neck, her reflexes — you should already have a working diagnosis in mind. The history and clinical examination in thyroid disease are not merely preludes to the blood test; they are rich diagnostic tools that establish severity, localise the most likely aetiology, and guide the prioritisation of investigations. This module will train you to take an IM12.4-to-IM12.7 level history and examination, to correctly palpate the thyroid, and to generate a differential diagnosis before the lab results arrive.
WHY THIS MATTERS
The clinical skills covered here are among the most commonly assessed in final-year MBBS OSCEs and vivas: thyroid history-taking, thyroid examination including correct palpation technique, identification of systemic features of thyrotoxicosis and hypothyroidism, and clinical reasoning from symptom cluster to a prioritised differential diagnosis. In daily clinical practice, a well-taken thyroid history predicts the diagnosis before investigations in the majority of cases. Incorrect palpation technique fails to detect goitre or characterise nodules reliably, delaying diagnosis of thyroid malignancy. The NMC competency set for this module — IM12.4 (history), IM12.5 (systemic examination), IM12.6 (thyroid palpation), IM12.7 (differential diagnosis generation) — all require you to demonstrate these skills at the SH or KH level in a supervised clinical setting.
RECALL
Before proceeding, recall the anatomy of the thyroid gland. The thyroid is a bilobed, butterfly-shaped endocrine gland in the anterior neck, straddling the trachea at the level of the 2nd to 4th tracheal rings, just below the larynx. The isthmus connects the two lobes across the trachea. A pyramidal lobe is present in approximately 50% of individuals, ascending from the isthmus toward the hyoid bone — a vestige of the thyroglossal duct. The gland moves upward on swallowing, a feature that distinguishes a thyroid mass from other anterior neck masses (a thyroglossal cyst moves on swallowing AND tongue protrusion; a lymph node does not move on swallowing). The two main clinical patterns of thyroid dysfunction you are examining for are: thyrotoxicosis (excess T3/T4 — a hyperadrenergic, hypermetabolic state) and hypothyroidism (deficient T3/T4 — a hypometabolic state). Recall that the autonomic nervous system modulates many of the clinical features you will elicit — increased sympathetic tone in thyrotoxicosis, and blunted sympathetic responsiveness in hypothyroidism.
Clinical Indication and Approach to Thyroid History
Thyroid disease presents with a remarkably diverse range of symptoms — from palpitations and weight loss in thyrotoxicosis to fatigue, constipation, and cognitive slowing in hypothyroidism. The structured thyroid history aims to accomplish four goals simultaneously: characterise the presenting complaint, identify the most likely diagnosis from the symptom pattern, assess severity and duration of disease, and flag any features that raise concern for malignancy or emergency (thyroid storm, myxoedema coma).
Provided image
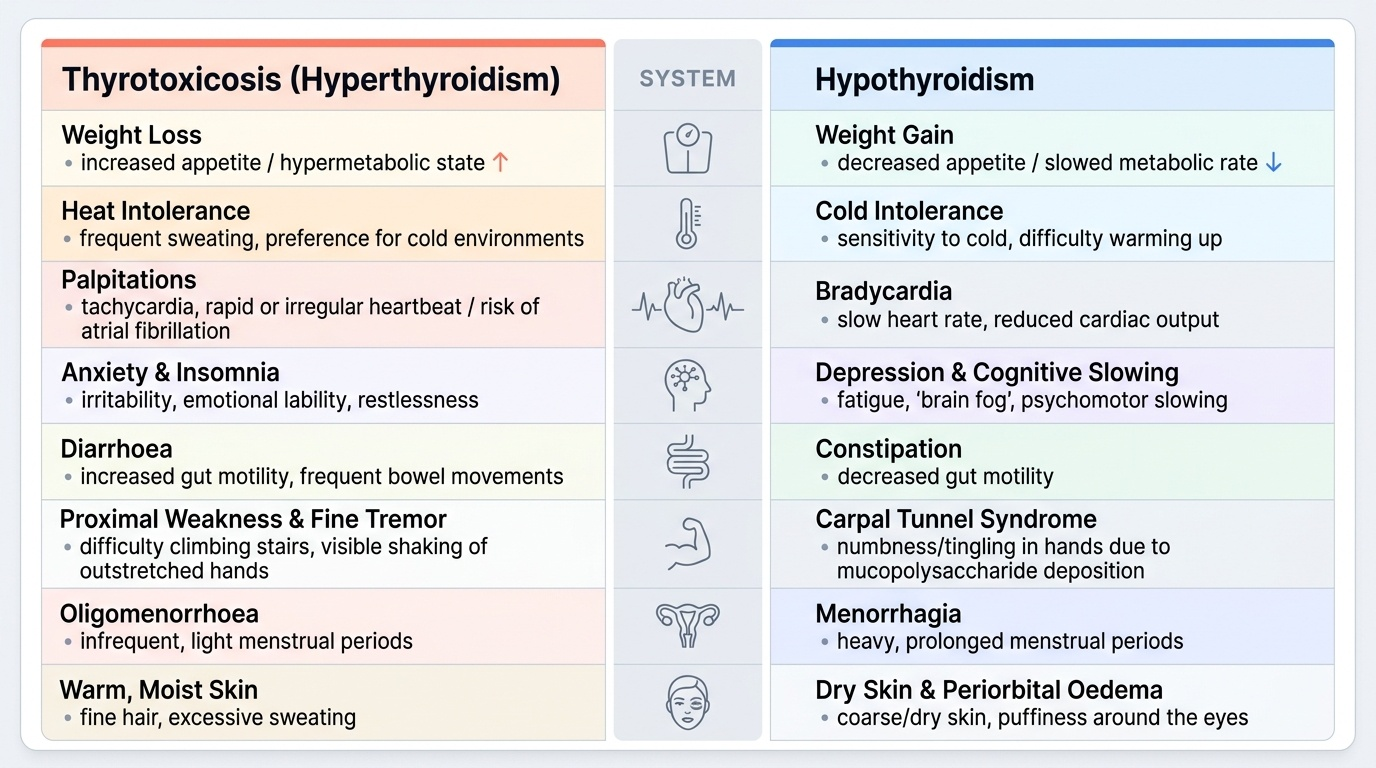
The history should be taken with a mental model of both thyroid states in mind. Rather than waiting for the patient to volunteer specific symptoms, a skilled clinician actively probes each organ system likely to be affected by thyroid hormone excess or deficiency. Begin with the presenting complaint and allow the patient to describe it in her own words — but then direct the inquiry systematically. The framework below covers the major symptom domains, with their thyrotoxic and hypothyroid polarities:
Weight and metabolic: Weight change is often the first clue. Weight loss with increased appetite is a cardinal feature of thyrotoxicosis (metabolic rate outstrips caloric intake); weight gain with decreased appetite or unchanged intake is typical of hypothyroidism. In elderly patients, thyrotoxicosis may present with weight loss alone — the 'apathetic hyperthyroidism' phenotype — without the adrenergic features.
Cardiovascular: Ask specifically about palpitations (rapid, sometimes irregular heartbeat — in thyrotoxicosis), dyspnoea on exertion, and ankle swelling (high-output cardiac failure in severe thyrotoxicosis or pericardial effusion in myxoedema). Duration, frequency, and whether palpitations are regular or irregular (may indicate atrial fibrillation) are important characterising details.
Neuropsychiatric: Thyrotoxicosis causes anxiety, irritability, emotional lability, insomnia, and fine tremor. Hypothyroidism causes fatigue, cognitive slowing ('brain fog'), depression, and in severe cases, dementia-like features. Ask: 'Have you noticed any change in your mood, concentration, or sleep recently?' Directly enquire about tremor (hands) in thyrotoxicosis.
Gastrointestinal: Thyrotoxicosis increases gut motility — patients report frequent bowel movements or diarrhoea. Hypothyroidism decreases gut motility — constipation, sometimes severe, is common. Nausea and vomiting can occur in thyroid storm.
Musculoskeletal: Thyrotoxicosis causes proximal muscle weakness (difficulty climbing stairs, rising from a chair) — thyrotoxic myopathy — without sensory symptoms. Hypothyroidism causes myalgia, cramps, and occasionally carpal tunnel syndrome (from mucopolysaccharide deposition compressing the median nerve).
Thermoregulation: Thyrotoxic patients feel heat intolerant and prefer cool environments; hypothyroid patients feel cold intolerant and require extra clothing. Heat intolerance with sweating, especially at night, is a sensitive symptom of thyrotoxicosis.
Menstrual: In women, thyrotoxicosis is classically associated with oligomenorrhea or amenorrhoea (reduced gonadotrophin release); hypothyroidism with menorrhagia (anovulatory cycles with unopposed oestrogen). Both affect fertility. Always ask about cycle regularity and any change since the symptom onset.
Neck symptoms: Ask about any visible or palpable swelling of the neck, its duration, rate of growth, any hoarseness of voice (recurrent laryngeal nerve involvement — suggests malignancy or large goitre), dysphagia (retrosternal extension), or pain (subacute thyroiditis characteristically produces an exquisitely painful tender thyroid after a viral illness).
Red flags for malignancy: Hard, fixed, rapidly growing nodule; hoarseness; cervical lymphadenopathy; family history of medullary thyroid carcinoma or MEN2 syndrome; prior neck irradiation in childhood.
Drug and dietary history: Amiodarone (contains 37% iodine by weight) causes both hypo- and hyperthyroidism. Lithium causes hypothyroidism. Immune checkpoint inhibitors (pembrolizumab, nivolumab) cause thyroiditis. Iodine-rich seaweed supplements. Calcium supplements (reduce levothyroxine absorption if taken together).
Past medical and family history: Personal or family history of autoimmune diseases (type 1 diabetes, rheumatoid arthritis, pernicious anaemia, Addison disease, vitiligo) significantly raises the prior probability of autoimmune thyroid disease. Previous thyroid surgery or radioiodine therapy.
Governing Principles of Thyroid Examination
The thyroid examination is a clinical skill with specific technique requirements that distinguish a trained clinician from a novice. The governing principles derive directly from the anatomy and physiology of the gland: its position in the anterior neck below the cricoid, its attachment to the pretracheal fascia (causing it to rise on swallowing), its vascularity (a goitre in Graves disease has increased blood flow, producing a thrill and audible bruit), and its relationship to surrounding structures (trachea, recurrent laryngeal nerves, cervical lymphatics). A systematic, structured approach to the examination ensures you elicit all clinically relevant signs without missing either life-threatening emergencies (thyroid storm, impending airway compromise) or high-yield diagnostic clues (the eye signs of Graves disease, the Addisonian pigmentation of polyglandular syndrome).
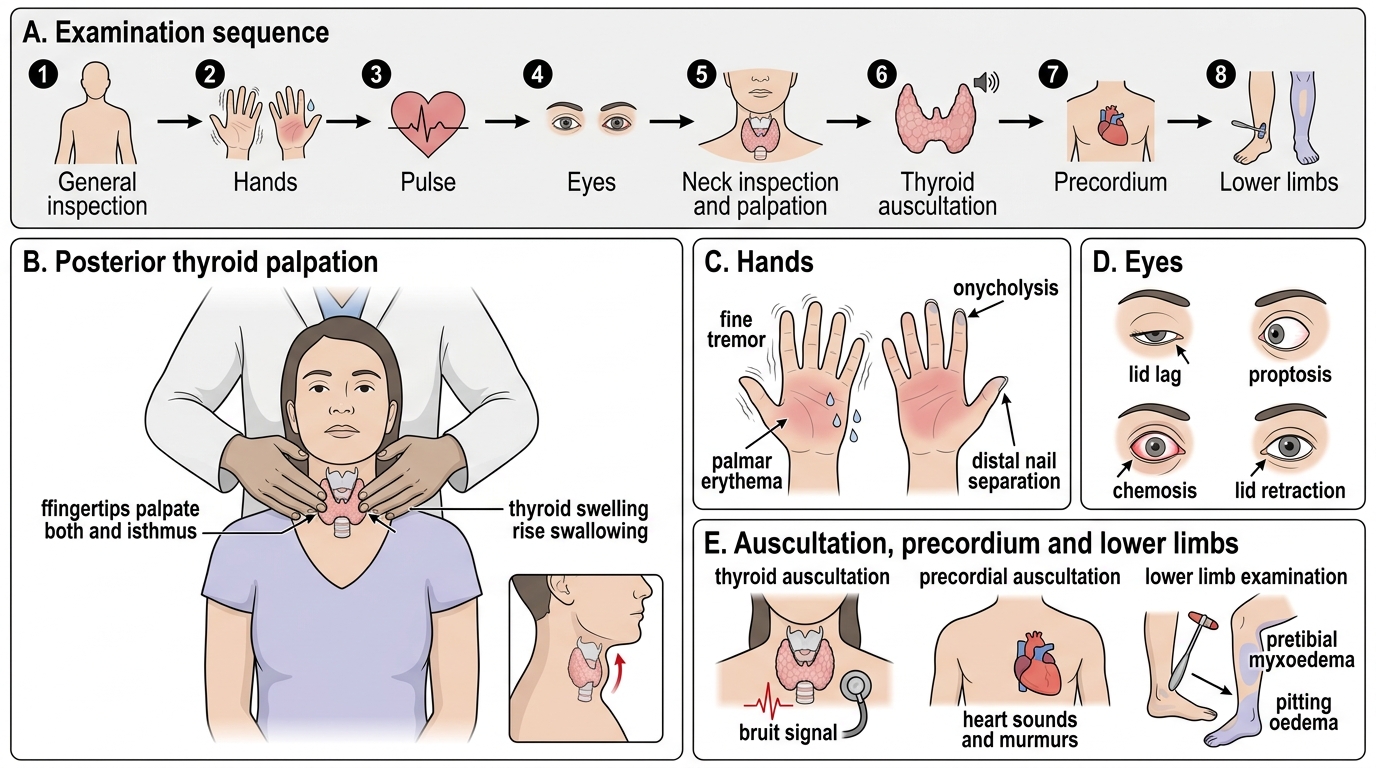
The principles underpinning the examination sequence are as follows: begin with the general inspection, which provides the most information per unit of time; assess the hands for the peripheral signs of thyroid dysfunction before approaching the neck; examine the neck with the patient seated, using the swallowing manoeuvre to confirm gland origin; palpate the thyroid systematically using the correct posterior approach; auscultate the gland only after palpation; assess the eyes formally in every patient with thyroid disease, not only when ophthalmopathy is suspected; and complete the cardiovascular and neurological assessments, which provide objective severity markers. The examination findings, interpreted alongside the history, should allow you to generate a prioritised differential diagnosis before any biochemical result is available.
IMPORTANT: the sequence of the examination is itself a clinical skill. A common student error is to proceed directly to the neck when the patient presents with 'neck swelling', neglecting the peripheral signs that may be more discriminating. The fine tremor of the outstretched hands, the warm moist palms, the tachycardia, and the hyperreflexia together constitute a more reliable sign cluster for thyrotoxicosis than neck palpation alone. Similarly, the dry skin, periorbital puffiness, bradycardia, and slow-relaxing reflexes of hypothyroidism are often more striking than the neck examination.
Clinical Examination Sequence in Thyroid Dysfunction
Thyroid Palpation Technique and Examination Findings
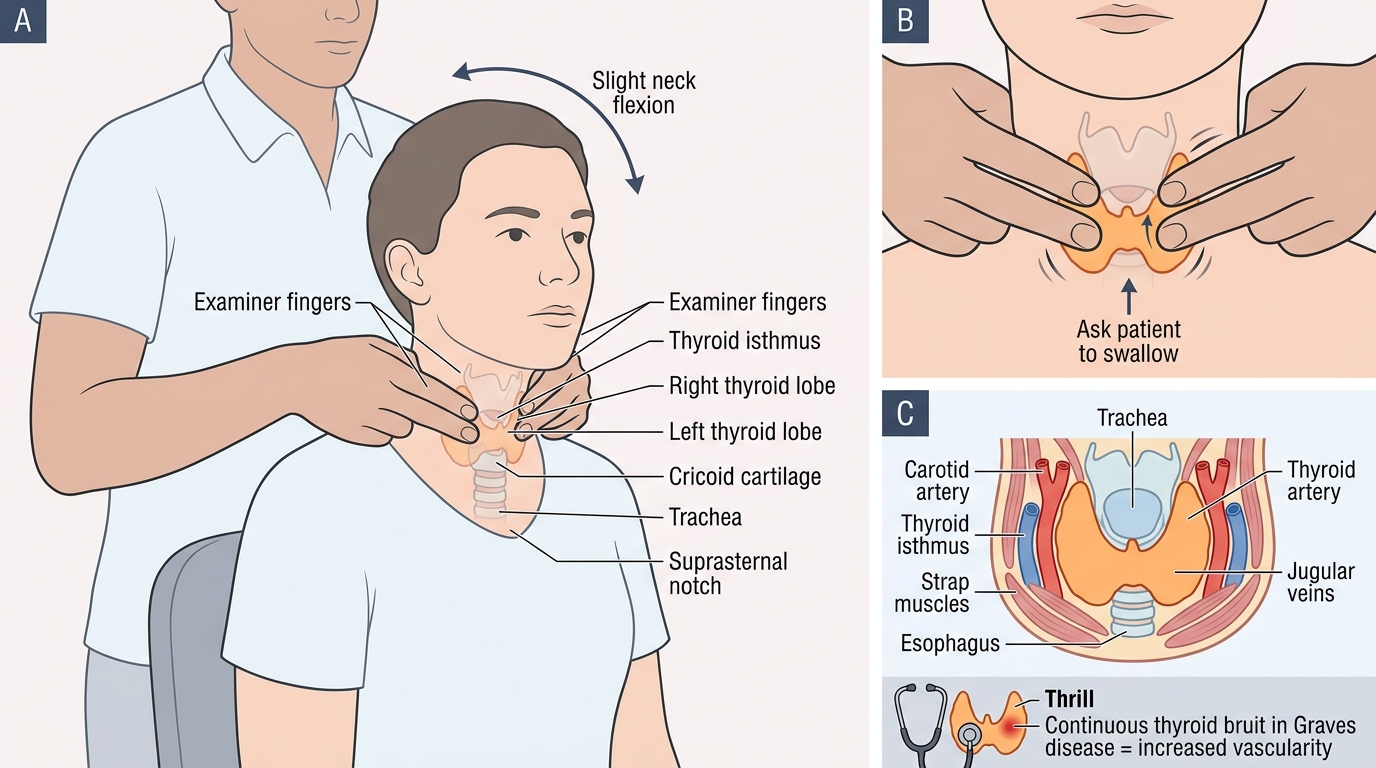
The correct technique for thyroid palpation is the posterior approach, which allows simultaneous two-handed palpation of both lobes and the isthmus, provides better stabilisation of the gland, and allows the examiner to assess consistency and nodularity more reliably than the anterior approach. This technique should be mastered as a reproducible clinical skill.
Step 1 — Positioning: The patient sits upright, facing forward, with the neck slightly extended to expose the thyroid. The examiner stands behind the patient.
Step 2 — Inspection (neck): Before palpating, inspect the anterior neck in good lighting. Ask the patient to swallow a sip of water; watch the neck. A thyroid swelling rises with swallowing. Compare the two sides for symmetry. A visible swelling is defined as a goitre (from Latin gutturia, throat). Note whether the swelling is diffuse (uniform bilateral enlargement) or nodular (visible irregularity, particularly over one lobe).
Step 3 — Posterior bimanual palpation: Stand behind the patient. Place both hands around the patient's neck with the fingertips of both hands meeting at the midline over the isthmus. Use the pads (not tips) of the index and middle fingers of both hands. Gently flex the patient's neck slightly forward to relax the strap muscles and sternocleidomastoids. Begin palpation at the isthmus, then systematically move to the right lobe (patient turns head slightly to the right and examiner uses right hand to push the trachea toward the right while left hand palpates the left lobe that has been pushed forward — the 'tennis ball technique'), then to the left lobe. Ask the patient to swallow — feel the gland move under your fingers.
Step 4 — What to assess on palpation:
- Size: Normal thyroid weight is ~20 g; a clinically detectable goitre weighs at least 25–30 g. Grade goitre using the WHO classification: Grade 0 = not palpable; Grade 1 = palpable but not visible; Grade 2 = palpable and visible.
- Consistency: A soft goitre suggests normal tissue or colloid; a firm, rubbery goitre is characteristic of Hashimoto thyroiditis; a hard or stony-hard gland raises concern for malignancy or Riedel thyroiditis; a tender goitre indicates subacute (de Quervain) thyroiditis.
- Surface: Smooth (Graves disease) vs nodular (multinodular goitre, adenoma, malignancy).
- Mobility: A mobile goitre moves with swallowing and is not fixed to surrounding structures. Fixity — inability to move with swallowing or fixation to adjacent tissues — is a red flag for malignancy or invasive Riedel thyroiditis.
- Nodule assessment: If a nodule is found, characterise: size (cm), location (which lobe, pole), consistency (soft/firm/hard), tenderness, mobility. A solitary 'cold' nodule on scintigraphy (non-functioning) has a ~5–10% malignancy risk; a hot nodule (autonomous) has negligible malignancy risk.
- Cervical lymph nodes: Palpate the anterior and posterior cervical chains and the submandibular and submental groups. Palpable hard cervical nodes in the context of a thyroid nodule suggest lymph node metastasis and warrant urgent referral.
Step 5 — Auscultation: Place the bell of the stethoscope over the thyroid after palpation. A thyroid bruit (a low-pitched, continuous murmur) is a sign of markedly increased vascularity and is pathognomonic of Graves disease (not found in toxic multinodular goitre or thyroiditis). Distinguish from a carotid bruit (which is heard best lateral to the thyroid and obliterates on pressure) and from a transmitted heart murmur.
Peripheral signs of thyroid dysfunction:
- Hands: Warm, moist, tremulous hands with fine resting tremor (extend arms forward, place paper on dorsum — paper shakes) = thyrotoxicosis. Dry, cold, puffy hands with coarse skin = hypothyroidism. Onycholysis (separation of nail from nail bed at the distal edge — Plummer nails) = thyrotoxicosis, especially Graves disease.
- Cardiovascular: Tachycardia (>100 bpm at rest) = thyrotoxicosis. Bradycardia (<60 bpm) = hypothyroidism. Atrial fibrillation — irregularly irregular pulse = complication of thyrotoxicosis, especially in older patients. Pericardial rub/muffled heart sounds/JVP elevation = pericardial effusion in myxoedema.
- Eyes: Lid retraction (scleral show above the iris) and lid lag (upper lid lags behind the globe on downward gaze — von Graefe sign) occur with any cause of thyrotoxicosis due to sympathetic overactivation of the superior tarsal muscle. Exophthalmos (proptosis) — protrusion of the eyeball beyond the orbital rim — is specific to Graves disease (not other causes of thyrotoxicosis) due to orbital fibroblast activation by TRAb.
- Neurological: Hyperreflexia with brisk, fast-relaxing tendon jerks = thyrotoxicosis. Slow-relaxing reflexes ('hung-up' reflexes) — delayed relaxation phase of the ankle jerk = hypothyroidism. Test by percussing the ankle tendon with knee flexed; in hypothyroidism, the foot plantar-flexes slowly and relaxes slowly.
- Skin and hair: Fine, silky hair with rapid growth = thyrotoxicosis. Dry, coarse, brittle hair; outer third of the eyebrows lost (Hertoghe sign) = hypothyroidism. Pretibial myxoedema (orange-peel, non-pitting, bilateral plaques on the anterior shin) = Graves disease specifically.
Posterior Bimanual Thyroid Palpation
SELF-CHECK
During thyroid examination of a 34-year-old woman, you find a diffuse goitre with a palpable thrill and an audible low-pitched continuous bruit over the thyroid gland. Which of the following best explains the bruit?
A. Transmitted murmur from aortic stenosis
B. Markedly increased thyroid vascularity due to TSH receptor antibody-driven hyperstimulation of the gland in Graves disease
C. Turbulent flow in the carotid artery adjacent to an enlarged lymph node
D. Venous hum from the jugular vein overlying the thyroid
Reveal Answer
Answer: B. Markedly increased thyroid vascularity due to TSH receptor antibody-driven hyperstimulation of the gland in Graves disease
A thyroid bruit — a continuous low-pitched murmur best heard over the thyroid lobes — reflects markedly increased intrathyroidal blood flow. In Graves disease, TSH receptor antibodies (TRAb/TSI) drive continuous follicular cell hyperactivity, increasing the gland's metabolic demands and causing vascular hypertrophy. A thrill may be palpable as well. This sign is pathognomonic of Graves disease among the causes of hyperthyroidism; it is not found in toxic multinodular goitre or thyroiditis. A carotid bruit is lateral to the thyroid, systolic only, and obliterates on pressure. A transmitted murmur from the heart is usually systolic and diminishes with distance from the precordium. A venous hum is heard in the supraclavicular region and is obliterated by gentle jugular compression.