Page 2 of 17
IM12.{1-3,11} | Thyroid Dysfunction Foundations — SDL Guide (Part 2)
Radioiodine Uptake: Principles and Diagnostic Role
The radioactive iodine uptake (RAIU) test exploits a fundamental property of the thyroid gland: its unique ability to concentrate iodine for hormone synthesis. Because the thyroid is the only tissue in the body that actively transports and organifies iodine, radioactive iodine isotopes administered orally are selectively concentrated in thyroid follicular cells, allowing both functional assessment and anatomical imaging of thyroid activity. Understanding this test requires integrating thyroid physiology with basic nuclear medicine principles.
Provided image
The isotopes used: The two isotopes of iodine used in clinical thyroidology are ¹²³I and ¹³¹I. ¹²³I emits gamma rays only, with a short half-life of 13 hours — properties that make it ideal for diagnostic RAIU testing and imaging, as the radiation dose to the patient is low. ¹³¹I emits both gamma rays (useful for imaging) and beta particles (which cause localised tissue destruction) — these beta-particle properties make it the agent of choice for radioiodine therapy of hyperthyroidism and thyroid cancer. ¹³¹I has a half-life of 8 days.
Principle of RAIU measurement: After oral administration of the radioiodine capsule or solution, the tracer is absorbed from the gut and enters the iodine pool. The sodium-iodide symporter (NIS) on thyroid follicular cells actively transports both radioactive and stable iodine from the bloodstream. The percentage of administered radioactivity taken up by the thyroid is measured with a gamma camera at defined time points — typically 4–6 hours and 24 hours after administration. Normal RAIU at 24 hours is approximately 10–35% (varies by region and dietary iodine intake; Indian values may differ from Western references due to variable background iodine supply). A high uptake means the gland is metabolically active and avidly concentrating iodine — as occurs in Graves disease and toxic nodular goitre. A low uptake means the gland is suppressed, unable to trap iodine, or the thyrotoxicosis is not driven by endogenous synthesis — as occurs in thyroiditis (where hormone leaks from damaged follicles but synthesis is not active) and factitious thyrotoxicosis (ingestion of exogenous T4/T3, which suppresses endogenous production).
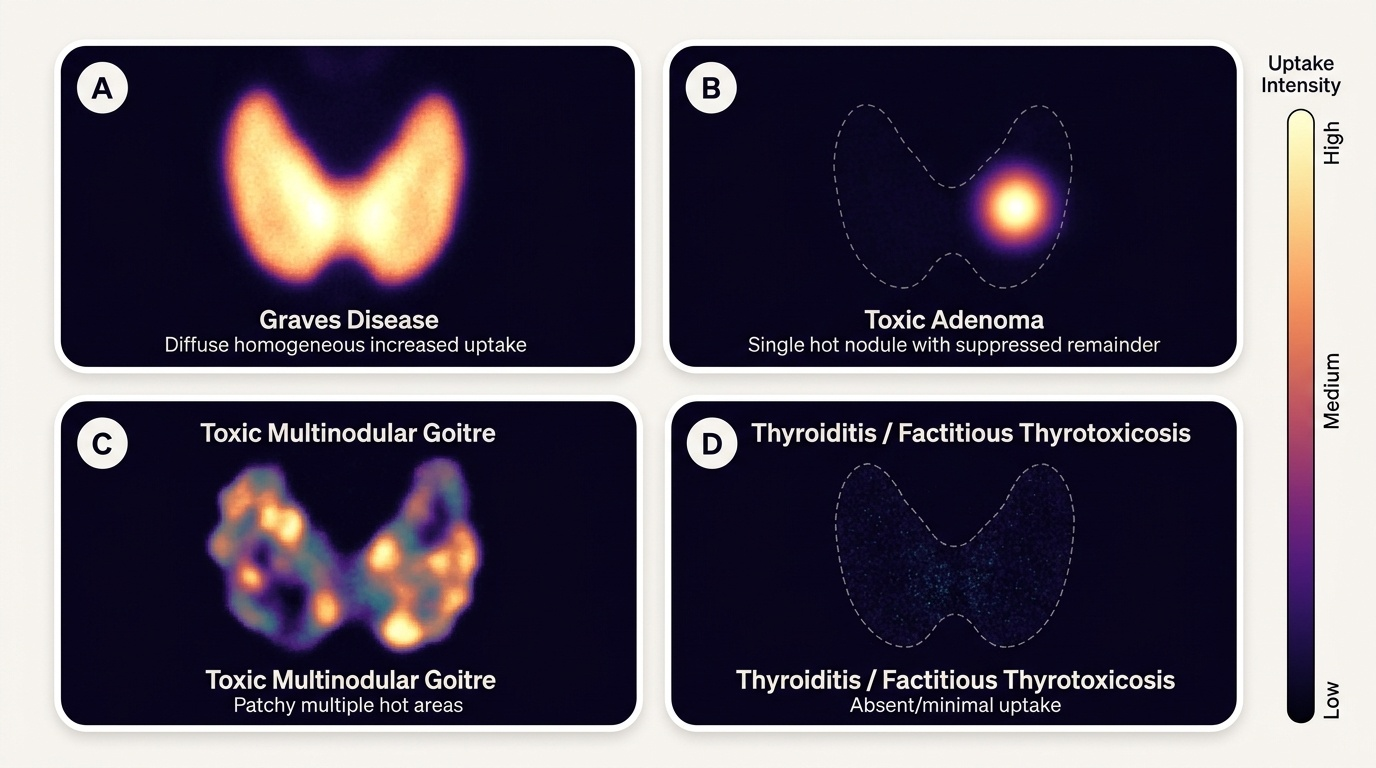
Diagnostic application — pattern interpretation:
- High RAIU, diffuse uptake: Graves disease — the entire gland is stimulated by TRAb
- High RAIU, focal hot nodule with suppressed rest of gland: toxic adenoma (Plummer disease) — autonomous nodule producing T3/T4 independent of TSH, suppressing the remainder
- High RAIU, multiple focal areas: toxic multinodular goitre (TMNG)
- Low RAIU + thyrotoxicosis: subacute (de Quervain) thyroiditis (inflammatory, iodine leakage), postpartum thyroiditis, silent thyroiditis, or factitious thyrotoxicosis
- Low RAIU + hypothyroidism: not the primary diagnostic use of RAIU for hypothyroidism; TSH + FT4 is preferred
This pattern recognition has direct therapeutic implications: low-RAIU thyrotoxicosis cannot be treated with radioiodine (there is nothing to target), and antithyroid drugs have limited utility (synthesis is not occurring). These patients are treated conservatively with beta-blockers and NSAIDs (for thyroiditis) and observed.
Contraindications: RAIU is contraindicated in pregnancy (radiation risk to fetal thyroid, which begins concentrating iodine from week 10–12 of gestation). It is also deferred in breastfeeding (¹³¹I is secreted in breast milk). A pregnancy test is mandatory before RAIU in any woman of childbearing age.
Technetium pertechnetate scan: As an alternative first-line thyroid imaging tool in many Indian centres, ⁹⁹ᵐTc-pertechnetate scintigraphy shares the NIS transport property with iodine (it is trapped but not organified) and gives similar functional information about regional gland activity (hot vs cold nodules) at a lower radiation dose and without the iodine constraint.
India's Iodine Deficiency Control Programme (NIDDCP)
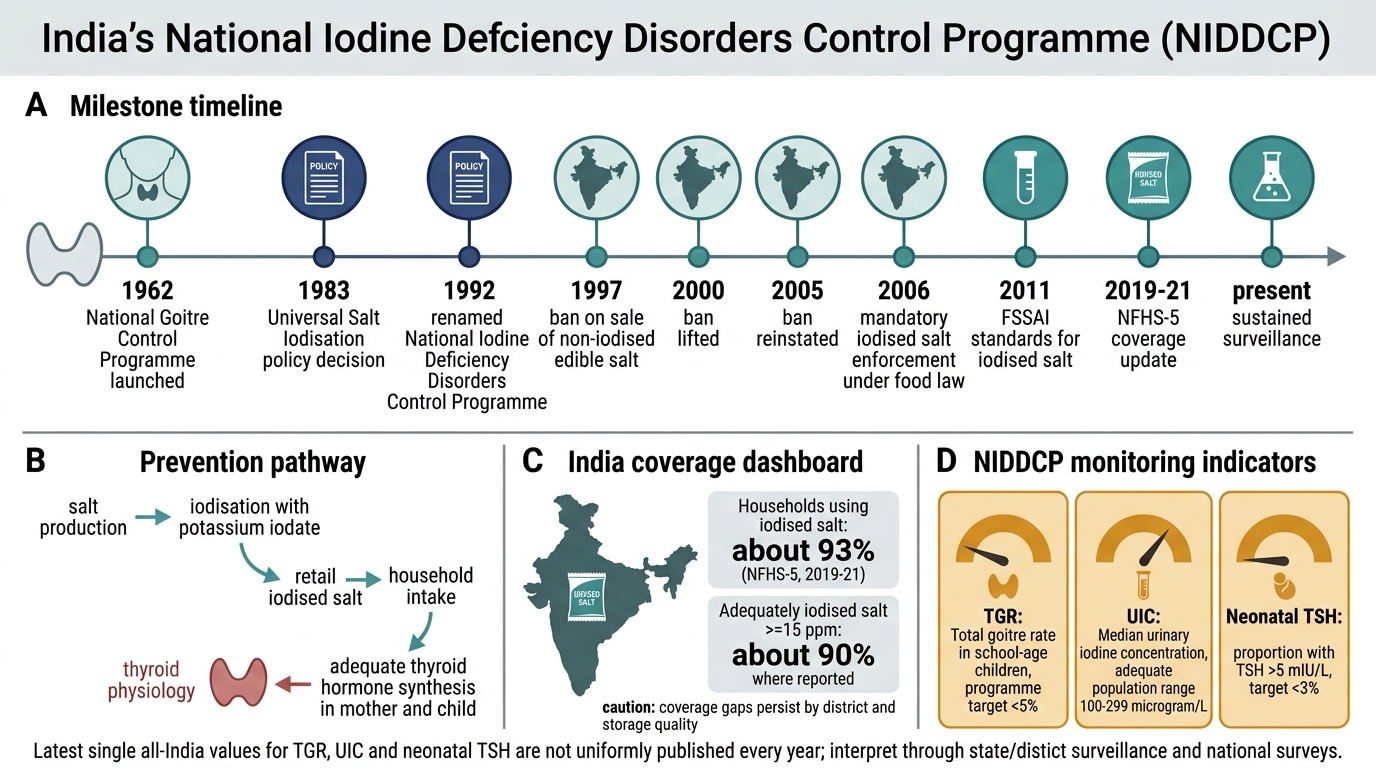
The National Iodine Deficiency Disorders Control Programme (NIDDCP) is one of India's most enduring and impactful public health initiatives, addressing the largest nutritional cause of preventable brain damage worldwide. Its history, structure, and achievements are directly relevant to clinical practice because they explain the epidemiology you will encounter — why goitre is endemic in certain regions, why cretinism has declined, and why iodine excess can occasionally cause paradoxical thyroid dysfunction.
Historical background: India first recognised the problem of endemic goitre in the sub-Himalayan belt and inland districts in the 1950s. The National Goitre Control Programme was launched in 1962 with the primary objective of supplying iodised salt to endemic goitre areas. Recognising that iodine deficiency causes a far broader spectrum of disorders than goitre alone — including subclinical hypothyroidism, impaired cognitive development, neonatal hypothyroidism, and stillbirths — the programme was renamed and expanded to the National Iodine Deficiency Disorders Control Programme (NIDDCP) in 1992. The key intervention is universal salt iodisation (USI): all edible salt for human and animal consumption is iodised to a level of 15 parts per million (ppm) at the retail level (the standard was 30 ppm at the production level to account for processing and storage losses, revised under Prevention of Food Adulteration rules). The Food Safety and Standards Authority of India (FSSAI) regulates salt iodisation standards.
Epidemiological targets and achievements: The programme's goal was to reduce IDD to a level where it is no longer a public health problem — defined as: goitre prevalence <5% in school-age children, median urinary iodine concentration (UIC) ≥100 µg/L, <50% of the population with UIC <100 µg/L, and <20% of households not using adequately iodised salt. Several states have achieved these targets; however, significant inter-state variation persists. The total goitre rate (TGR) has decreased substantially in most endemic zones since the programme's inception.
Clinical relevance of iodine status: As a clinician, awareness of NIDDCP informs your differential diagnosis. In a patient from a sub-Himalayan or inland district presenting with goitre and hypothyroidism, iodine deficiency remains in the differential even today, particularly in low-income, non-urban populations who may use non-iodised salt from local sources. Conversely, iodine supplementation in people with pre-existing subclinical Hashimoto thyroiditis can trigger overt hypothyroidism (Wolff-Chaikoff effect and loss of adaptation in susceptible individuals). Additionally, iodinated contrast agents (used in CT and cardiac catheterisation) can precipitate both hyperthyroidism (jod-Basedow phenomenon — iodine excess triggering autonomous nodule activation) and hypothyroidism — making thyroid status evaluation relevant before contrast procedures in at-risk patients.
Monitoring programme: NIDDCP monitoring uses three indicators: (1) total goitre rate (TGR) in school-age children (clinical measurement); (2) median urinary iodine concentration (UIC) as a population-level indicator of current iodine intake; (3) neonatal TSH screening (whole-blood TSH on filter paper) to detect congenital hypothyroidism, with a target of <3% of neonates with TSH >5 mIU/L. India introduced the universal newborn screening programme in some states, though coverage is not yet national.
NIDDCP Milestones and Monitoring
SELF-CHECK
A 28-year-old woman presents with symptomatic thyrotoxicosis: palpitations, weight loss, and tremor. Her serum TSH is undetectable and Free T4 is elevated. Radioactive iodine uptake (RAIU) at 24 hours is 3% (reference: 10–35%). Which of the following diagnoses is most consistent with this pattern?
A. Graves disease
B. Toxic multinodular goitre
C. Subacute (de Quervain) thyroiditis
D. Toxic adenoma
Reveal Answer
Answer: C. Subacute (de Quervain) thyroiditis
Low RAIU in the setting of thyrotoxicosis means the gland is not actively trapping iodine. This occurs when elevated circulating T4/T3 does not arise from active thyroid synthesis — as in thyroiditis, where inflammatory destruction releases preformed hormone into the circulation (passive hormone leak, not active synthesis). In Graves disease, toxic multinodular goitre, and toxic adenoma, the gland is actively synthesising excess hormone and RAIU is elevated (often >35–60%). Subacute (de Quervain) thyroiditis is the classic cause of thyrotoxicosis with low RAIU, typically preceded by a viral upper respiratory tract infection and associated with a painful, tender thyroid and elevated ESR.
Self-Assessment: Integrating HPT Axis Knowledge
This final section integrates the epidemiology, physiology, pathogenesis, and RAIU principles from this module through structured clinical application scenarios. The goal is to move from recall to application — the competency level expected at KH for IM12.1, IM12.2, IM12.3, and IM12.11 — by presenting you with real-world hormonal patterns and asking you to identify the aetiology, link it to the underlying mechanism you have just studied, and reason toward management. Each scenario is designed to require you to apply the HPT axis physiology, not simply list facts. You should be able to reason from a hormonal pattern to the level of disease (primary thyroid failure, pituitary suppression, autonomous synthesis, or inflammatory hormone leak), and from that level to the diagnosis and its management implications. Commit the TFT patterns in the reference table below to memory — they are tested in every clinical examination and are the backbone of thyroid function test interpretation taught formally in the diagnostics module. Work through each scenario before reading the analysis.
Review the following reference summary before working through the scenarios:
| Condition | TSH | FT4 | FT3 | RAIU | Key antibodies |
|---|---|---|---|---|---|
| Primary hypothyroidism (overt) | High | Low | Low | Low | Anti-TPO (Hashimoto) |
| Subclinical hypothyroidism | High | Normal | Normal | Normal | Anti-TPO (if Hashimoto) |
| Primary hyperthyroidism (overt) | Low/undetectable | High | High | High (Graves/toxic) / Low (thyroiditis) | TRAb (Graves), Anti-TPO (Graves/Hashimoto) |
| Subclinical hyperthyroidism | Low | Normal | Normal | Variable | Variable |
| Secondary hypothyroidism (pituitary) | Low | Low | Low | Low | None |
| Sick euthyroid syndrome | Low/normal | Low/normal | Low | N/A | None |
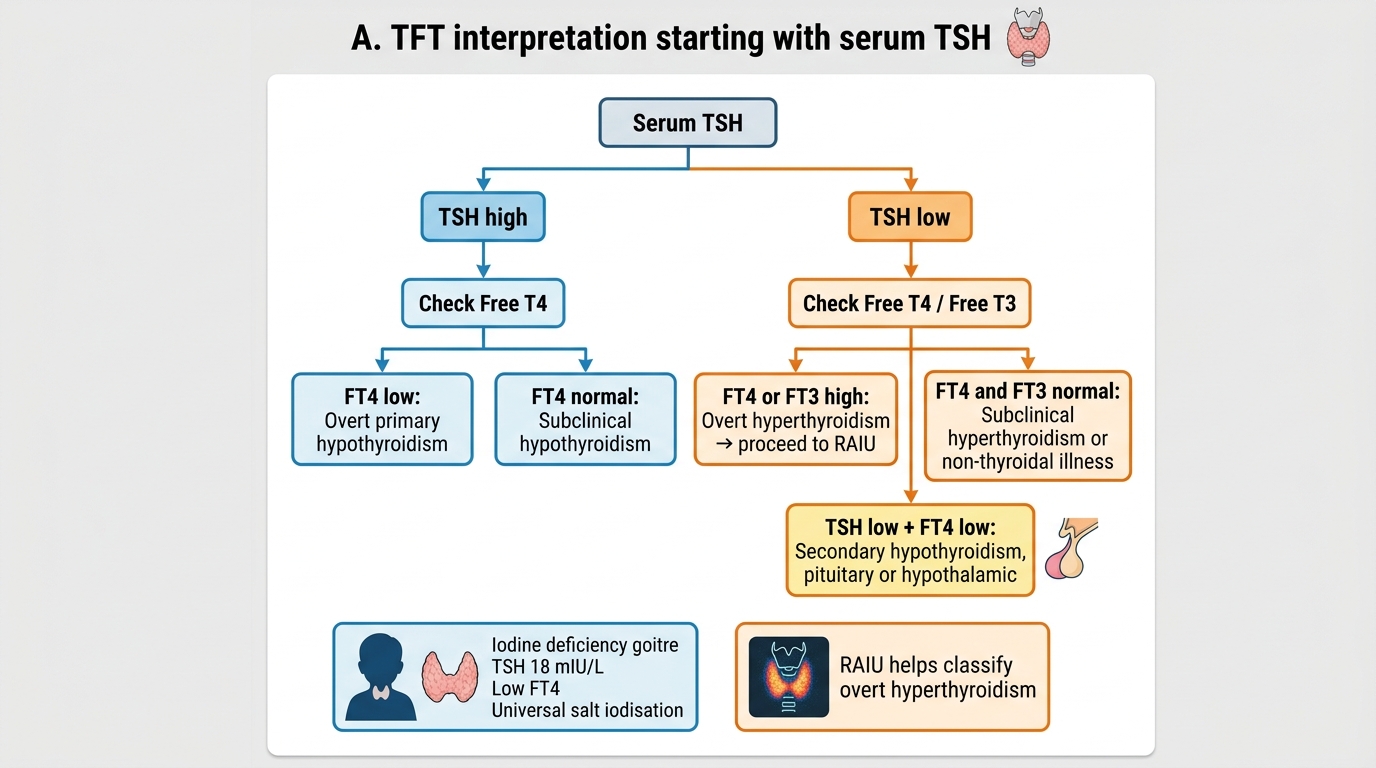
TFT Interpretation Algorithm Starting With Serum TSH
Scenario A: A 10-year-old girl from a remote sub-Himalayan district presents with a large painless neck swelling and short stature. Her schoolteacher reports that she was bright until a few years ago but now struggles academically. Serum TSH is 18 mIU/L; Free T4 is low. Urinary iodine concentration is 28 µg/L (deficient: <100 µg/L). Anti-TPO antibodies are negative. What is the most likely aetiology and what public health measure directly addresses this?
Analysis: Overt primary hypothyroidism in a child from an iodine-deficient area with negative autoimmune antibodies — the aetiology is iodine deficiency goitre and hypothyroidism. The cognitive decline suggests prolonged inadequate thyroid hormone, impairing brain development. The public health measure is universal salt iodisation (USI) under NIDDCP — ensuring that all edible salt provides ≥15 ppm iodine at retail level. Treatment requires levothyroxine and, if the family uses non-iodised salt, dietary iodine supplementation.
Scenario B: A 38-year-old woman is treated for hyperthyroidism with carbimazole for 18 months. Her hyperthyroidism has resolved, but now she complains of fatigue, constipation, and weight gain. Her TSH is undetectable, and FT4 is low. What is the likely explanation for the dissociation between undetectable TSH and low FT4?
Analysis: This is central hypothyroidism from pituitary TSH suppression — a well-recognised transient state following treatment of long-standing hyperthyroidism. Prolonged exposure to elevated T4/T3 downregulates pituitary thyrotroph cells; after hyperthyroidism is corrected, TSH recovery may lag behind FT4 normalisation for weeks to months. The TSH remains suppressed even as FT4 falls below normal. This is not pituitary disease; it is a reversible adaptation. Clinical symptoms of hypothyroidism with low FT4 confirm the patient needs levothyroxine supplementation, but TSH cannot be used as the monitoring target during this recovery phase — FT4 levels must guide dosing.
SELF-CHECK
A medical student is asked why Anti-TPO antibodies are present in both Hashimoto thyroiditis AND Graves disease, even though the two conditions produce opposite outcomes (hypothyroidism vs hyperthyroidism). Which of the following best explains this?
A. Anti-TPO antibodies directly stimulate the TSH receptor in Graves disease
B. Anti-TPO antibodies are pathognomonic of Graves disease only; their presence in Hashimoto is a laboratory error
C. Anti-TPO antibodies are markers of autoimmune activation of the thyroid and are present in both conditions, but the functional outcome is determined by whether the dominant antibody type is stimulatory (TRAb/TSI in Graves) or whether T-cell-mediated destruction predominates (Hashimoto)
D. Anti-TPO antibodies inhibit thyroid peroxidase, explaining hypothyroidism in both conditions
Reveal Answer
Answer: C. Anti-TPO antibodies are markers of autoimmune activation of the thyroid and are present in both conditions, but the functional outcome is determined by whether the dominant antibody type is stimulatory (TRAb/TSI in Graves) or whether T-cell-mediated destruction predominates (Hashimoto)
Anti-TPO antibodies reflect autoimmune sensitisation to a key thyroid enzyme and are found in both Hashimoto thyroiditis (>90%) and Graves disease (~75%). They are markers of autoimmune thyroid disease in general, not disease-specific. The functional outcome (hypo- vs hyperthyroidism) is determined by the balance of mechanisms: in Hashimoto thyroiditis, the dominant process is CD8+ T-cell cytotoxicity and ADCC leading to follicular destruction; in Graves disease, the dominant driver is stimulatory TRAb (TSI) that constitutively activates the TSH receptor. Anti-TPO antibodies are not the primary pathogenic drivers in Graves disease, and they do not stimulate the TSH receptor. Option D is incorrect — anti-TPO antibodies do not reliably inhibit TPO activity at physiological concentrations.
CLINICAL PEARL
The most commonly tested TFT pattern in examinations — and the most frequently misinterpreted in clinical practice — is the dissociation between TSH and FT4. Remember: TSH is a logarithmic responder to small changes in FT4. A doubling of FT4 can suppress TSH from 2 to 0.01 mIU/L — an apparently massive change. Conversely, a small fall in FT4 drives TSH markedly upward. This means TSH is the most sensitive screen for thyroid dysfunction — a normal TSH in a clinically stable patient virtually excludes primary thyroid disease. However, TSH is unreliable as a standalone test in three specific situations: (1) pituitary disease (where TSH may be inappropriately normal or low despite low FT4 — secondary hypothyroidism); (2) the first 6–12 weeks after treating hyperthyroidism (TSH recovery lag); and (3) sick euthyroid syndrome in acutely ill patients (suppressed TSH despite normal thyroid function, mediated by cytokines). In these three situations, always check FT4 and FT3 alongside TSH and interpret in context.