Page 10 of 17
IM12.12-14 | Thyroid Pharmacotherapy and Definitive Therapy — SDL Guide
Learning Objectives
- Describe the pharmacology, indications, adverse effects, and drug interactions of levothyroxine, carbimazole/methimazole, and propylthiouracil
- Write and communicate a levothyroxine prescription appropriate to the patient's age, sex, weight, comorbidities, and clinical status
- Describe the indications, contraindications, and practical considerations for thionamide therapy, radioiodine ablation, and thyroid surgery in the management of thyrotoxicosis
- Outline the pharmacological management of thyroid storm and myxoedema coma, including correct drug sequencing
INSTRUCTIONS
This module covers the pharmacology, dosing, and clinical decision-making for thyroid pharmacotherapy — levothyroxine (hypothyroidism), thionamides (hyperthyroidism), and definitive therapy (radioiodine, surgery). It maps to NMC competencies IM12.12, IM12.13, and IM12.14 at KH and SH levels.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Treatment of Thyroid Disorders (textbook)
- API Textbook of Medicine, 10th ed. — Thyroid Pharmacotherapy (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed. — Management of Thyroid Disease (textbook)
- American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism, 2016 (guideline)
- European Thyroid Association Guidelines for the Management of Graves Disease, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients come to you for treatment decisions. Patient 1 is a 26-year-old pregnant woman at 10 weeks gestation with newly diagnosed Graves hyperthyroidism — her TRAb is strongly positive, FT4 is elevated, and she has a small diffuse goitre. Patient 2 is a 58-year-old man with toxic multinodular goitre who has been euthyroid for 18 months on carbimazole and wants to know if he can stop the medication. Patient 3 is a 44-year-old woman with overt primary hypothyroidism (TSH 22 mIU/L, FT4 5.8 pmol/L) with no other medical conditions, weighing 68 kg. Each of these patients needs a precise pharmacological decision: which drug, what dose, which contraindications to check, what monitoring to arrange, and when to escalate to definitive therapy. This is the applied pharmacology competency set — IM12.12, IM12.13, and IM12.14 — the bridge between diagnosis and treatment that closes the clinical loop.
WHY THIS MATTERS
Thyroid pharmacotherapy errors cause real patient harm: under-dosed levothyroxine leaves hypothyroid patients symptomatic and at risk of myxoedema; over-dosed levothyroxine causes AF and osteoporosis; missing carbimazole-induced agranulocytosis is life-threatening; using carbimazole in the first trimester of pregnancy causes embryopathy; and failing to recognise the indications for definitive therapy — radioiodine or surgery — results in unnecessary long-term drug exposure. The NMC competencies IM12.12 (pharmacology of thyroxine and antithyroid drugs), IM12.13 (writing and communicating a levothyroxine prescription), and IM12.14 (indications for thionamide, radioiodine, and surgery in thyrotoxicosis) require you to integrate pharmacological knowledge with patient-specific decision-making at the KH and SH levels.
RECALL
Before proceeding, recall the key pathophysiological distinctions that determine treatment choice. In hypothyroidism, the thyroid is failing — treatment is straightforward hormone replacement with levothyroxine, titrated to TSH. In hyperthyroidism (thyrotoxicosis), the treatment depends on the aetiology: if due to autoimmune stimulation (Graves disease) or autonomous nodular activity (toxic adenoma, TMNG), the goal is to block hormone synthesis or ablate the gland — hence antithyroid drugs (thionamides), radioiodine, or surgery. If due to thyroiditis (passive hormone leak, not active synthesis), antithyroid drugs are NOT effective — beta-blockers and anti-inflammatories manage symptoms until the episode self-resolves. Also recall the two thionamides available in India: carbimazole (the prodrug, converted to methimazole in the body) and propylthiouracil (PTU) — they share a mechanism but have distinct clinical niches, particularly in pregnancy.
Hypothyroidism Pharmacotherapy: Levothyroxine
Levothyroxine (L-thyroxine, T4) is the standard pharmacological treatment for all forms of hypothyroidism — primary, secondary, and post-ablative. It is one of the most widely prescribed drugs worldwide, and prescribing it correctly requires understanding its pharmacokinetics, dosing principles, interactions, monitoring requirements, and patient-specific adjustments.
Mechanism and pharmacokinetics: Levothyroxine is a synthetic T4 identical to the naturally secreted hormone. After oral administration, it is absorbed primarily in the duodenum and jejunum — absorption is approximately 70–80% under fasting conditions and is significantly impaired by food, calcium supplements, iron preparations, antacids, cholestyramine, and proton pump inhibitors. These interactions have important practical implications: levothyroxine must be taken 30–60 minutes before food, in the morning on an empty stomach, separate from calcium and iron supplements by at least 4 hours. The half-life of T4 is approximately 7 days, which means steady-state is reached in about 4–6 weeks after any dose change — this is the basis for the monitoring interval.
Starting dose and titration:
- Healthy adults under 60 years: Start at the calculated full replacement dose: approximately 1.6 µg/kg/day of ideal body weight. For a 60 kg person, this would be approximately 96 µg/day, typically rounded to 100 µg/day. In clinical practice, 100 µg/day is a reasonable starting dose for most young to middle-aged adults with overt hypothyroidism and no cardiac disease.
- Elderly patients (>60 years) and those with cardiac disease (angina, arrhythmia, heart failure): Start low and titrate slowly — begin at 25–50 µg/day and increase by 25 µg every 4–6 weeks. The rationale is that sudden normalisation of thyroid hormone in a cardiovascular-compromised patient may precipitate angina, AF, or heart failure. Gradual titration allows the myocardium to adapt.
- Severe or long-standing hypothyroidism: Start low regardless of age — the body has adapted to low T4 levels, and abrupt normalisation may precipitate adrenal insufficiency (by accelerating cortisol clearance) or cardiac complications.
- Secondary hypothyroidism: Cortisol replacement (hydrocortisone 20 mg morning + 10 mg afternoon) MUST be initiated before or simultaneously with levothyroxine — T4 accelerates cortisol clearance, and starting T4 first can precipitate adrenal crisis. This is a non-negotiable sequence.
- Pregnancy: Levothyroxine requirements increase by approximately 30–50% during pregnancy because of increased TBG levels (more T4 binding), increased volume of distribution, placental T4 metabolism, and HCG-driven changes. The dose should be increased as soon as pregnancy is confirmed in a hypothyroid woman. The target TSH in pregnancy is: first trimester <2.5 mIU/L, second and third trimesters <3.0 mIU/L (may vary by guideline).
Monitoring: After initiating or changing the dose, check TSH after 4–6 weeks (time for steady-state). The treatment target is TSH within the normal reference range, typically 0.5–2.5 mIU/L for most patients (avoiding suppressed TSH, which causes bone loss and AF risk). In patients with differentiated thyroid cancer after total thyroidectomy, TSH is intentionally suppressed to <0.1 mIU/L (or 0.1–0.5 for low-risk disease) to reduce TSH-driven tumour stimulation — in this context, the bone and cardiac risks of suppressed TSH must be weighed against the oncological benefit. Once euthyroid, TSH should be rechecked every 6–12 months.
Adverse effects of levothyroxine: Adverse effects are dose-dependent and represent the effects of excess T4/T3 — tachycardia, palpitations, anxiety, tremor, heat intolerance, weight loss, diarrhoea, insomnia, and bone loss. Chronic TSH suppression (over-replacement) is the most clinically important long-term adverse effect — it causes cortical bone loss (particularly in postmenopausal women, increasing fracture risk) and atrial fibrillation (increased risk with suppressed TSH, especially in older patients). The lesson: never aim for suppressed TSH as a treatment target in primary hypothyroidism — the goal is normal TSH.
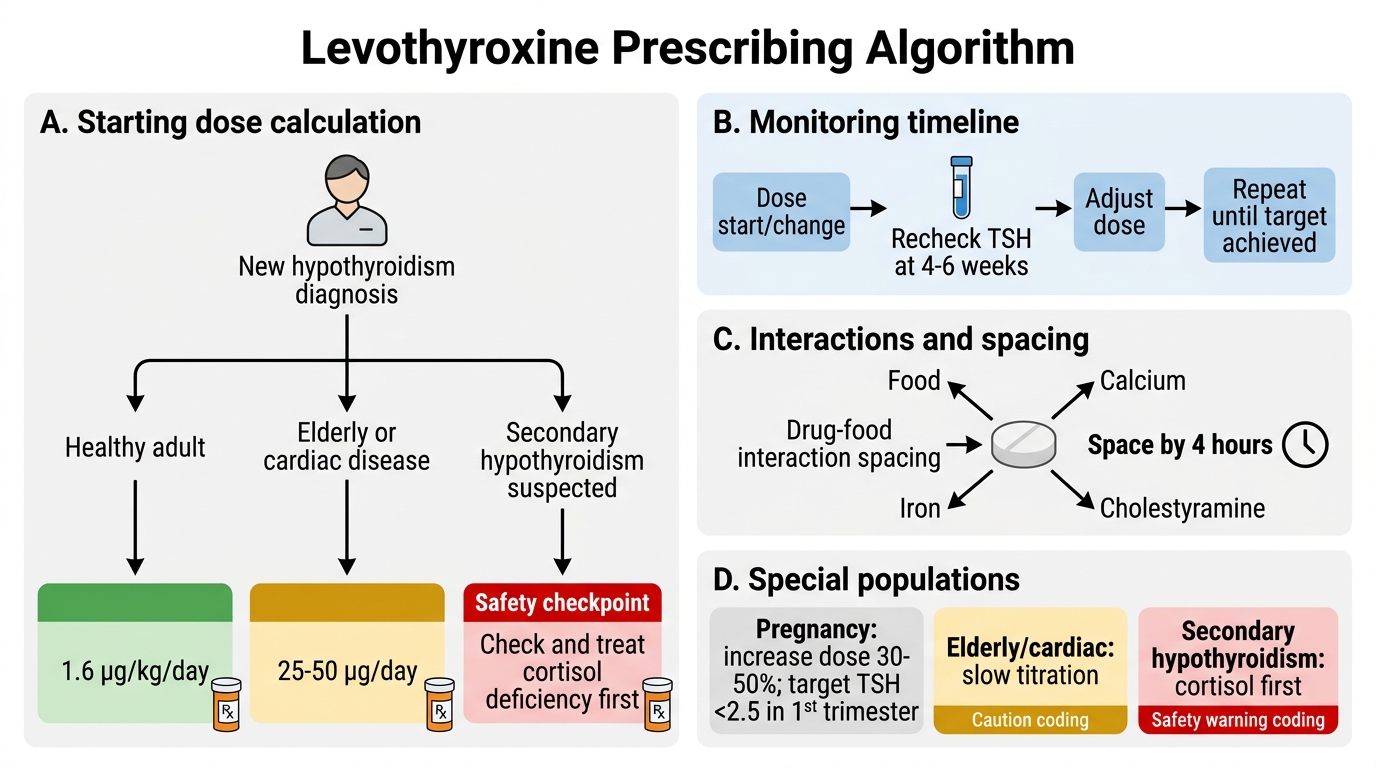
Levothyroxine Prescribing Algorithm
Antithyroid Drug Pharmacology: Thionamides
Thionamide drugs are the primary pharmacological treatment for hyperthyroidism arising from autonomous thyroid synthesis — specifically Graves disease and toxic nodular goitre. Their mechanism, pharmacokinetics, dosing, adverse effect profile, and specific contraindications (particularly in pregnancy) must be understood precisely, as errors in this area carry direct patient harm.
Provided image
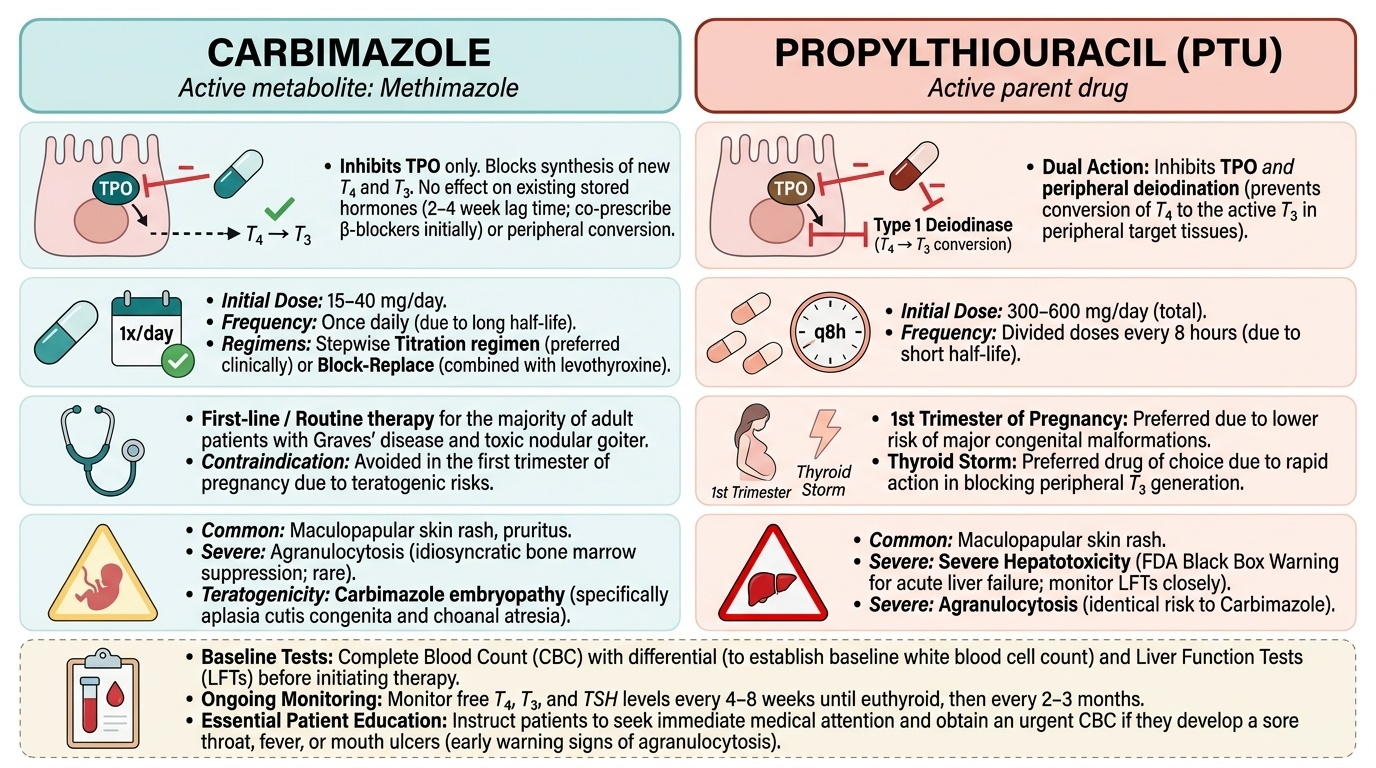
Mechanism of action: Both carbimazole (the prodrug) and propylthiouracil (PTU) inhibit thyroid peroxidase (TPO), the enzyme responsible for iodide oxidation and organification of thyroglobulin — the key steps in thyroid hormone synthesis. By blocking TPO, they prevent the production of new T4 and T3. They do NOT deplete existing stored hormone, nor do they affect hormone already in the circulation — therefore there is a lag period of 2–4 weeks before symptom improvement (the time needed to exhaust existing thyroid hormone stores). This is clinically important: patients remain symptomatic for the first few weeks of treatment, and beta-blockers (propranolol or atenolol) are co-prescribed to control adrenergic symptoms (palpitations, tremor, anxiety) during this period.
Additional mechanism of PTU: PTU, but not carbimazole/methimazole, also inhibits peripheral deiodination — the conversion of T4 to the active T3 in peripheral tissues. This additional action makes PTU preferable in thyroid storm (where urgent reduction of T3 levels is needed) and in the first trimester of pregnancy (where T3 levels are particularly important for fetal neural development). Carbimazole does NOT inhibit deiodination.
Dosing:
- Carbimazole: Initial dose for moderate-to-severe Graves hyperthyroidism: 20–40 mg/day (single daily dose or divided twice daily). For mild disease: 15–20 mg/day. Once euthyroidism is achieved (typically 4–8 weeks), the dose is either: (a) block-replace regimen — continue full blocking dose + add levothyroxine to prevent hypothyroidism (achieves stable thyroid hormone levels with fewer fluctuations but more adverse effects at higher carbimazole dose); or (b) titration regimen — reduce carbimazole dose stepwise as FT4 normalises (requires more frequent monitoring but lower total drug dose). In India, the titration regimen is most commonly used.
- Propylthiouracil (PTU): Initial dose: 100–200 mg every 8 hours (300–600 mg/day total). Three-times-daily dosing is required due to shorter half-life. PTU is preferred over carbimazole in the first trimester of pregnancy because carbimazole/methimazole is associated with specific congenital anomalies (carbimazole embryopathy): aplasia cutis (absence of scalp skin), choanal atresia, and other midline defects when given in the first trimester. PTU does not cause these defects. However, PTU carries a risk of rare but severe hepatotoxicity (hepatocellular damage, occasionally fulminant hepatic failure) — for this reason, carbimazole/methimazole is preferred at all other times. The recommended approach in Graves disease in pregnancy: PTU in the first trimester → switch to carbimazole in the second trimester (once the period of embryogenesis for carbimazole-sensitive structures has passed).
Duration of antithyroid drug therapy in Graves disease: Antithyroid drugs are not curative for Graves disease — they suppress thyroid hormone production but do not eliminate the underlying TRAb-driven autoimmunity. The typical course is 12–18 months of treatment, after which the drug is withdrawn and the patient is observed for relapse. Remission (persistent euthyroidism after drug withdrawal) occurs in approximately 30–50% of patients — those with small goitre, mild disease, and decreasing TRAb levels during treatment. Relapse (return of hyperthyroidism) occurs in 50–70% and is an indication for definitive therapy. Toxic multinodular goitre does NOT remit with antithyroid drugs — definitive therapy (radioiodine or surgery) is the eventual plan for all TMNG patients after achieving euthyroidism.
Adverse effects of thionamides:
- Common (5–10%): Rash (pruritic, maculopapular), arthralgia, urticaria, nausea, gastrointestinal upset. Minor rash: switch to the other drug (partial cross-reactivity). Severe rash (vasculitis, SLE-like): stop both drugs.
- Rare but serious: Agranulocytosis (0.1–0.5%) — absolute neutrophil count <0.5 × 10⁹/L; presents with fever, sore throat, mouth ulcers (typically within 3 months of starting); immediately stop drug, urgent CBC, admit, supportive care ± G-CSF. Hepatotoxicity (PTU-specific): Monitor LFTs; stop PTU if symptomatic hepatitis develops. Rare vasculitis (PTU > carbimazole): ANCA-positive vasculitis.
- First trimester embryopathy: Carbimazole/methimazole — aplasia cutis, choanal atresia. PTU — safer in first trimester.
SELF-CHECK
A 28-year-old woman is 8 weeks pregnant and is newly diagnosed with Graves hyperthyroidism (TRAb strongly positive, FT4 elevated). Which antithyroid drug and at what dose should be initiated?
A. Carbimazole 20 mg once daily — it is the preferred drug at all times
B. Propylthiouracil 100 mg every 8 hours — PTU is preferred in the first trimester to avoid carbimazole embryopathy
C. Radioiodine ablation — safest definitive therapy in pregnancy
D. Watchful waiting — antithyroid drugs should be avoided in the first trimester
Reveal Answer
Answer: B. Propylthiouracil 100 mg every 8 hours — PTU is preferred in the first trimester to avoid carbimazole embryopathy
In the first trimester of pregnancy, propylthiouracil (PTU) is the preferred antithyroid drug. Carbimazole/methimazole is associated with a specific embryopathy when given in the first trimester (aplasia cutis, choanal atresia, and other midline defects), so it is avoided during this period. PTU does not cause these defects. The recommended approach is: PTU in the first trimester, then switch to carbimazole in the second trimester (to reduce the risk of PTU hepatotoxicity with prolonged use). Radioiodine is absolutely contraindicated in pregnancy — it crosses the placenta, concentrates in the fetal thyroid from week 10–12, and ablates it. Watchful waiting is not appropriate — untreated maternal thyrotoxicosis causes fetal growth restriction, preterm birth, and thyroid storm.
Levothyroxine Prescription Communication
The NMC IM12.13 competency requires you not only to select the correct dose of levothyroxine but also to write a complete, legally valid prescription and communicate it effectively to the patient. This dual requirement — prescribing accuracy and patient communication — reflects the recognition that even the correct drug at the correct dose achieves suboptimal outcomes if the patient does not understand how to take it correctly.
Elements of a valid levothyroxine prescription:
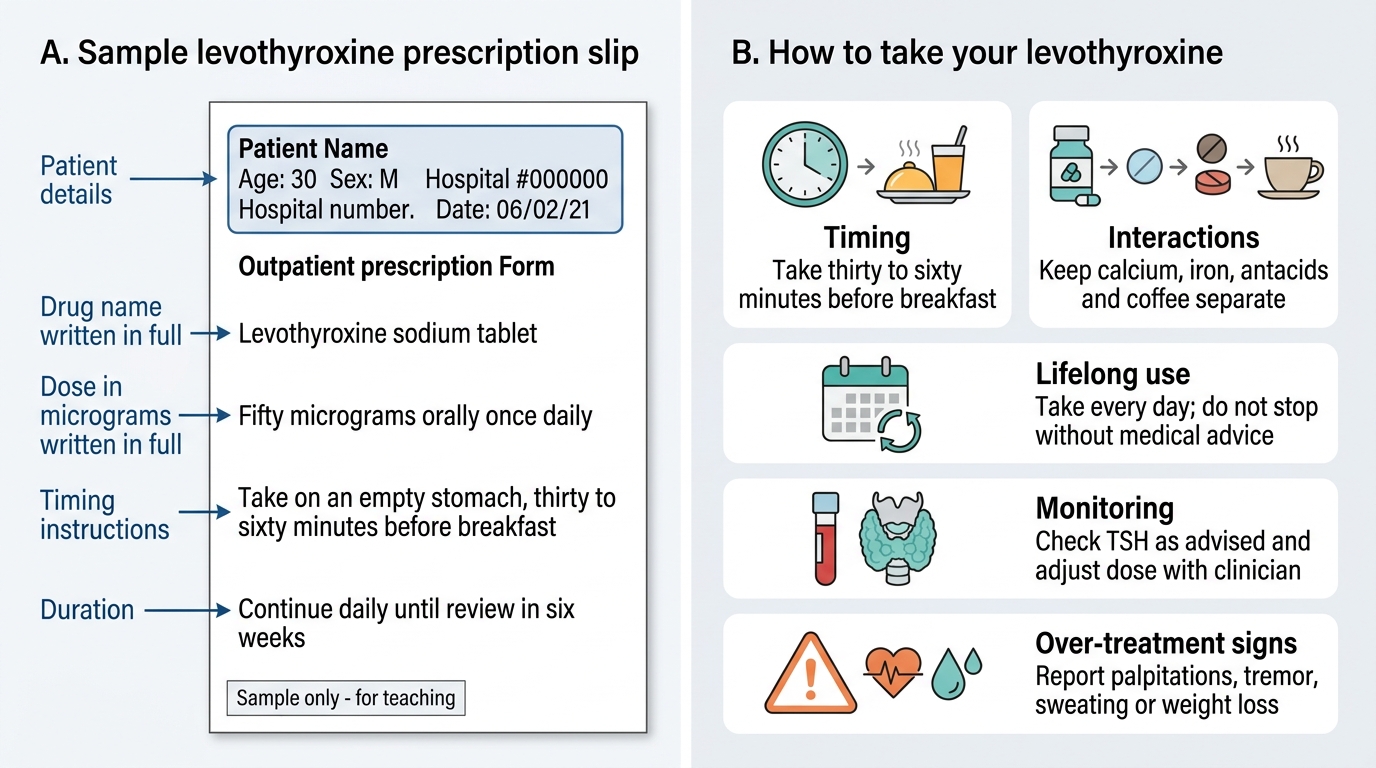
A complete prescription must include: patient's full name, age, and address; date of prescription; drug name (Levothyroxine sodium — generic name preferred); strength (e.g., 100 micrograms — always write 'micrograms' in full, never abbreviate as 'mcg' or 'µg' on handwritten prescriptions to prevent misreading as 'mg'); dose (e.g., 1 tablet daily); route (oral); frequency (once daily in the morning); duration or number of tablets; and the prescriber's name, registration number, and signature. In India, levothyroxine is a Schedule H drug (prescription only).
Sample prescription for a 68 kg, 38-year-old woman with newly diagnosed overt hypothyroidism:
Dose calculation: 1.6 µg/kg × 68 kg = 108.8 µg → round to 100 µg/day (nearest available tablet strength; 88 µg, 100 µg, 112 µg, 125 µg are common strengths). For this patient: Levothyroxine sodium 100 micrograms, one tablet by mouth, once daily in the morning on an empty stomach, 30–60 minutes before food. Review in 6 weeks with serum TSH and FT4. Supply: 30 tablets.
Patient communication — the 5 key teaching points for levothyroxine:
1. Timing: Take the tablet first thing in the morning, 30–60 minutes before breakfast. Taking it with food reduces absorption by up to 40%.
2. Interactions: Calcium supplements, iron tablets, antacids (calcium carbonate, aluminium hydroxide), cholestyramine, and some proton pump inhibitors reduce levothyroxine absorption. Separate these by at least 4 hours.
3. Lifelong medication: Hypothyroidism (in most cases, particularly Hashimoto thyroiditis and post-ablative) is permanent — the tablet cannot be stopped when you feel better. Stopping will cause hypothyroidism to return.
4. Monitoring: A blood test (TSH) must be checked 6 weeks after starting or after any dose change, and then annually once stable. Do NOT self-adjust the dose based on symptoms alone.
5. Symptoms of over-treatment: If you develop palpitations, tremor, insomnia, or unexplained weight loss, these may indicate the dose is too high — do not stop suddenly, but contact your doctor for a blood test.
Special prescribing scenarios:
- Elderly patient (72 years, no cardiac disease): Start 25 µg/day. Increase by 25 µg every 6 weeks targeting TSH 0.5–2.5 mIU/L.
- Elderly patient with known angina: Start 12.5–25 µg/day. Increase by 12.5–25 µg every 6–8 weeks. Consult cardiology before titrating further if angina worsens.
- Pregnancy (pre-existing hypothyroidism): Increase current dose by 25–30% (approximately 25–50 µg/day increment) immediately upon pregnancy confirmation. Target TSH <2.5 mIU/L (first trimester), <3.0 mIU/L (second and third trimesters).
- Secondary hypothyroidism: Titrate to FT4 in the upper half of the normal range (TSH cannot be used as a target because pituitary TSH secretion is impaired).
- Subclinical hypothyroidism with TSH 6–8 mIU/L in a woman planning pregnancy: Treat with low-dose levothyroxine (25–50 µg/day) — the ATA recommends treatment in this scenario to optimise thyroid function before conception.
Levothyroxine Prescription and Patient Instructions