Page 1 of 21
IM13.{1-4,15} | Oncology Foundations — SDL Guide
Learning Objectives
- Describe the clinical epidemiology and key risk factors (inherited and modifiable) for common malignancies in India
- Explain the genetic basis of cancer including oncogenes, tumour suppressor genes, and inherited cancer syndromes
- Describe the relationship between infection (viral, bacterial, parasitic) and specific cancers
- Outline the natural history, clinical presentation, disease course, and complications of common cancers
- Describe the rationale and tests used in cancer prevention and screening programmes
INSTRUCTIONS
Cancer is now the second leading cause of death in India and a growing public health challenge. This foundational module establishes the epidemiological, genetic, and aetiological framework that underpins all subsequent oncology learning. Mastering these concepts allows you to counsel patients on risk reduction, recognise red-flag presentations early, and understand why targeted therapies work.
References
- Harrison's Principles of Internal Medicine, 21st ed., Part 7 — Oncology (textbook)
- API Textbook of Medicine, 10th ed., Section on Oncology (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 11 — Cancer (textbook)
- ICMR–NCDIR National Cancer Registry Programme Report 2020 (guideline)
- WHO International Agency for Research on Cancer (IARC) GLOBOCAN 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajan is a 52-year-old tobacco farmer who presents to your outpatient clinic with a six-week history of hoarseness, progressive dysphagia to solids, and a 6 kg weight loss. His 70 pack-year smoking history and daily betel nut chewing are documented in his old notes. His sister died of breast cancer at 44. As you examine him you notice a firm, non-tender lymph node in the right supraclavicular fossa. Consider the layers of this single presentation: a tobacco-related carcinogen at work in the larynx and oesophagus, a nutritional consequence of mechanical obstruction, a possible inherited susceptibility hinted at by his family history, and a lymphatic spread already in progress. Every element — risk exposure, genetic background, infectious co-factor, natural history, and spread — is covered by today's module. Understanding why Rajan's cancer developed and where it is going is the first and most essential step before you can investigate or treat.
WHY THIS MATTERS
India carries a disproportionate burden of cancer: the ICMR–NCDIR 2020 report estimated 1.39 million new cancer cases annually, with projections to exceed 1.57 million by 2025. Oral cavity cancers — largely driven by tobacco and areca nut — are disproportionately common in South Asia and often present at advanced stages. Cervical cancer, which is largely preventable by vaccination and screening, remains among the top three female cancers in India. As a final-year MBBS student, you are entering a healthcare system where early cancer recognition and appropriate referral are life-saving skills. The NMC competencies IM13.1–13.4 and IM13.15 establish the foundation without which the clinical, diagnostic, and therapeutic modules cannot be meaningfully understood.
RECALL
Before proceeding, activate your prior knowledge. From your biochemistry and pathology blocks, recall the cell cycle and how mutations in proto-oncogenes and tumour suppressor genes disrupt it. Remember that the body normally controls cell proliferation through checkpoints at G1/S and G2/M; apoptotic pathways remove damaged cells. Recall from microbiology that certain viruses — such as the human papillomavirus (HPV) and hepatitis B and C viruses — can integrate into host DNA and dysregulate these controls. From your community medicine lectures, you should be familiar with the IARC carcinogen classification (Group 1 = human carcinogen), which places tobacco smoke, aflatoxin, asbestos, and ionising radiation in the highest-risk category. This module extends those concepts into the clinical epidemiological context of Indian patients.
Cancer Epidemiology in India — Burden and Risk Factors
Cancer epidemiology in India is shaped by a unique interplay of tobacco use, infectious co-factors, nutritional deficiencies, and rising non-communicable disease risk from urbanisation. Understanding the epidemiological pattern is fundamental to making early diagnoses and counselling patients on prevention, because the predominant cancers in Indian practice differ substantially from those in high-income Western settings.
The National Cancer Registry Programme (NCRP) under ICMR–NCDIR provides India's most comprehensive incidence data. The top five cancers by incidence in males are: oral cavity and lip, lung, colorectal, stomach, and oesophagus. In females: breast, cervix, colorectal, ovary, and oral cavity. This ranking differs from global patterns where prostate and colorectal cancers dominate in males; the Indian male pattern reflects the near-epidemic burden of tobacco-associated oral cancers driven by smokeless tobacco, betel quid, and areca nut consumption. Breast cancer has now overtaken cervical cancer as the commonest female cancer in urban India, though cervical cancer remains dominant in rural populations where screening penetration is low.
Modifiable risk factors account for a substantial proportion of the Indian cancer burden. Tobacco use — both smoked and smokeless (bidi, khaini, gutkha, pan masala) — is the single most important modifiable carcinogen, implicated in cancers of the oral cavity, pharynx, larynx, lung, oesophagus, stomach, bladder, kidney, and cervix. Smokeless tobacco products are particularly prevalent in India, driving the extremely high incidence of buccal mucosa carcinoma, which is rare in Western populations. Alcohol use synergises with tobacco in head-and-neck and oesophageal cancer. Areca nut (betel nut) is independently carcinogenic regardless of tobacco content; it causes oral submucous fibrosis (OSMF), a premalignant condition affecting up to 5 million Indians, and is an IARC Group 1 carcinogen for oral cancer.
Inherited (non-modifiable) risk factors include germline mutations in cancer predisposition genes. While the majority of cancers are sporadic (arising from somatic mutations only), approximately 5–10% carry a heritable component. Key examples: BRCA1/BRCA2 mutations confer a lifetime breast cancer risk of 60–80% and ovarian cancer risk of 15–40%; Lynch syndrome (mismatch repair gene mutations — MLH1, MSH2, MSH6, PMS2) predisposes to colorectal, endometrial, ovarian, and urothelial cancers; familial adenomatous polyposis (FAP) due to APC gene mutations creates hundreds of colorectal polyps with near-certain progression to carcinoma. Recognising an inherited pattern (early age at onset, multiple affected relatives, bilateral or multifocal disease) triggers referral for genetic counselling and cascade testing.
Other risk factors include obesity and physical inactivity (increasing risk of breast, endometrial, colorectal cancers), occupational carcinogens (asbestos → mesothelioma and lung cancer; benzene → leukaemia; arsenic → skin, lung, bladder), and dietary factors (aflatoxin contamination in stored grains → hepatocellular carcinoma; high salt-preserved foods → gastric cancer).
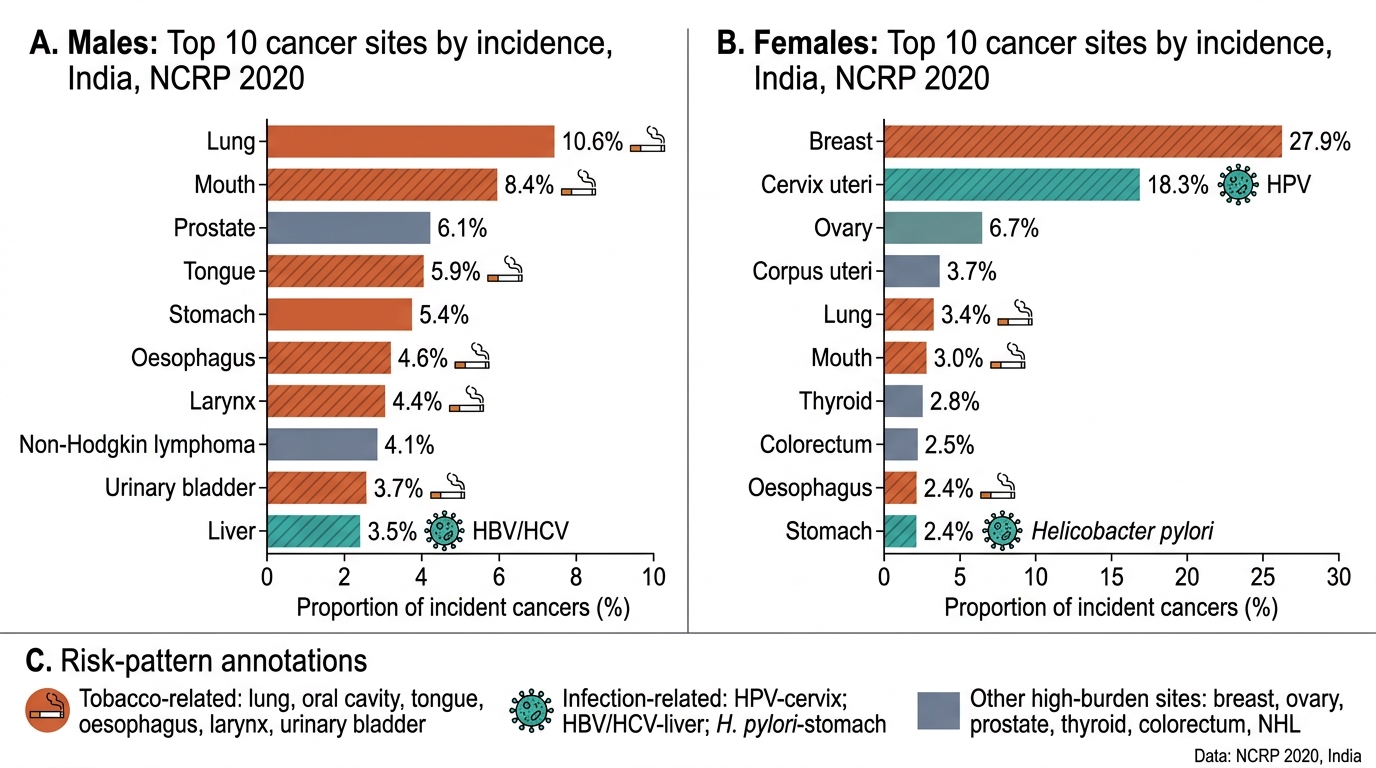
Top Cancer Sites in India by Sex, NCRP 2020
Genetic Basis of Cancer
The genetic basis of cancer rests on the principle that malignant transformation results from the accumulation of mutations in critical genes that control cell growth, differentiation, and apoptosis. No single mutation is sufficient; cancer requires the sequential acquisition of mutations across multiple pathways — the multi-hit hypothesis first articulated by Knudson in 1971 in the context of retinoblastoma. Understanding this genetic framework explains why cancer takes years to develop, why certain genetic backgrounds confer high risk, and why targeted therapies are designed against specific molecular drivers.
Proto-oncogenes are normal cellular genes that promote cell growth and proliferation. When mutated or abnormally expressed, they become oncogenes that drive uncontrolled cell division. Activation mechanisms include point mutations (e.g., RAS point mutation in codon 12 or 13 — found in ~30% of all human cancers, especially colorectal, pancreatic, and lung adenocarcinoma), gene amplification (e.g., HER2/neu (ERBB2) amplification in 15–20% of breast cancers, driving aggressive phenotype and targeted by trastuzumab), and chromosomal translocation (e.g., the Philadelphia chromosome — the t(9;22)(q34;q11) translocation that creates the BCR-ABL1 fusion protein in chronic myeloid leukaemia (CML), constitutively activating tyrosine kinase signalling; targeted by imatinib). In Burkitt lymphoma, the translocation t(8;14) places the c-MYC oncogene under immunoglobulin heavy chain promoter control, driving uncontrolled transcription of proliferative genes.
Tumour suppressor genes (TSGs) normally restrain cell division, promote apoptosis, or enable DNA repair. Their inactivation follows the Knudson two-hit model: both alleles must be inactivated (loss of heterozygosity, LOH) for function to be lost — one allele may be inherited in germline (familial), the other lost somatically. The paradigmatic TSG is TP53 (chromosome 17p13), which encodes the p53 protein — the 'guardian of the genome'. p53 is activated by DNA damage, arrests the cell cycle at G1, and triggers apoptosis if repair fails. TP53 is mutated in >50% of all human cancers. Other critical TSGs: RB1 (retinoblastoma — regulates G1/S checkpoint), BRCA1/2 (DNA double-strand break repair), APC (Wnt signalling, mutated in FAP and most sporadic colorectal cancers), VHL (renal cell carcinoma), and CDKN2A (p16 — CDK4/6 inhibitor, methylation-silenced in many cancers).
DNA mismatch repair (MMR) deficiency — the molecular basis of Lynch syndrome — leads to microsatellite instability (MSI-H), a mutational phenotype characterised by expansion or contraction of short repeat sequences. MSI-H tumours accumulate thousands of mutations per tumour (hypermutator phenotype), which paradoxically generates a high neoantigen load and makes them particularly responsive to immune checkpoint inhibitor therapy (pembrolizumab is FDA-approved for any MSI-H/dMMR solid tumour regardless of origin). Testing for MMR status by immunohistochemistry (loss of MLH1, MSH2, MSH6, or PMS2 staining) or by polymerase chain reaction (MSI testing) is now standard in colorectal cancer and increasingly in all solid tumours.
Epigenetic mechanisms also contribute to cancer without altering the DNA sequence itself: promoter methylation silences TSGs (e.g., MLH1 promoter methylation in sporadic MSI-H colorectal cancer), and histone modification alters chromatin accessibility. These mechanisms are potentially reversible and are being exploited therapeutically by DNMT inhibitors (azacitidine, decitabine) and HDAC inhibitors.
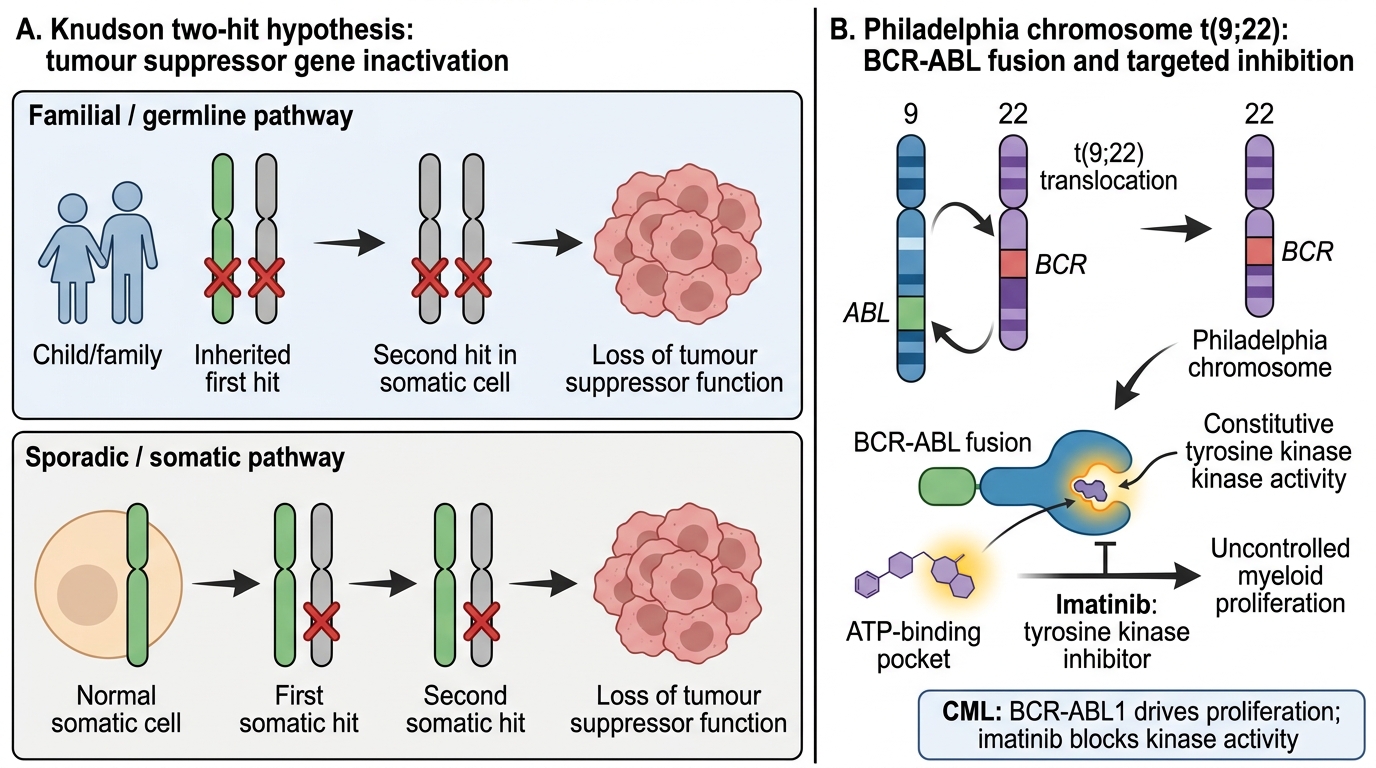
Knudson Two-Hit Hypothesis and BCR-ABL Targeted Therapy
SELF-CHECK
A 45-year-old man with chronic myeloid leukaemia (CML) has the Philadelphia chromosome confirmed on cytogenetics. The BCR-ABL1 fusion gene encodes a constitutively active tyrosine kinase. Which drug class was designed to target this specific molecular abnormality?
A. Alkylating agents (e.g., cyclophosphamide)
B. Tyrosine kinase inhibitors (e.g., imatinib)
C. Topoisomerase II inhibitors (e.g., doxorubicin)
D. Anti-metabolites (e.g., methotrexate)
Reveal Answer
Answer: B. Tyrosine kinase inhibitors (e.g., imatinib)
The BCR-ABL1 fusion protein is a constitutively active tyrosine kinase that drives uncontrolled proliferation of CML cells. Imatinib (Gleevec) — the first approved tyrosine kinase inhibitor — was designed to occupy the ATP-binding pocket of BCR-ABL1 and block its kinase activity. This targeted approach transformed CML from a disease requiring bone marrow transplantation to a chronically managed condition. Alkylating agents, anthracyclines, and antimetabolites are cytotoxic chemotherapy agents without this specificity.
Infection-Related Cancers
Infectious agents account for approximately 13–16% of the global cancer burden — and a higher proportion in low- and middle-income countries, including India, where viral hepatitis, HPV infection, and Helicobacter pylori remain prevalent. Recognising the infection–cancer link is essential for two reasons: first, it identifies preventable cancers through vaccination and treatment; second, it defines a distinct pathogenic mechanism that differs from chemical carcinogenesis.
Human papillomavirus (HPV) is the most important oncogenic virus globally. High-risk HPV types — predominantly HPV 16 and HPV 18 — account for >99% of cervical cancers, 90% of anal cancers, and a growing proportion of oropharyngeal cancers (especially base of tongue and tonsillar cancers, often in non-smokers — the HPV-positive oropharyngeal cancer epidemic). The mechanism involves the viral oncoproteins E6 (which targets p53 for proteasomal degradation) and E7 (which binds and inactivates the RB1 protein), thereby disabling the two most critical tumour suppressor pathways simultaneously. In India, cervical cancer remains one of the most common female malignancies — almost entirely attributable to HPV infection — despite the existence of effective vaccines (bivalent, quadrivalent, nonavalent) and cytological screening (Pap smear) that together can reduce cervical cancer incidence by >90%.
Hepatitis B virus (HBV) and Hepatitis C virus (HCV) are the dominant causes of hepatocellular carcinoma (HCC), one of the most common cancers in parts of India, particularly the North-East and tribal regions where chronic HBV endemicity is high. HBV integrates into the host genome and activates hepatocyte proliferation; HCV acts through chronic inflammatory damage and cirrhosis rather than direct DNA integration. The key point for prevention: HBV vaccination (part of India's Universal Immunisation Programme since 2002) is expected to dramatically reduce HCC incidence over the coming decades. Direct-acting antivirals for HCV cure the infection and significantly reduce HCC risk even in patients with established cirrhosis.
Helicobacter pylori is classified as an IARC Group 1 carcinogen for gastric cancer. Chronic H. pylori infection drives a recognised progression from chronic active gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → gastric adenocarcinoma (the Correa cascade). H. pylori is also strongly associated with mucosa-associated lymphoid tissue (MALT) lymphoma of the stomach — a low-grade B-cell lymphoma that may regress completely with H. pylori eradication therapy (triple or quadruple regimen) in early stages, making it one of the few cancers cured by antimicrobials.
Epstein-Barr virus (EBV) is associated with Burkitt lymphoma (endemic form in sub-Saharan Africa — nearly 100% EBV association; sporadic form has lower EBV association), nasopharyngeal carcinoma (particularly common in Southeast Asia and southern China; virtually 100% EBV-positive), EBV-positive diffuse large B-cell lymphoma in immunocompromised hosts, and post-transplant lymphoproliferative disorder (PTLD).
Human T-cell leukaemia virus type 1 (HTLV-1) causes adult T-cell leukaemia/lymphoma (ATLL) — endemic in Japan, the Caribbean, and parts of Africa. Other oncogenic viruses: Kaposi sarcoma herpesvirus (KSHV/HHV-8) causes Kaposi sarcoma and primary effusion lymphoma; Merkel cell polyomavirus causes Merkel cell carcinoma of the skin.
Schistosoma haematobium (a parasitic infection) is associated with squamous cell carcinoma of the bladder in endemic regions of Africa and the Middle East — a parasitic rather than viral mechanism, mediated by chronic inflammation and nitroso-compound production by the parasite.
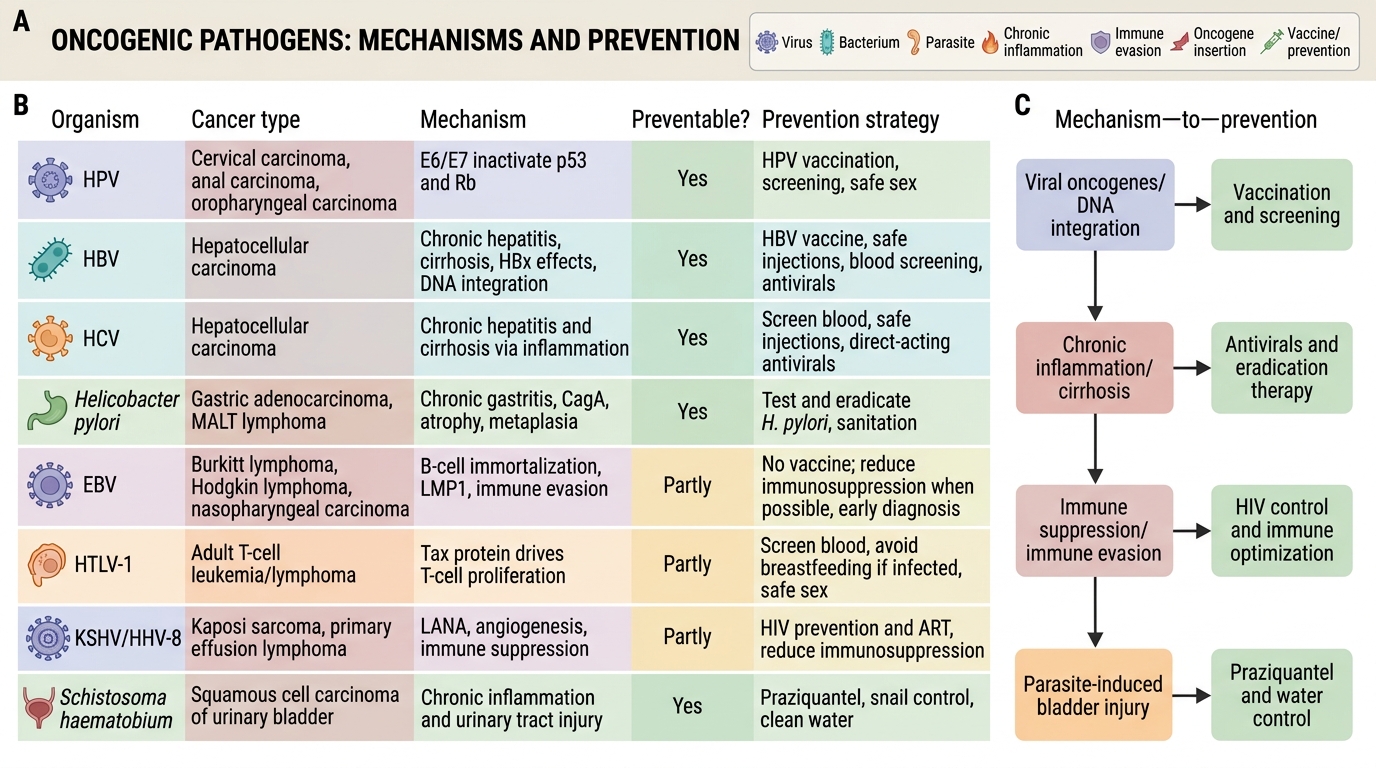
Oncogenic Infectious Agents and Cancer Prevention