Page 8 of 15
IM14.11-14 | Obesity Counselling and Treatment — SDL Guide
Learning Objectives
- Apply the 5As framework and motivational interviewing principles to deliver non-judgmental, patient-centred obesity counselling
- Prescribe evidence-based dietary and lifestyle modification for Indian patients with obesity, including caloric deficit targets, food substitution guidance, and physical activity prescription
- Identify and address barriers to adherence using empathic, non-judgmental counselling strategies
- Describe the indications, mechanisms, pharmacology, and side effects of GLP-1 receptor agonists (liraglutide, semaglutide) and orlistat, using Asian-Indian BMI thresholds for pharmacotherapy initiation
- Describe the indications, procedures, expected outcomes, and complications of bariatric surgery (sleeve gastrectomy, Roux-en-Y gastric bypass) using Asian-Indian BMI thresholds
- Develop and deliver patient and public education messages for obesity prevention at individual and community levels
INSTRUCTIONS
This module addresses the treatment and prevention competencies for obesity (IM14.11–14.14). The emphasis is on applied clinical skills: counselling technique, dietary prescription, pharmacotherapy selection, and bariatric surgery indications. The non-judgmental counselling competency (IM14.12) is as clinically important as the pharmacological knowledge and should be given equal attention. Use the scenarios in the self-assessment section to practise integrating counselling and management decisions in realistic patient contexts.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 415 — Management of Obesity (textbook)
- API Textbook of Medicine, 10th ed. — Treatment of Obesity (textbook)
- OMAI/OSSI Clinical Practice Guidelines for Management of Obesity in Indians, 2016 (guideline)
- Wilding JPH et al. Once-weekly semaglutide in adults with overweight or obesity (STEP 1). NEJM 2021;384:989–1002 (guideline)
- 2nd Diabetes Surgery Summit (DSS-II) Consensus Report: Guidelines for Metabolic Surgery, Diabetes Care 2016 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ramesh is a 48-year-old bus driver with BMI 34 kg/m² (obese by Asian-Indian criteria), waist circumference 102 cm, type 2 diabetes on metformin, and blood pressure 148/92 mmHg. He has attended the obesity clinic twice before. Both times, the consultation ended with a printed diet sheet and an instruction to 'lose weight and exercise more.' He has not returned in two years. When he finally comes back, he says: 'Doctor, every time I come here I leave feeling like a failure. I know I should eat less. I can't. My shift starts at 4 AM and ends at 8 PM. My wife packs whatever is available. I'm too tired to cook or exercise. I know it's bad for me. I just don't know where to start.' Ramesh's story illustrates the central challenge of obesity counselling: the gap between knowing and doing. This module is about bridging that gap — using evidence-based behavioural, dietary, pharmacological, and surgical tools, delivered in a non-judgmental and patient-centred way.
WHY THIS MATTERS
Competencies IM14.11–14.14 require you to counsel patients on lifestyle and behavioural modification, demonstrate an understanding of patients' inability to adhere to instructions and counsel them non-judgementally, describe pharmacotherapy and bariatric surgery options with their indications and side effects, and educate patients and the public on obesity prevention. These are among the most practically important competencies in the subject, because they are applied in almost every clinical encounter with an obese patient across all specialties. The skills developed here will determine whether your patients receive real, actionable support — or leave feeling judged, unsupported, and less likely to return.
RECALL
Recall from the Obesity Foundations module that the intervention ladder for obesity proceeds stepwise: lifestyle modification (foundation, all patients) → pharmacotherapy (added at BMI ≥27.5 with comorbidities or ≥32.5 without) → bariatric surgery (BMI ≥37.5 or ≥32.5 with major comorbidities) — using Asian-Indian BMI thresholds throughout. Recall that 5–10% total body weight loss is the minimum clinically meaningful threshold: it reduces blood pressure, improves glycaemia, lowers triglycerides, reduces hepatic fat, and decreases OSA severity. Recall from the Clinical Evaluation module that the Stages of Change model describes five stages of readiness: pre-contemplation, contemplation, preparation, action, and maintenance — and that matching the counselling intervention to the patient's stage is more effective than providing uniform advice to all patients.
The Clinical Encounter: Setting the Stage for Non-Judgmental Counselling
Effective obesity counselling begins before any dietary advice is given. The manner in which the clinician opens the conversation, frames the problem, and responds to the patient's emotional state determines whether the patient feels heard and supported — or judged and shamed. Weight stigma in healthcare is well-documented and consequential: patients who experience stigmatising interactions with healthcare providers report avoiding follow-up appointments, delaying seeking care, and engaging in compensatory eating as a response to shame. A clinician who communicates genuine interest in the patient's life circumstances, acknowledges the complexity of the problem, and avoids moral judgement about weight is more likely to build a therapeutic alliance that sustains behaviour change.
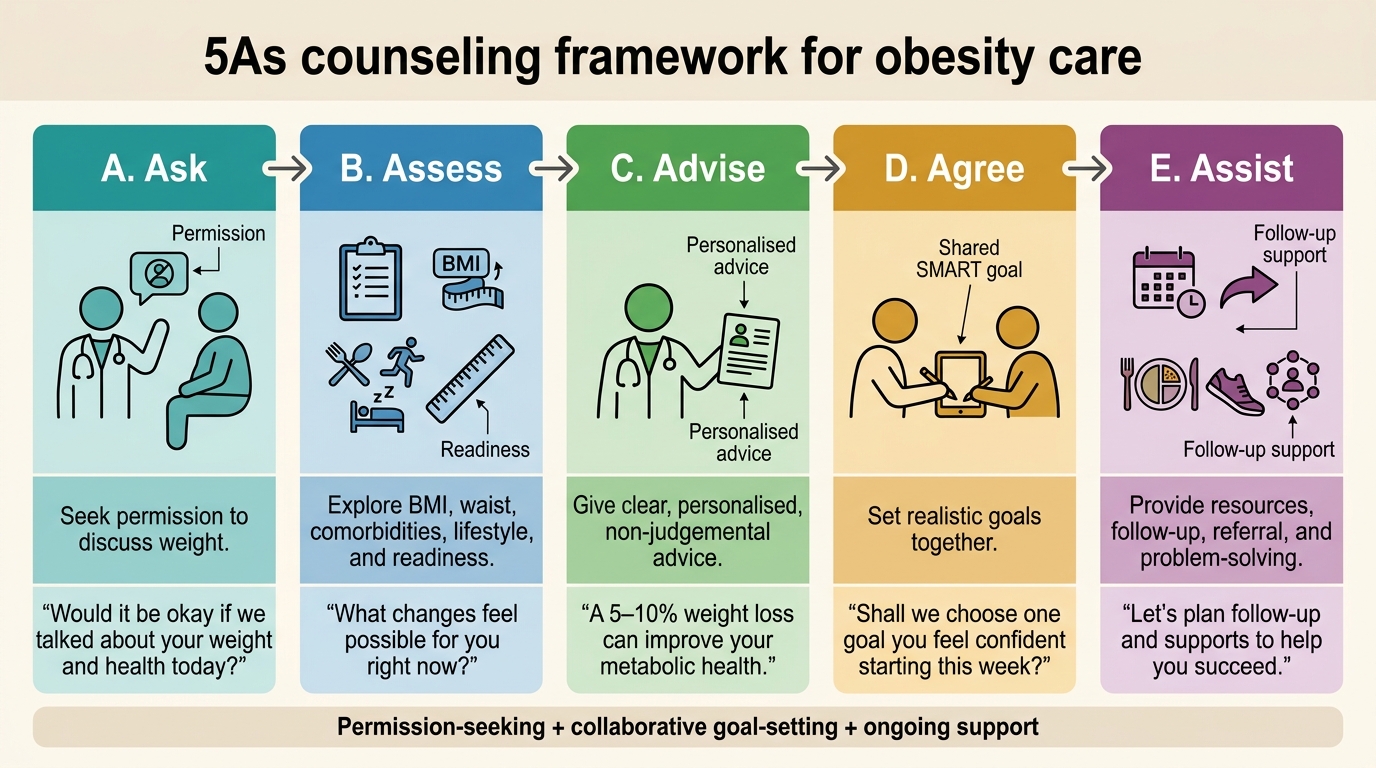
The 5As framework is a structured, evidence-based approach to brief obesity counselling that can be applied in any clinical setting within a 5–10 minute consultation:
1. Ask: 'Would it be alright if we discussed your weight today?' — always seek permission first; this respects autonomy and avoids the patient feeling ambushed.
2. Assess: Assess BMI, waist circumference, current comorbidities, barriers, and stage of readiness to change.
3. Advise: Provide clear, personalised, non-judgmental advice on the health risks of current weight and the benefits of even modest weight loss.
4. Agree: Collaboratively set a realistic, specific, and time-bound goal with the patient ('Let us aim for 3 kg over the next 6 weeks by reducing one soft drink per day and adding a 15-minute evening walk') — goals imposed unilaterally are unlikely to be pursued.
5. Assist: Provide concrete resources, refer to a dietitian or structured weight loss programme, schedule follow-up, and address barriers proactively.
Language matters. Current best practice (endorsed by the Canadian Obesity Network and Obesity Medicine Association) recommends person-first language: 'person with obesity' rather than 'obese person'; 'high BMI' rather than 'fat.' Avoid phrases like 'you need to try harder,' 'just eat less and move more,' or 'your weight is your fault.' These phrases reflect weight bias and are empirically counterproductive.
5As Framework for Obesity Counselling
Dietary and Lifestyle Modification: Evidence-Based Approaches
Lifestyle modification — encompassing dietary change, increased physical activity, and behavioural strategies — is the foundation of obesity treatment and the prerequisite for all other interventions. It must be the first treatment modality offered and must be continued as a background therapy even when pharmacotherapy or bariatric surgery is added. The evidence base for lifestyle modification has matured substantially over the past two decades, moving from simplistic 'eat less, move more' messaging to a structured understanding of which dietary patterns, activity prescriptions, and behavioural supports produce clinically meaningful, sustained weight loss.
Dietary therapy — principles and approaches:
The fundamental therapeutic goal is creating a sustained caloric deficit of 500–750 kcal/day below total daily energy expenditure (TDEE). This produces an expected weight loss of approximately 0.5–0.75 kg/week and 4–8 kg over 6 months. Critically, the specific macronutrient composition of the diet is less important than the size of the caloric deficit and the patient's ability to sustain the dietary pattern — there is no evidence that any single 'diet type' (low-fat, low-carbohydrate, Mediterranean, high-protein) is superior for weight loss when total caloric restriction is matched.
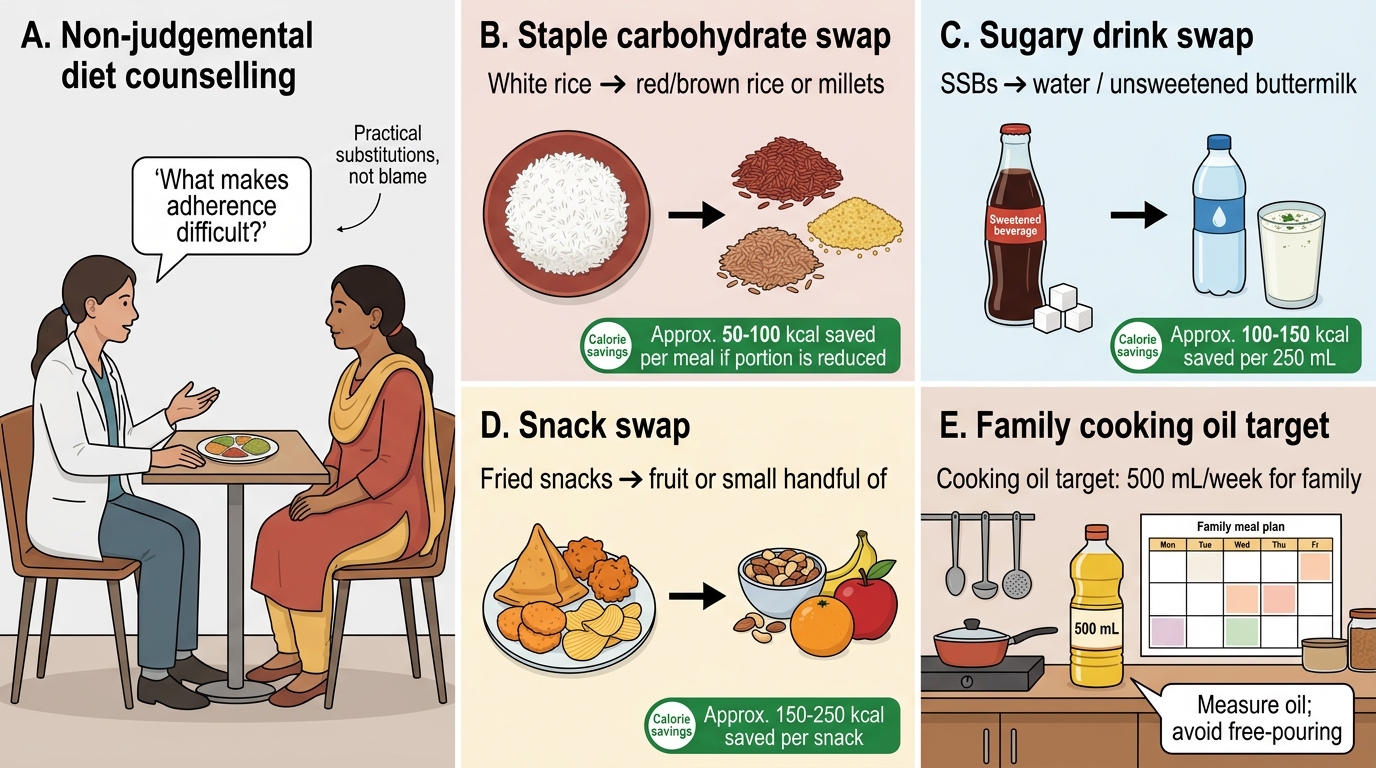
For practical counselling of Indian patients, however, dietary composition guidance is necessary because the traditional Indian diet is often high in refined carbohydrates (white rice, maida-based products), cooking oil, and sugar-sweetened beverages — and reducing these specifically produces both caloric deficit and metabolic benefit:
- Reduce refined carbohydrates: substitute white rice for red/brown rice, millets, oats, or whole wheat. Reduce maida-based products (bread, biscuits, bakery items). Limit potatoes and sugary fruits.
- Eliminate or drastically reduce sugar-sweetened beverages (SSBs): each 350 mL serving of cola contains approximately 150 kcal and 38 g sugar. Eliminating 2 SSBs/day removes 300 kcal and 76 g sugar daily — a major and often underestimated intervention.
- Reduce cooking oil: measuring oil (target ≤3–4 teaspoons/person/day for cooking) rather than pouring freely from a container is a simple, high-impact change.
- Increase dietary fibre: vegetables, whole pulses (dal), fruits (in moderation), and whole grains improve satiety and slow carbohydrate absorption.
- Protein adequacy: adequate dietary protein (0.8–1.2 g/kg lean body weight/day) is important to preserve lean muscle mass during caloric restriction.
- Meal timing and frequency: irregular meal patterns, skipped breakfast, and large late-night meals are associated with adverse metabolic profiles independent of caloric content; structured 3-meal patterns with limited snacking are recommended.
Physical activity prescription:
The WHO recommends for weight management: ≥150–300 minutes/week of moderate-intensity aerobic activity (brisk walking, cycling, swimming). For clinically significant weight loss (as distinct from weight maintenance), ≥300 minutes/week is more effective. Resistance/strength training (2–3 sessions/week) is important adjunctively to preserve lean muscle mass during caloric restriction and improve insulin sensitivity. For patients who are significantly deconditioned or have orthopaedic limitations (knee/hip osteoarthritis is common in obese patients), low-impact options should be prescribed: swimming, water aerobics, recumbent cycling, yoga.
A practical counselling principle for sedentary patients: begin with achievable goals — even 10–15 minutes of walking twice daily is a meaningful starting point for a patient who has been entirely sedentary. Incremental increase (the '10% rule' — increase activity duration by no more than 10% per week) prevents injury and dropout. The 'active breaks' strategy — standing for 2 minutes every 30 minutes of sitting — has measurable metabolic benefit and is achievable by patients with sedentary occupations.
Behavioural strategies:
- Self-monitoring: keeping a food diary, step counter, or app-based calorie tracker is one of the most consistently effective predictors of long-term weight loss maintenance.
- Goal-setting: SMART goals (Specific, Measurable, Achievable, Relevant, Time-bound) — 'I will walk for 20 minutes after dinner every weekday this week' is more actionable than 'I will exercise more.'
- Stimulus control: removing high-calorie foods from the home, not keeping SSBs in the refrigerator, serving food on smaller plates.
- Cognitive behavioural therapy (CBT): structured CBT addressing food-related thought patterns, emotional eating triggers, and body image distress is the evidence-based psychological intervention for obesity, particularly when there is associated binge eating disorder or emotional eating.
Practical Dietary Substitutions for Obesity Management
Understanding and Managing Non-Adherence: The Non-Judgemental Approach
Non-adherence to lifestyle modification is not primarily a motivational failure. It is the expected and well-documented outcome of a biological system designed for survival in food-scarce environments encountering an intervention that requires chronic caloric restriction in a food-abundant environment with multiple social, occupational, and psychological barriers. Understanding this framing — shifting from 'why doesn't the patient try harder' to 'what is making adherence difficult' — is the clinical foundation of effective obesity management and the competency described in IM14.12.
Why adherence is biologically difficult:
During caloric restriction, compensatory neuroendocrine mechanisms activate to resist weight loss: leptin levels fall, activating hypothalamic hunger circuits; ghrelin (the orexigenic gut hormone) rises; resting metabolic rate falls as lean mass is partially lost; and the hedonic reward value of calorie-dense food increases through changes in mesolimbic dopamine signalling. These adaptations are robust and persistent — studies show that 1 year after diet-induced weight loss, the hormone profile promoting hunger and reducing satiety is still actively opposing maintenance. This explains why the common instruction 'just maintain the calorie deficit you used to lose weight' is physiologically more demanding than losing the weight in the first place.
Common barriers to adherence in Indian patients and how to address them:
| Barrier | Non-Judgemental Exploration | Practical Strategy |
|---|---|---|
| Long working hours (shift work, like Ramesh's 4 AM–8 PM bus driver schedule) | 'Tell me about your typical workday — when do you eat?' | Structured meal prep on rest days; healthy options in workplace canteen; small frequent meals if schedule allows |
| Food prepared by family members | 'Does your family cook for you? Do they know about the changes you are trying to make?' | Involve family in dietary change; frame changes for the whole family's health |
| Financial constraints (healthy food perceived as expensive) | 'How easy is it to access fresh vegetables and pulses where you live?' | Budget-friendly guidance: dals/pulses are cheap protein; seasonal vegetables; reducing SSBs saves money |
| Emotional/stress eating | 'Do you notice that you eat more when you are stressed or upset?' | CBT referral if available; mindful eating techniques; address the underlying stressor |
| Cultural and social pressures | 'Are there situations at family gatherings or festivals where it is hard to control portions?' | Permission to participate; harm reduction ('have one serving, not three'); timing of celebrations |
| Physical barriers (knee pain limiting walking) | 'Does your weight make it painful to exercise?' | Refer to physiotherapy; low-impact alternatives (swimming, chair exercises, water aerobics) |
| Previous failed attempts | 'What has worked in the past, even a little? What got in the way?' | Validate previous effort; reframe 'failure' as information; start with the most achievable change |
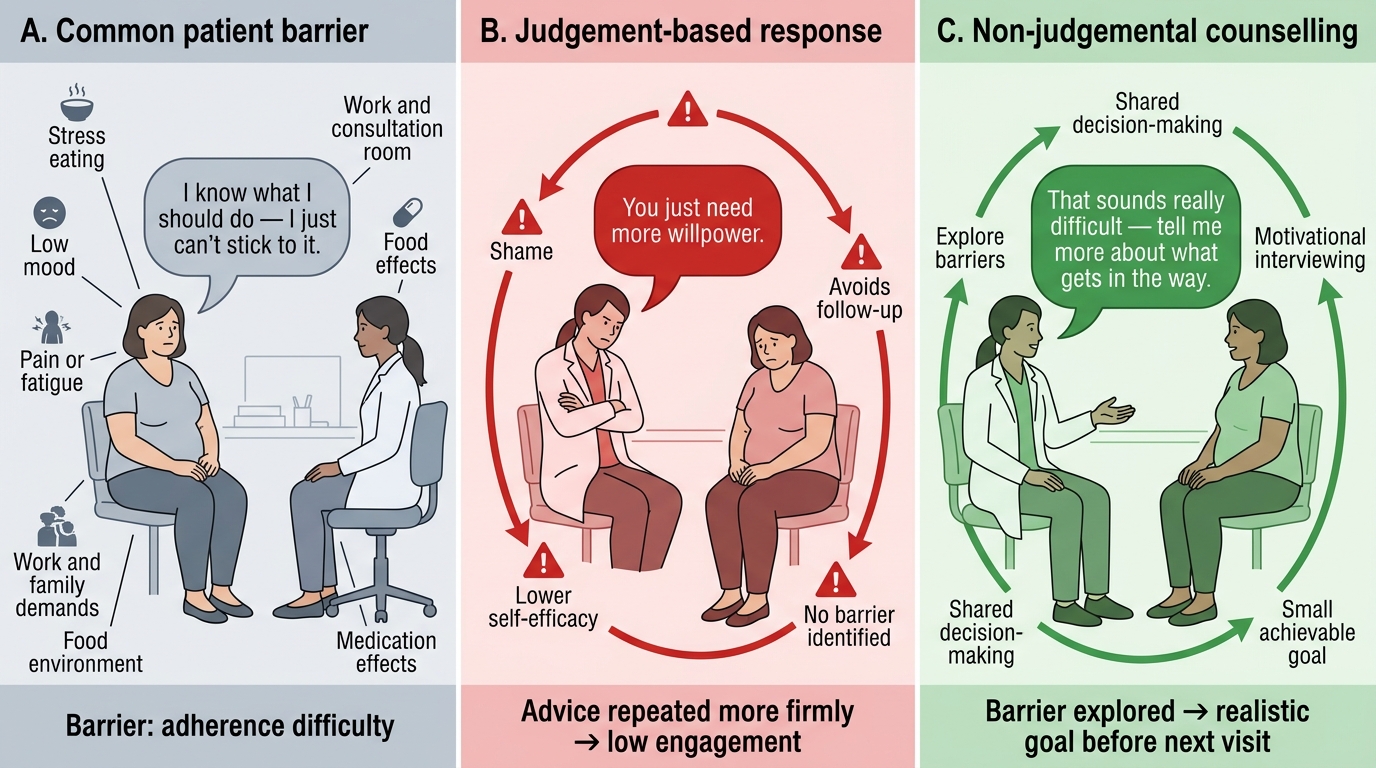
The key counselling principle: approach each barrier with curiosity, not judgement. The clinician's role is to explore and problem-solve, not to prescribe and monitor compliance. Phrases that close down the conversation — 'you just need more willpower,' 'you know what to eat, you just have to do it,' 'this is very simple' — are invalidating and empirically counterproductive. Phrases that open it up: 'that sounds really difficult — what has made it hard to walk regularly?'; 'you're dealing with a lot — which of these changes feels most manageable to start with?'
Motivational Interviewing (MI) is an evidence-based counselling technique particularly effective for behaviour change in obesity. Key MI principles: express empathy (reflective listening, acknowledging ambivalence), develop discrepancy (help patients articulate the gap between their current behaviour and their stated goals), roll with resistance (do not argue; explore ambivalence), and support self-efficacy (build confidence in small achievable steps). Studies show that MI-based obesity counselling produces significantly better weight loss outcomes than traditional didactic advice.
Judgement-Based vs Non-Judgemental Obesity Counselling
SELF-CHECK
A 38-year-old woman with BMI 33 kg/m² and type 2 diabetes has attended the obesity clinic four times in the past year. Each time, she is advised to eat less and exercise more. She has lost no weight. She says: 'I know what I should do — I just can't stick to it.' The most effective next step in her management is:
A. Repeat the dietary advice more firmly, explaining the serious health consequences of continuing to fail to lose weight
B. Start anti-obesity pharmacotherapy with a GLP-1 receptor agonist immediately, as lifestyle modification has clearly failed
C. Explore specific barriers to adherence using motivational interviewing and collaboratively set a small, achievable goal she can realistically accomplish before her next visit
D. Refer her for bariatric surgery assessment, as she has been non-compliant with all conservative management
Reveal Answer
Answer: C. Explore specific barriers to adherence using motivational interviewing and collaboratively set a small, achievable goal she can realistically accomplish before her next visit
Repeating the same advice more firmly ignores the well-established evidence that most barriers to adherence are practical and psychosocial rather than motivational, and that repetitive generic advice without exploring barriers is ineffective. Pharmacotherapy is an option but should be used alongside — not instead of — understanding and addressing barriers; it is not the first step when the behavioural component has not been properly addressed. Bariatric surgery referral requires documented failure of a structured lifestyle programme, not simply repeated generic advice that was never personalised. The correct step is to explore barriers using motivational interviewing, understand what specifically makes adherence difficult for this patient, and agree on a small, specific, achievable goal for the next 2–4 weeks.