Page 2 of 19
IM15.{1-3,6} | GI Bleeding Foundations and Stabilisation — SDL Guide (Part 2)
Initial Risk Stratification: Glasgow-Blatchford and Rockall Scores
Before selecting investigations and treatment, every patient with acute GI bleeding should undergo rapid risk stratification using validated clinical scoring systems. These scores operationalise the clinical data already collected during history and physical examination into a numerical estimate of risk that drives the timing and urgency of investigation and treatment. Understanding the purpose, inputs, and clinical application of the two principal scores — the Glasgow-Blatchford Score (pre-endoscopy) and the Rockall Score (post-endoscopy) — is required at the KH level and directly governs clinical decision-making.
The Glasgow-Blatchford Score (GBS) is a pre-endoscopy triage tool that uses data available at the bedside and from simple first-line blood tests to categorise patients with UGIB into low-risk (suitable for outpatient management or early discharge) versus high-risk (requiring admission and urgent intervention). The score incorporates: blood urea nitrogen (BUN) range, haemoglobin (sex-specific range), systolic blood pressure, pulse rate, and clinical features including melaena, syncope, hepatic disease, and cardiac failure. Each variable contributes weighted points (BUN and Hb have the highest weighting). A total score of 0–1 identifies patients at very low risk of needing any clinical intervention — these patients can safely be considered for outpatient management or early discharge with planned outpatient endoscopy. A score of ≥6 indicates high risk for clinical intervention (transfusion, endoscopic haemostasis, or surgery) and mandates admission and urgent endoscopy. The GBS has a sensitivity of approximately 99% for identifying patients requiring intervention at the ≥1 threshold, meaning almost no patient who needs intervention will be sent home if the score is correctly applied.
The Rockall Score is a post-endoscopy prognostic tool that predicts 30-day mortality and rebleeding risk after endoscopy. It requires both clinical pre-endoscopy variables (age, haemodynamic shock, comorbidities) and the endoscopic findings (diagnosis — varices and cancers score highest; stigmata of recent haemorrhage by Forrest classification). A combined Rockall score of 0–2 indicates low risk of rebleeding and low mortality; a score ≥5 carries a significant rebleeding risk and moderate mortality that warrants close inpatient monitoring. These two scores are sequential and complementary: use GBS first (do I admit this patient? how urgently do I need to scope?) and Rockall after OGD (what is this patient's ongoing risk of rebleeding and death?).
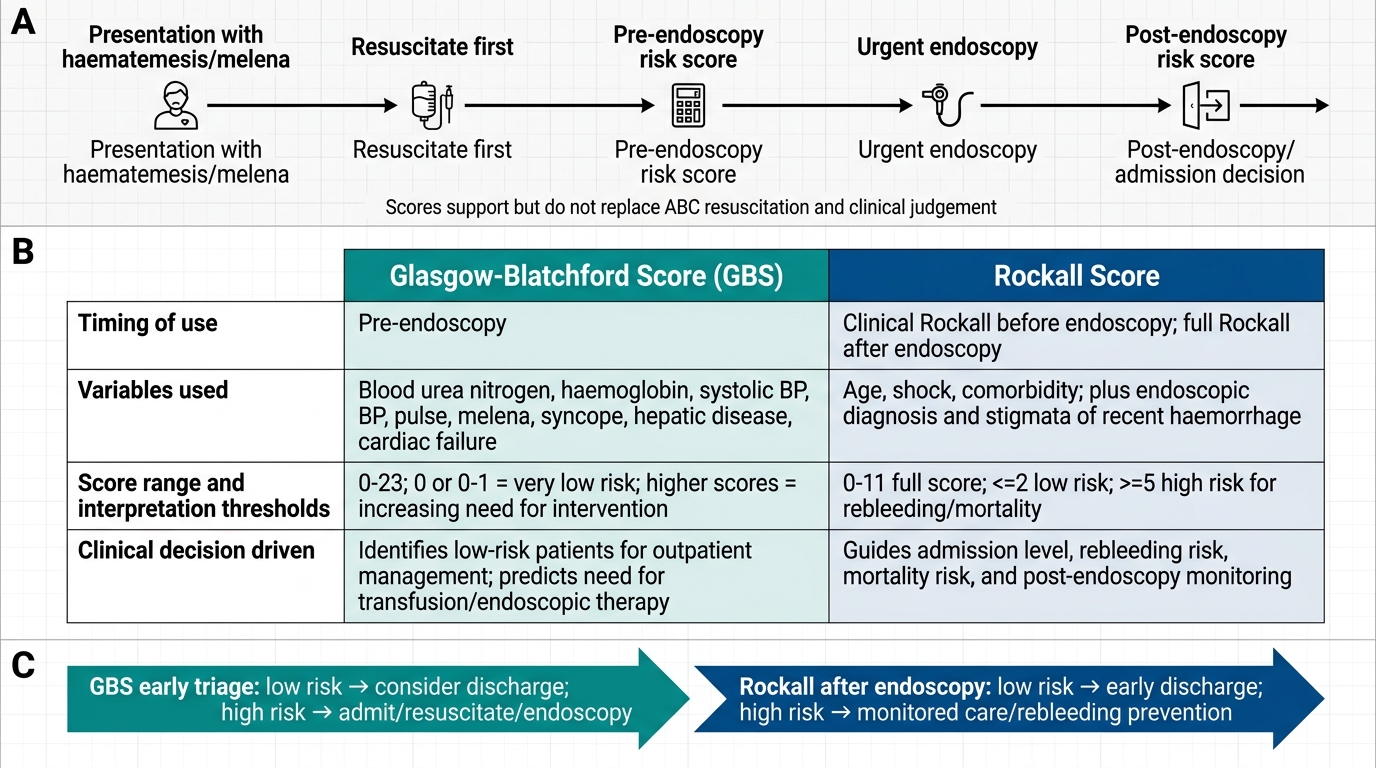
Glasgow-Blatchford vs Rockall Score in GI Bleeding
Stabilisation of the Acute GI Bleed: Systematic Approach
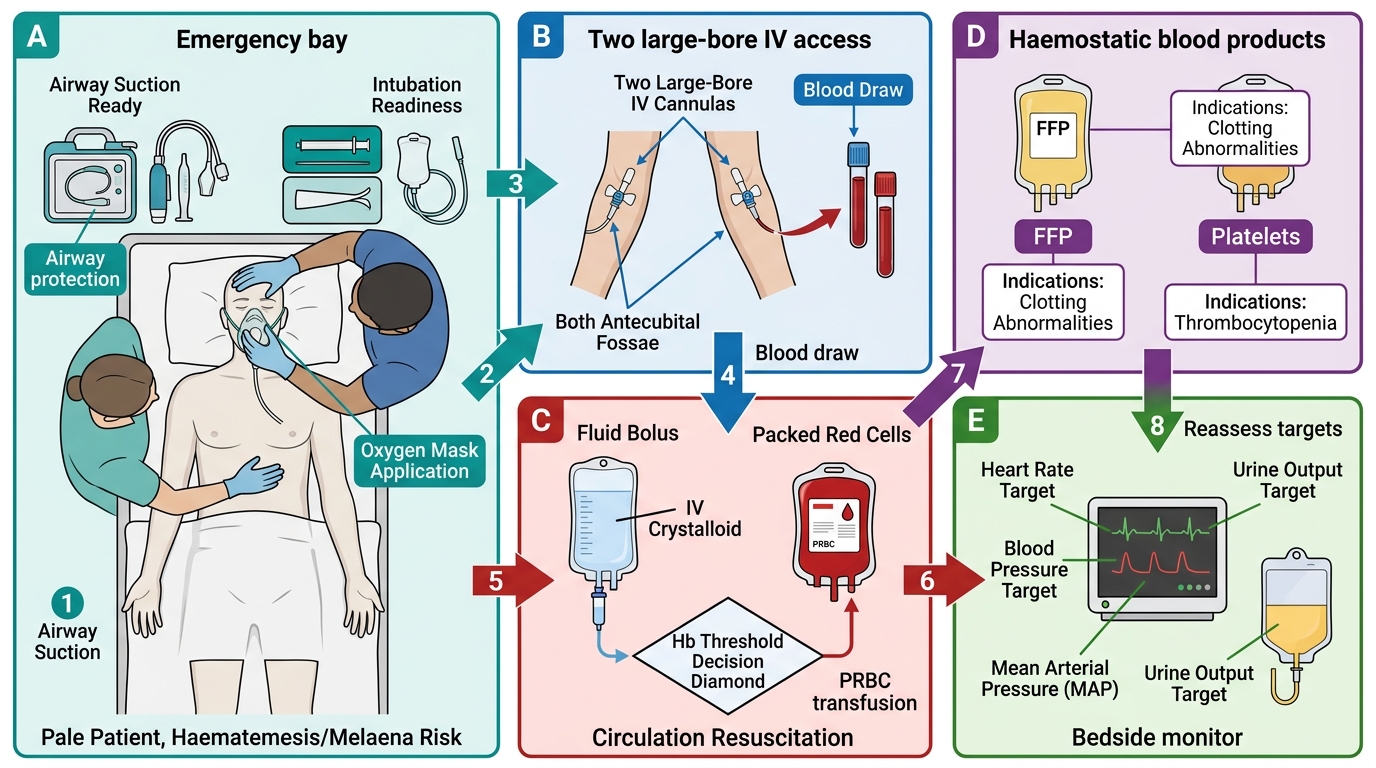
Stabilisation of the acutely bleeding patient follows a structured primary survey approach that must be executed rapidly and simultaneously by the medical team. The mnemonic 'resuscitate first, then diagnose' captures the correct priority order: no investigation — not even a blood test — should delay the initiation of IV access and volume resuscitation in a haemodynamically unstable patient. The following sequence is evidence-based and maps directly to NMC competency IM15.2.
Step 1 — Airway and Breathing: In a patient with active haematemesis, the airway is the immediate priority. Massive haematemesis can cause aspiration of blood into the tracheobronchial tree, causing airway obstruction and aspiration pneumonia. Position the patient sitting up or in the left lateral decubitus position (recovery position) to minimise aspiration risk. If the patient cannot protect their airway (altered consciousness, profuse continuous haematemesis, or GCS <8), urgent endotracheal intubation should be arranged with senior/anaesthetic assistance before endoscopy. Supplemental oxygen via face mask or nasal prongs should be given immediately to all patients — tissue oxygen delivery is doubly compromised by both anaemia (reduced oxygen-carrying capacity) and reduced cardiac output (low perfusion pressure).
Step 2 — Two large-bore IV cannulae: Establish two large-bore peripheral IV cannulae (minimum 16 gauge, ideally 14 gauge) immediately. The flow rate through a cannula is proportional to its radius to the fourth power (Poiseuille's law), so a large-bore peripheral cannula delivers fluid far faster than a central venous line of smaller bore. Central venous access (internal jugular or subclavian) is reserved for monitoring CVP in refractory shock, not as the primary resuscitation route. At the time of IV insertion, draw blood for: full blood count, urea and electrolytes, liver function tests, coagulation profile (PT, aPTT, INR), blood grouping and crossmatch (6 units), blood glucose, and a lactate measurement.
Step 3 — Fluid resuscitation: Begin crystalloid infusion (normal saline or Ringer's lactate) immediately while awaiting blood products. The target in haemorrhagic shock is restoration of organ perfusion: aim for a mean arterial pressure (MAP) of ≥65 mmHg and urine output of ≥0.5 mL/kg/hour as markers of adequate end-organ perfusion. However, avoid excessive crystalloid resuscitation ('permissive hypotension' or targeted resuscitation is preferred in uncontrolled haemorrhagic shock until the bleeding source is controlled, to avoid diluting clotting factors and worsening coagulopathy). In variceal bleeding particularly, aggressive fluid resuscitation raises portal pressure and may precipitate rebleeding — a MAP of 65–80 mmHg is the target, not supra-normal pressure.
Step 4 — Blood and blood product transfusion: The transfusion threshold for acute GI bleeding is one of the most impactful evidence-based decisions in acute medicine. A restrictive transfusion strategy — transfusing only when haemoglobin falls below 7 g/dL in haemodynamically stable patients — has been shown in the landmark TRICC trial and subsequent studies to reduce mortality, rebleeding rates, and length of stay compared with a liberal strategy (threshold Hb 9 g/dL). The threshold is raised to 8 g/dL in patients with known significant cardiovascular disease (ischaemic heart disease, heart failure), where myocardial oxygen demand is higher and anaemia tolerance is reduced. In the actively bleeding, haemodynamically unstable patient, packed red cells should be transfused without waiting for the haemoglobin result. Fresh frozen plasma (FFP) is indicated if INR >1.5 — typically given as 4 units FFP alongside every 6 units of packed red cells in massive transfusion. Platelets should be transfused if the count falls below 50 × 10⁹/L in active bleeding, or below 100 × 10⁹/L if the patient has a traumatic brain injury. Cryoprecipitate is given if fibrinogen falls below 1.0–1.5 g/L. Vitamin K (IV phytomenadione) should be given if the patient is on warfarin or has liver disease causing factor deficiency.
Acute GI Bleeding Resuscitation Algorithm
Step 5 — Monitoring and escalation: Insert a urinary catheter to monitor urine output hourly — it is the most reliable bedside indicator of renal perfusion. Apply continuous ECG monitoring and pulse oximetry. A nasogastric tube can be placed to confirm blood in the stomach and facilitate lavage but should NOT be used as a primary resuscitative measure or to estimate blood loss. Liaise early with gastroenterology (for urgent endoscopy), haematology (for massive transfusion protocol activation), and surgical and ICU teams for patients with ongoing haemodynamic instability. The decision to escalate to the ICU should be made early in patients with haemodynamic instability unresponsive to initial resuscitation, suspected variceal bleeding with decompensated liver disease, or suspicion of arterial haemorrhage.
SELF-CHECK
A 58-year-old woman with ischaemic heart disease presents with haematemesis and haemoglobin of 7.8 g/dL. She is haemodynamically stable (BP 110/70, pulse 88). What is the appropriate transfusion threshold in this patient?
A. Hb <6 g/dL — she is stable so transfusion is not yet needed
B. Hb <7 g/dL — the standard restrictive threshold for all GI bleed patients
C. Hb <8 g/dL — because her cardiovascular disease raises the transfusion threshold
D. Hb <10 g/dL — older patients with cardiac disease need near-normal haemoglobin
Reveal Answer
Answer: C. Hb <8 g/dL — because her cardiovascular disease raises the transfusion threshold
The restrictive transfusion threshold of Hb 7 g/dL applies to haemodynamically stable patients without significant cardiovascular disease and has been shown to reduce mortality and rebleeding compared to liberal strategies. However, the threshold is raised to 8 g/dL in patients with cardiovascular disease (ischaemic heart disease, heart failure) because myocardial oxygen demand is higher and these patients tolerate anaemia less well. This patient has ischaemic heart disease and her Hb is 7.8 g/dL — she meets the raised CVD-adjusted threshold. Hb 10 g/dL is not evidence-supported and corresponds to the old liberal strategy shown to be harmful.
SELF-CHECK
A 50-year-old man with known alcoholic cirrhosis presents with massive haematemesis, BP 72/40 mmHg, and pulse 130 bpm. Two large-bore IV cannulae are inserted and blood sent for grouping. What is the MOST appropriate immediate next step while awaiting crossmatched blood?
A. Emergency upper GI endoscopy to identify and treat the bleeding source
B. IV omeprazole infusion to reduce gastric acid
C. IV crystalloid (normal saline or Ringer's lactate) bolus resuscitation to restore perfusion pressure
D. Oral propranolol to reduce portal pressure
Reveal Answer
Answer: C. IV crystalloid (normal saline or Ringer's lactate) bolus resuscitation to restore perfusion pressure
The immediate priority in haemodynamic shock is restoration of circulating volume and organ perfusion pressure — resuscitate FIRST, then diagnose and treat the source. Crystalloid bolus (normal saline or Ringer's lactate) should be started immediately while awaiting crossmatched blood. Endoscopy in an actively haemodynamically unstable patient is dangerous and should only be done once the patient is stabilised. IV PPI may be added but does not replace volume resuscitation. Oral propranolol is a secondary prophylactic measure and is absolutely contraindicated in active haemorrhage and hypotension.
CLINICAL PEARL
Two deceptive bedside errors kill patients with GI bleeding. First, the haematocrit misleads early — in the first 4–6 hours after acute haemorrhage, compensatory vasoconstriction maintains haematocrit at near-normal values even when 30% of blood volume has been lost. Do not use the initial Hb or haematocrit alone to estimate blood loss; use haemodynamics (heart rate, blood pressure, pulse pressure, capillary refill, mental state) alongside lactate as your shock gauge. Second, beta-blockers mask tachycardia — a cirrhotic patient on propranolol for portal hypertension cannot mount the expected tachycardic response to haemorrhage; you may see a heart rate of only 70 bpm in a patient who is in moderate haemorrhagic shock. Always interpret heart rate in the context of the patient's medication list.
Self-Assessment: Integrating Foundations and Stabilisation
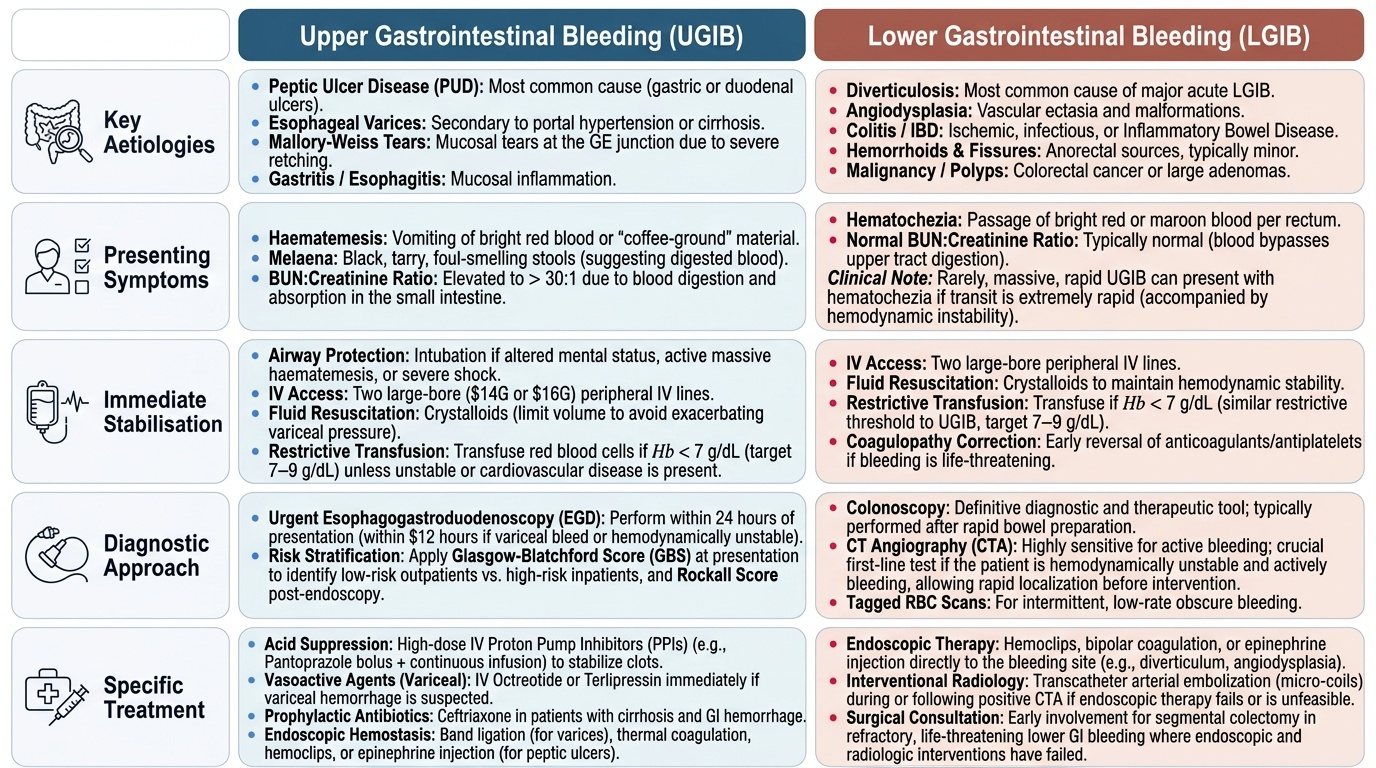
At this point in the module you have covered the clinical features that distinguish upper from lower GI bleeding, the major aetiological categories, the pathophysiology of haemorrhagic shock across its four phases, and the structured stabilisation approach with specific evidence-based decisions (transfusion thresholds, fluid choice, blood product triggers). The self-assessment scenarios below are designed to consolidate your pattern recognition and decision-making under the kind of time pressure you will face in clinical practice. For each case, work through the clinical reasoning before reading the analysis — the goal is to integrate the anatomical localisation, the aetiological probability, the shock phase assessment, and the correct first interventions as a seamless clinical unit. Apply the Glasgow-Blatchford and Rockall frameworks to each case as you reason through the management.
Provided image
Scenario A: A 68-year-old man on aspirin and ibuprofen for osteoarthritis presents to the emergency department with haematemesis and melaena. His BP is 95/60 mmHg, pulse 112 bpm, and he is confused. His Hb is 7.1 g/dL, INR 1.1, platelets 220 × 10⁹/L. BUN:creatinine ratio is 32:1. Identify: (1) the probable source and aetiology, (2) the shock phase, and (3) the three most immediate interventions.
Analysis: Source = upper GI (haematemesis + melaena + elevated BUN:creatinine ratio). Aetiology = almost certainly peptic ulcer disease (NSAID use, haematemesis/melaena without liver stigmata). Shock phase = phase 2–3 (hypotension, tachycardia, confusion — 30% or more blood volume loss). Immediate interventions: (1) airway protection — position patient, assess need for intubation given confusion; (2) two large-bore IV lines and blood draw for FBC/U&E/LFTs/coags/group-and-crossmatch; (3) IV crystalloid bolus followed by packed red cells (Hb is 7.1 — near threshold; active haemodynamic instability means transfuse now, do not wait for the threshold).
Scenario B: A 72-year-old woman with no prior abdominal history develops sudden painless passage of a large volume of maroon blood per rectum. Her BP is 115/75 mmHg, pulse 92 bpm, and she is alert. Hb is 10.3 g/dL. BUN:creatinine ratio is 9:1. No haematemesis. Identify: (1) the probable source and aetiology, (2) the shock assessment, (3) the appropriate immediate management and investigation priority.
Analysis: Source = lower GI (haematochezia without haematemesis, normal BUN:creatinine ratio, acute painless presentation in elderly patient). Aetiology = most likely diverticular bleeding given age, acute painless large-volume haematochezia — though angiodysplasia and colorectal carcinoma must also be considered. Shock assessment = compensated / minimal (mild tachycardia, preserved BP, alert) — phase 1 at most. Management: IV access, blood tests (including crossmatch), monitor with urine output and serial haematocrit; blood transfusion not immediately indicated (Hb 10.3 g/dL, haemodynamically stable); early colonoscopy after bowel preparation is the investigation of choice once stabilised. Note: haemorrhage ceases spontaneously in ~80% of diverticular bleeds.