Page 8 of 19
IM15.{9-10,16} | GI Bleeding Investigations — SDL Guide
Learning Objectives
- Choose and interpret baseline laboratory investigations in GI bleeding including CBC, PT/aPTT, stool examination, occult blood, LFTs, and H. pylori testing
- Enumerate the indications for endoscopy and colonoscopy in the investigation of upper and lower GI bleeding
- Identify the indications for other imaging modalities including CT angiography, nuclear medicine scanning, and angiography
- Enumerate the indications for endoscopic intervention and surgery in GI bleeding
INSTRUCTIONS
Investigations in GI bleeding serve two parallel purposes: characterising the severity of the physiological derangement and identifying the source of bleeding to enable targeted treatment. This module guides you through the rational selection and interpretation of the investigation ladder, from bedside tests to endoscopy to advanced imaging.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 47 — Gastrointestinal Bleeding (textbook)
- API Textbook of Medicine, 10th ed. — Gastrointestinal Haemorrhage (textbook)
- British Society of Gastroenterology: UK guidelines on the management of upper gastrointestinal bleeding, 2021 (guideline)
- American College of Gastroenterology guidelines on lower GI bleeding, 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man with melaena is brought to the emergency department. A junior doctor orders 14 blood tests, CT abdomen, chest X-ray, ECG, and an immediate upper GI endoscopy — simultaneously. The endoscopy suite nurse calls to say the patient needs to be haemodynamically stable before endoscopy can proceed safely. The CT radiologist asks what contrast protocol to use. Meanwhile the blood count result comes back showing haemoglobin of 6.2 g/dL and INR of 1.8. The problem is not a lack of investigations — it is a lack of a rational framework for sequencing them. In GI bleeding, the question is never 'what investigations should we do?' but 'which investigation will give the most clinically actionable information right now?' Getting this sequencing right separates the effective clinician from one who generates data without direction.
WHY THIS MATTERS
NMC competencies IM15.9, IM15.10, and IM15.16 require you to choose and interpret diagnostic tests, enumerate endoscopy indications, and identify when endoscopic or surgical intervention is required — reflecting that the investigation phase is not passive data-collection but active clinical decision-making. In India, where many centres lack 24-hour endoscopy services, understanding the exact conditions under which urgent endoscopy is warranted (versus what can wait until morning) is clinically critical. Similarly, knowing when to escalate from endoscopy to angiography or surgery can be the difference between a salvageable haemorrhage and death. The investigation decisions you make in the first hour of a GI bleed patient's care set the trajectory of the entire admission.
RECALL
Recall the Glasgow-Blatchford Score for UGIB risk stratification — it uses BUN, haemoglobin, systolic blood pressure, pulse rate, and clinical features. Recall the Rockall Score for post-endoscopy risk assessment of UGIB — it combines clinical variables (age, shock, comorbidities) with endoscopic findings (diagnosis, stigmata of recent haemorrhage) to predict mortality and rebleeding risk. Recall the Forrest classification of peptic ulcer stigmata seen at endoscopy: Forrest Ia (spurting artery, highest rebleeding risk ~55%), Ib (oozing), IIa (visible non-bleeding vessel, ~43%), IIb (adherent clot), IIc (flat pigmented spot), III (clean base, <5% rebleed). These three classification systems — Glasgow-Blatchford, Rockall, and Forrest — are the backbone of GI bleed risk stratification and appear in almost every clinical guideline.
Clinical Indication for Investigation in GI Bleeding
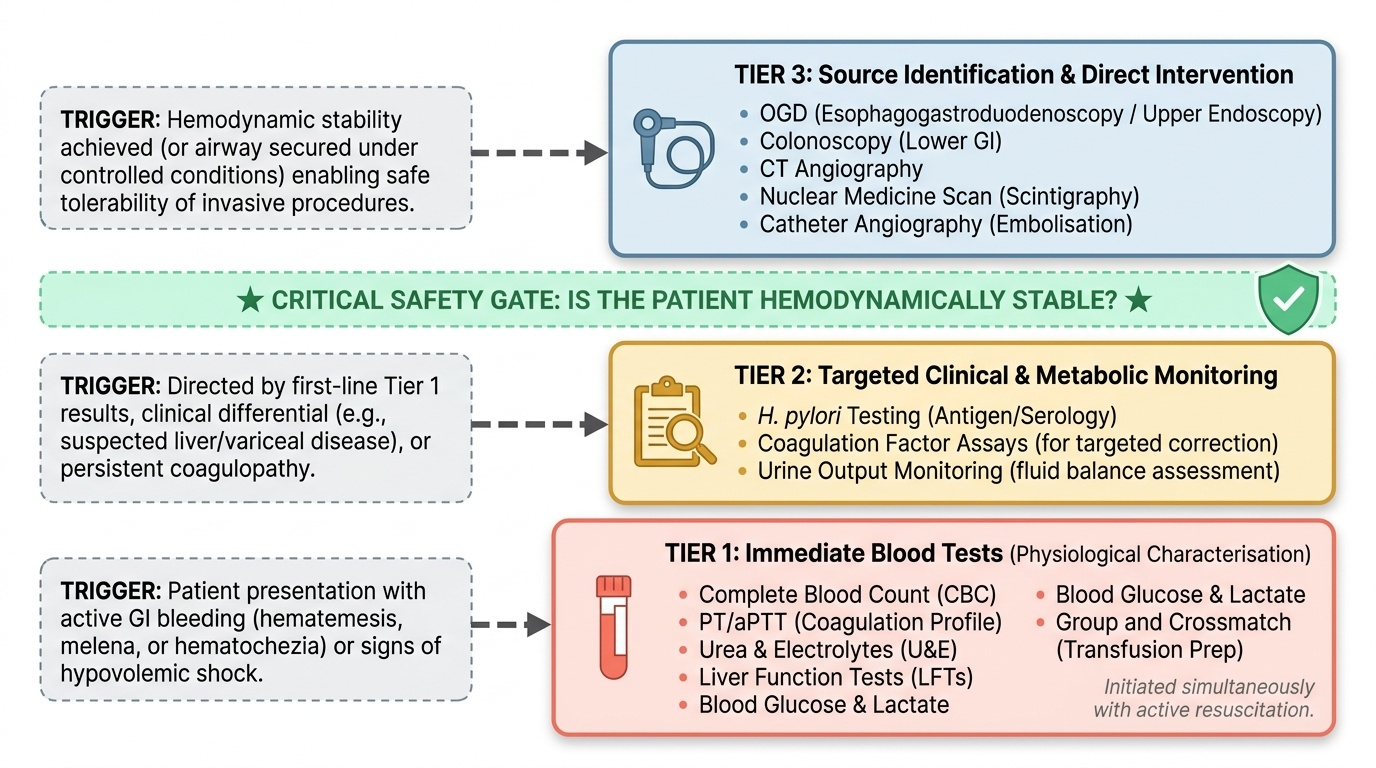
Investigations in GI bleeding serve two parallel, sequential purposes that should never be conflated. The first purpose is physiological characterisation — determining the severity of the haemorrhage, its metabolic consequences, and the patient's coagulation and haematological status. This guides immediate resuscitation decisions (transfusion thresholds, coagulopathy correction) and provides the pre-endoscopy component of risk stratification scores. The second purpose is source identification — determining precisely where in the GI tract the bleeding originates and what the responsible lesion is. This directs both the investigation approach (upper vs lower endoscopy, imaging modality) and the treatment strategy (endoscopic haemostasis technique, surgical approach, vasoactive drug choice).
Provided image
The fundamental principle of investigation sequencing in GI bleeding is that physiological stabilisation and initial laboratory investigations should proceed simultaneously, but source identification (endoscopy, imaging) should occur only after the patient is haemodynamically stable enough to safely tolerate the procedure. An upper GI endoscopy performed on a patient in active haemodynamic shock carries significant procedural mortality from cardiovascular decompensation and airway aspiration. The BSG and ESGE guidelines specify that early endoscopy (within 24 hours of presentation) for UGIB improves outcomes, but urgent endoscopy within 6–12 hours is recommended for patients with Rockall pre-endoscopy score ≥3 or Glasgow-Blatchford score ≥6 who have been haemodynamically stabilised — not in those who remain unstable.
The investigation ladder follows a rational hierarchy: first-line tests are universally applicable and immediately actionable (CBC, coagulation, metabolic panel, crossmatch), second-line tests are directed by the first-line results and clinical differential (LFTs and liver enzymes in suspected hepatic disease, H. pylori testing when PUD is probable), and third-line investigations are source-specific (endoscopy, colonoscopy, CT angiography, nuclear scanning) and proceed after clinical risk stratification.
Governing Principles of Investigation Selection in GI Bleeding
The investigation of GI bleeding is governed by a set of organising principles that, when internalised, transform a potentially chaotic multi-system investigation workup into a rational, stepwise clinical plan. These principles apply regardless of the specific clinical presentation and provide the conceptual framework that prevents both over-investigation (ordering every available test at once) and under-investigation (missing critical first-line data before proceeding to endoscopy). Understanding these governing principles — as required by the IM-skills arc step 2 — is the intellectual scaffolding on which all technical investigation knowledge depends.
Provided image
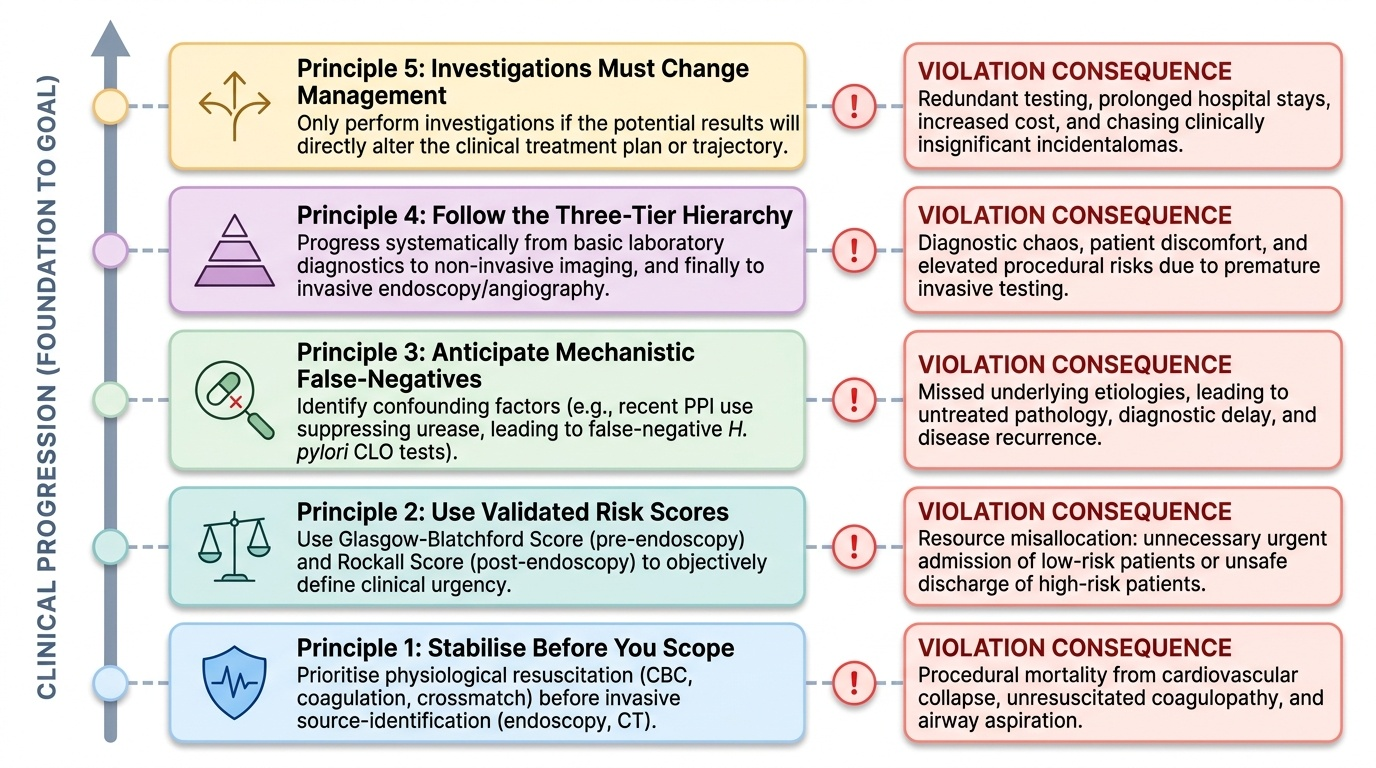
Principle 1 — Stabilise before you scope. Investigations designed to identify the bleeding source (endoscopy, CT angiography) should only be performed after the patient is haemodynamically stable or optimised for the procedure. Upper GI endoscopy in a patient with an active MAP of 50 mmHg, unresuscitated coagulopathy, and an unprotected airway carries procedural mortality from cardiovascular collapse and aspiration pneumonia. The physiological characterisation investigations (CBC, coagulation, crossmatch) must precede and inform the source-identification investigations. This is not a guideline caveat — it is a safety principle.
Principle 2 — Use validated risk scores to prioritise investigation urgency. The Glasgow-Blatchford Score stratifies patients before endoscopy; the Rockall Score stratifies them after. Using these scores correctly means that investigation urgency is evidence-based rather than impression-based. A patient with Blatchford Score 0–1 does not need immediate inpatient endoscopy — urgent outpatient endoscopy within a few days is appropriate. A patient with Blatchford Score ≥6 needs OGD within 24 hours (and within 12 hours if haemodynamically unstable after resuscitation). Risk stratification before investigation prevents both under-investigation (sending home a high-risk patient) and over-investigation (admitting a low-risk patient for unnecessary urgent endoscopy).
Principle 3 — False-negatives have mechanistic causes that must be anticipated. H. pylori CLO test false-negatives occur because of PPI-mediated urease suppression — if the patient has been on a PPI before OGD, the CLO test result cannot be trusted. This is not bad luck — it is a predictable interaction that should be anticipated and documented in the investigation plan, with a re-testing protocol specified at outset. Similarly, a CT angiogram requested in a patient who is not actively bleeding at the time of scanning will show no contrast extravasation — it is not a negative investigation if the bleeding has temporarily ceased; it means 'not actively bleeding at the moment the scan was acquired.'
Principle 4 — The investigation ladder is tiered. Not all investigations in GI bleeding are equally urgent or equally indicated in every patient. The three-tier framework (first-line universal → second-line targeted → third-line source-identification) ensures that the most actionable information is obtained first and that downstream investigation choices are guided by what the first-tier results reveal. Ordering a CT angiogram before basic bloods are available in a haemodynamically stable patient represents an inversion of the investigation hierarchy.
Principle 5 — Investigations must change management. Before ordering any investigation, ask: how will the result change my management? If the answer is 'it will not change anything I do in the next 24 hours,' re-examine whether the investigation is truly needed at this time. This is not a cost-cutting principle — it is a clinical discipline that reduces procedural risk (unnecessary endoscopy carries perforation and aspiration risk), preserves limited investigation resources, and prevents the cognitive overload of managing large volumes of minimally relevant data in an acute emergency.
Laboratory Investigations: Choice and Interpretation
The first-line laboratory investigations in GI bleeding are drawn at the time of IV cannula insertion and provide immediate actionable data for resuscitation and risk stratification. Understanding how to interpret each test — and crucially, understanding its limitations in the acute setting — prevents clinical errors.
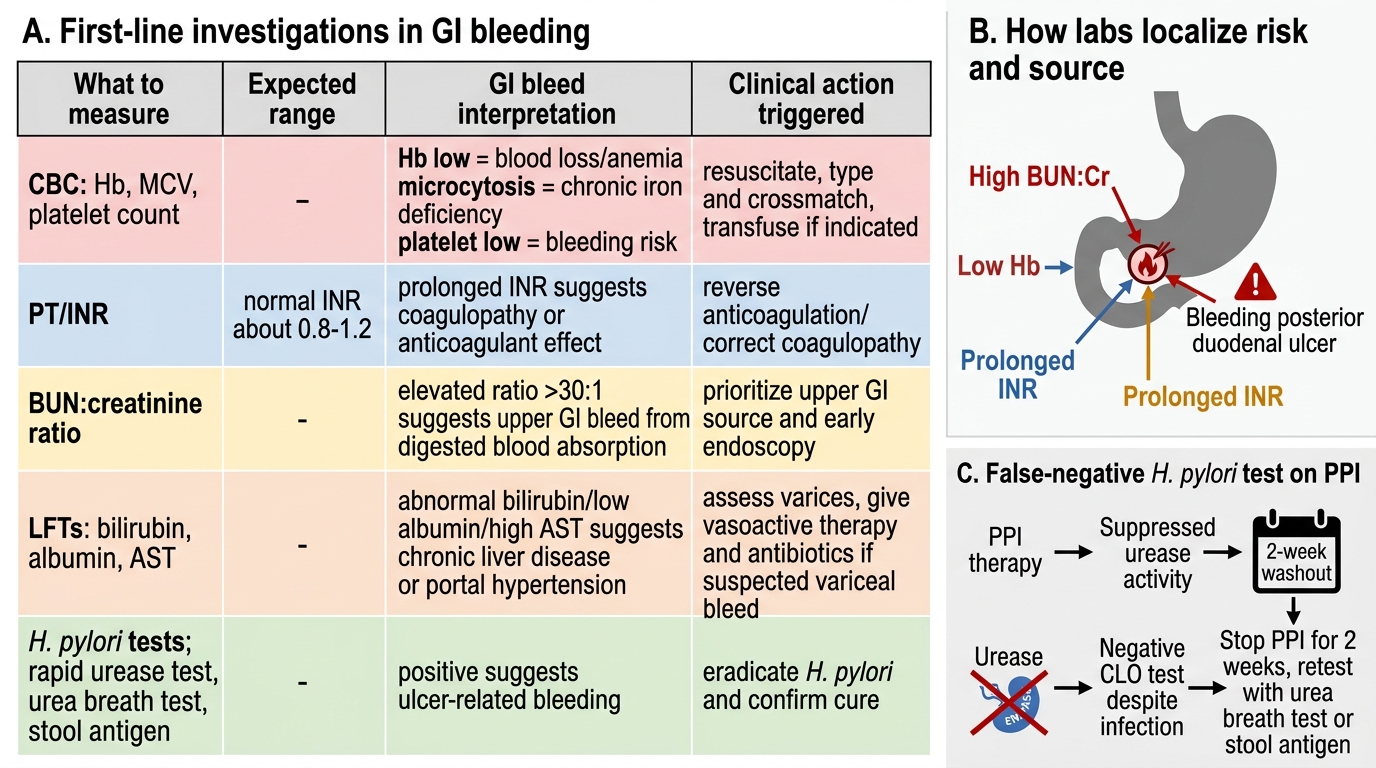
Complete blood count (CBC): The haemoglobin concentration reflects the cumulative net blood loss but is an unreliable indicator of acute haemorrhage volume in the first 6–12 hours, because haemodilution — the equilibration of plasma volume between the intravascular and interstitial compartments — takes time. A haemoglobin of 10 g/dL 2 hours after acute massive haemorrhage may reflect pre-existing anaemia or early haemoconcentration, not the actual current haemoglobin after equilibration. Serial measurements (at presentation, 4 hours, and 12–24 hours) are more informative than a single acute measurement. A mean corpuscular volume (MCV) below normal (microcytic anaemia) in the presence of rectal bleeding strongly suggests chronic iron-deficiency anaemia from occult lower GI bleeding — potentially from a colorectal carcinoma, polyp, or angiodysplasia. The platelet count is important: thrombocytopaenia (<50 × 10⁹/L) in active bleeding warrants platelet transfusion. In a patient with chronic liver disease and splenomegaly, splenic sequestration commonly reduces platelets — values of 80–120 × 10⁹/L are expected and should not cause alarm, but values below 50 × 10⁹/L in the context of active haemorrhage require correction.
Prothrombin time (PT), INR, and activated partial thromboplastin time (aPTT): These coagulation tests are critical in two contexts: patients on anticoagulant therapy (warfarin, rivaroxaban, apixaban, dabigatran — note that DOACs do NOT affect PT/INR or aPTT in the standard assay and specific factor assays or drug levels are needed); and patients with suspected liver disease (hepatic synthetic failure produces prolonged PT/INR). An INR >1.5 in the context of active GI bleeding is an indication for fresh frozen plasma (4 units FFP alongside every 6 units of packed red cells in massive transfusion) or specific factor replacement. Vitamin K (IV phytomenadione 10 mg over 30 minutes) should be given if the INR is elevated and the cause is vitamin K deficiency or warfarin anticoagulation.
Urea and electrolytes (U&E), BUN, creatinine: The BUN:creatinine ratio is both a diagnostic marker (>20:1 suggests upper GI source due to protein digestion) and a monitor of kidney function (rising creatinine indicates AKI from renal hypoperfusion — a complication requiring adjustment of fluid and drug management). Urea and creatinine together track the trajectory of renal function over the admission.
Liver function tests (LFTs): In any patient with suspected liver disease or variceal bleeding, LFTs are mandatory and provide diagnostic and prognostic information. Elevated bilirubin and low albumin together with coagulopathy suggest decompensated liver disease — a Child-Pugh score C patient with variceal bleeding has a 30-day mortality exceeding 30%. Elevated AST and ALT (hepatocellular pattern) in a patient with alcohol use disorder suggests alcoholic hepatitis or chronic hepatitis B/C. Elevated alkaline phosphatase and GGT with bilirubin suggests cholestatic liver disease.
H. pylori testing: In any patient with UGIB in whom peptic ulcer disease is confirmed or likely, H. pylori testing is mandatory — because eradication therapy is both curative (eliminating the causative organism) and reduces the long-term rebleeding risk by 80–90%. Testing methods in acute GI bleeding: (a) Antral biopsy at OGD for rapid urease test (CLO test) or histology — the most sensitive and specific, but false-negatives occur if the patient is already on a PPI (PPIs suppress urease activity, giving false-negative CLO test — the PPI should ideally be stopped 2 weeks before the biopsy); (b) Urea breath test — the gold standard non-invasive test, but cannot be done in the acute setting; (c) Stool antigen test — convenient, moderately sensitive, valid in the acute setting; (d) H. pylori serology — detects IgG antibodies but cannot distinguish active from past infection and is now considered unreliable for confirmation of active infection.
Faecal occult blood (FOB) testing: While not an acute investigation, FOB testing is the investigation for screening asymptomatic iron-deficiency anaemia where the source is unknown. A positive FOB test mandates lower GI endoscopy to exclude colorectal carcinoma. The immunochemical FOB test (iFOB or FIT test) has higher specificity than the older guaiac-based test and does not require dietary restrictions.
First-Line Investigation Interpretation in GI Bleeding
SELF-CHECK
A 64-year-old man with known peptic ulcer disease undergoes upper GI endoscopy which reveals a posterior duodenal ulcer. The CLO test (rapid urease test) for H. pylori returns negative. He was started on IV omeprazole 3 days ago before endoscopy. What is the most likely explanation for the negative result, and what should you do?
A. The negative CLO test confirms H. pylori is not present; no further testing needed
B. PPI therapy suppresses urease activity, causing a false-negative CLO test; re-test after 2 weeks off PPI using urea breath test or stool antigen test
C. The CLO test is unreliable in patients over 60 and should not be used
D. H. pylori serology should be checked — it is unaffected by PPI therapy
Reveal Answer
Answer: B. PPI therapy suppresses urease activity, causing a false-negative CLO test; re-test after 2 weeks off PPI using urea breath test or stool antigen test
PPI therapy (and to a lesser extent bismuth compounds and antibiotics) suppresses urease activity, causing false-negative results on the CLO (rapid urease) test and the urea breath test. After a negative CLO test in a PPI-treated patient, re-testing after a 2-week PPI washout using the urea breath test (gold standard) or stool antigen test is the correct approach. Serology (IgG) cannot distinguish active from past infection and remains positive even after successful eradication — making it unsuitable for confirming active infection or confirming eradication.