Page 1 of 19
IM16.{1-3,6,15} | Diarrheal Disorder Foundations — SDL Guide
Learning Objectives
- Define diarrhoea and dysentery and distinguish them on clinical grounds
- Classify diarrhoeal disorders by duration (acute, persistent, chronic) and enumerate the commonest causes in each category, with attention to India-relevant pathogens
- Describe the four pathophysiological mechanisms of diarrhoea (secretory, osmotic, inflammatory, malabsorptive) and their clinical signatures
- Explain the acute systemic consequences of diarrhoea including dehydration assessment using the WHO 3-plan framework and composition of WHO ORS
- Describe the chronic effects of diarrhoea including malabsorption, fat-soluble vitamin deficiencies, hypoalbuminaemia, and anaemia
- Distinguish Crohn's disease from ulcerative colitis on the basis of clinical features, distribution, histopathology, and management principles
INSTRUCTIONS
Diarrhoeal disorders span the full spectrum of acute life-threatening dehydration to chronic debilitating malabsorption. This foundational SDL builds the mechanistic and classificatory scaffold — four pathophysiological mechanisms, duration-based classification, the WHO dehydration framework, and the Crohn's vs UC distinction — that underpins all clinical reasoning in subsequent modules. Work through the scenarios actively: map each case to a mechanism before looking at the analysis.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 43 — Diarrhoea and Constipation (textbook)
- API Textbook of Medicine, 10th ed., Ch. 7 — Gastroenterology (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 24 — Alimentary Tract (textbook)
- WHO Guidelines for the Control of Cholera, 2017 (guideline)
- WHO ORS Formulation (Reduced Osmolarity), WHO/UNICEF 2002 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man is rushed into the casualty department at a district hospital in West Bengal during July. He arrived by auto-rickshaw, barely able to sit upright. His wife explains he started passing watery stools at midnight — colourless, odourless, and appearing like rice-water — and has now passed more than a litre in three hours. His eyes are sunken, his skin tents when pinched, and his radial pulse is barely palpable. He does not complain of abdominal pain or fever. Within 200 metres, four other households have reported similar illness in the last 24 hours. Now, across the corridor, a 28-year-old woman is brought in with bloody, mucoid stools, lower abdominal cramps, tenesmus, and fever of 38.8°C. She is alert and her radial pulse is strong. Both patients have 'diarrhoea' — but everything else about their presentations is different. Understanding why begins with the mechanisms, consequences, and classification system that separates these two patients the moment they walk through the door.
WHY THIS MATTERS
Diarrhoeal disease remains one of the top five causes of mortality and morbidity in India, particularly among children under five and in adults during monsoon and post-flood seasons. For a final-year MBBS student, diarrhoeal disorders are not merely examination material — they are the single most common acute presentation you will encounter in government district hospitals, primary health centres, and emergency departments across the country. The competencies IM16.1–IM16.15 span the breadth of diarrhoeal disease from basic aetiology and pathophysiology through clinical assessment, diagnostic testing, and treatment — demanding a coherent, mechanistic understanding, not a list of diseases. This foundational SDL establishes the conceptual scaffold on which all subsequent SDL modules in this cluster build: without a clear mental model of mechanisms, duration-based classification, and the acute versus chronic consequences of diarrhoea, you cannot reason through a diagnostic workup, counsel a patient about oral rehydration, or recognise when a patient with chronic loose stools has inflammatory bowel disease rather than irritable bowel syndrome.
RECALL
Before proceeding, recall the physiology of the small and large intestine. Each day, approximately 9 litres of fluid enter the small intestine (2 L ingested + 7 L from salivary, gastric, pancreatic, biliary, and intestinal secretions). Of this, the small intestine absorbs approximately 7–8 litres and the colon absorbs the remaining 1–1.5 litres, leaving only about 100–200 mL in the final stool. Any disruption that increases fluid entering the colon beyond its absorptive capacity (~3–4 L/day), decreases the colon's absorptive capacity, or drives net secretion will result in diarrhoea. Recall also the anatomy of electrolyte transport: sodium is absorbed by coupled co-transporters (sodium-glucose, sodium-amino acid) and through sodium channels, while chloride can be secreted via CFTR channels in intestinal epithelial cells. Cyclic AMP and cyclic GMP activate these channels — a mechanism exploited by cholera toxin. From your Pathology training, recall that villous architecture of the small intestine (villus-to-crypt ratio 3–5:1) is critical for absorptive surface area, and that any process reducing this ratio (villous atrophy in coeliac disease, tropical sprue) will directly impair absorption.
Classification and Aetiology of Diarrhoeal Disorders
Diarrhoea is defined as the passage of three or more loose or liquid stools per day, or a frequency greater than is normal for the individual, representing a significant change from baseline. This quantitative definition is important because frequency alone can be misleading — some individuals pass loose stools twice daily as their baseline without any disease. The WHO practical definition for clinical settings is stool weight exceeding 200 grams per day or stool water content exceeding 80% of stool mass. For field settings and epidemiological surveys, the three-loose-stools threshold is retained. Dysentery — a term often loosely applied — is specifically defined as diarrhoea with visible blood and/or mucus in the stool, which signals mucosal invasion or inflammation and is NOT synonymous with severe diarrhoea; a patient with profuse watery cholera has severe diarrhoea but NOT dysentery.
The duration-based classification of diarrhoea creates three clinically meaningful groups:
- Acute diarrhoea: <2 weeks duration. The overwhelming majority of infectious diarrhoeal episodes fall here. Most self-resolve within 3–5 days. Infectious causes dominate in this category.
- Persistent diarrhoea: 2–4 weeks duration. This intermediate category (codified by WHO/UNICEF for child health programmes) represents cases that have escaped self-resolution and raises concern for parasitic infection, post-infectious disruption of the mucosa, or early chronic disease.
- Chronic diarrhoea: >4 weeks duration. Non-infectious causes predominate, including inflammatory bowel disease, malabsorption syndromes, functional disorders, and secretory tumours. The diagnostic approach shifts substantially from acute diarrhoea.
The aetiology framework organises causes by mechanism and acuity:
Infectious causes (predominate in acute/persistent diarrhoea):
- Viral: Rotavirus (commonest cause of acute diarrhoeal mortality in children under 5 globally), norovirus (explosive outbreaks in closed settings: hospitals, cruise ships, schools), adenovirus 40/41, astrovirus. Mechanism: viral enterocyte damage + osmotic + secretory components.
- Bacterial: Vibrio cholerae (rice-water stools, profuse secretory diarrhoea, dehydration without fever — the classic epidemic form); Enterotoxigenic Escherichia coli (ETEC) (traveller's diarrhoea, heat-labile and heat-stable toxins); Enteroinvasive E. coli (EIEC) / Shigella spp. (dysentery: bloody mucoid stools, fever, tenesmus); Campylobacter jejuni (commonest bacterial cause of diarrhoea in high-income countries, less appreciated in India; bloody stools, preceded by fever); Salmonella typhi (enteric fever — diarrhoea usually late in the course, 'pea-soup' stools); non-typhoidal Salmonella (food-borne, gastroenteritis); Clostridioides difficile (post-antibiotic, hospital-acquired, pseudomembranous colitis).
- Parasitic: Entamoeba histolytica (amoebiasis — flask-shaped ulcers in the colon, bloody mucoid diarrhoea; risk of amoebic liver abscess if invasive); Giardia intestinalis (lamblia) (malabsorption, foul-smelling floating stools, no blood, small intestine involvement); Cryptosporidium parvum (self-limiting in immunocompetent, severe and life-threatening in HIV — watery diarrhoea).
Non-infectious causes (predominate in chronic diarrhoea):
- Inflammatory bowel disease: Crohn's disease and ulcerative colitis (discussed under IM16.15).
- Malabsorption syndromes: coeliac disease (gluten-sensitive enteropathy; villous atrophy; anti-tTG antibodies), tropical sprue (malabsorption in tropical regions, responds to folate + tetracycline), lactase deficiency, post-infectious malabsorption.
- Secretory causes: carcinoid tumours (serotonin), VIPoma (vasoactive intestinal peptide), Zollinger-Ellison syndrome (excess acid damaging small bowel mucosa).
- Osmotic causes: laxative abuse, sorbitol ingestion, lactose intolerance (stool osmotic gap elevated).
- Functional: irritable bowel syndrome (IBS) — altered bowel habit without structural or biochemical cause, Rome IV criteria required.
- Drugs: metformin, broad-spectrum antibiotics, PPIs (rare), magnesium-containing antacids, colchicine.
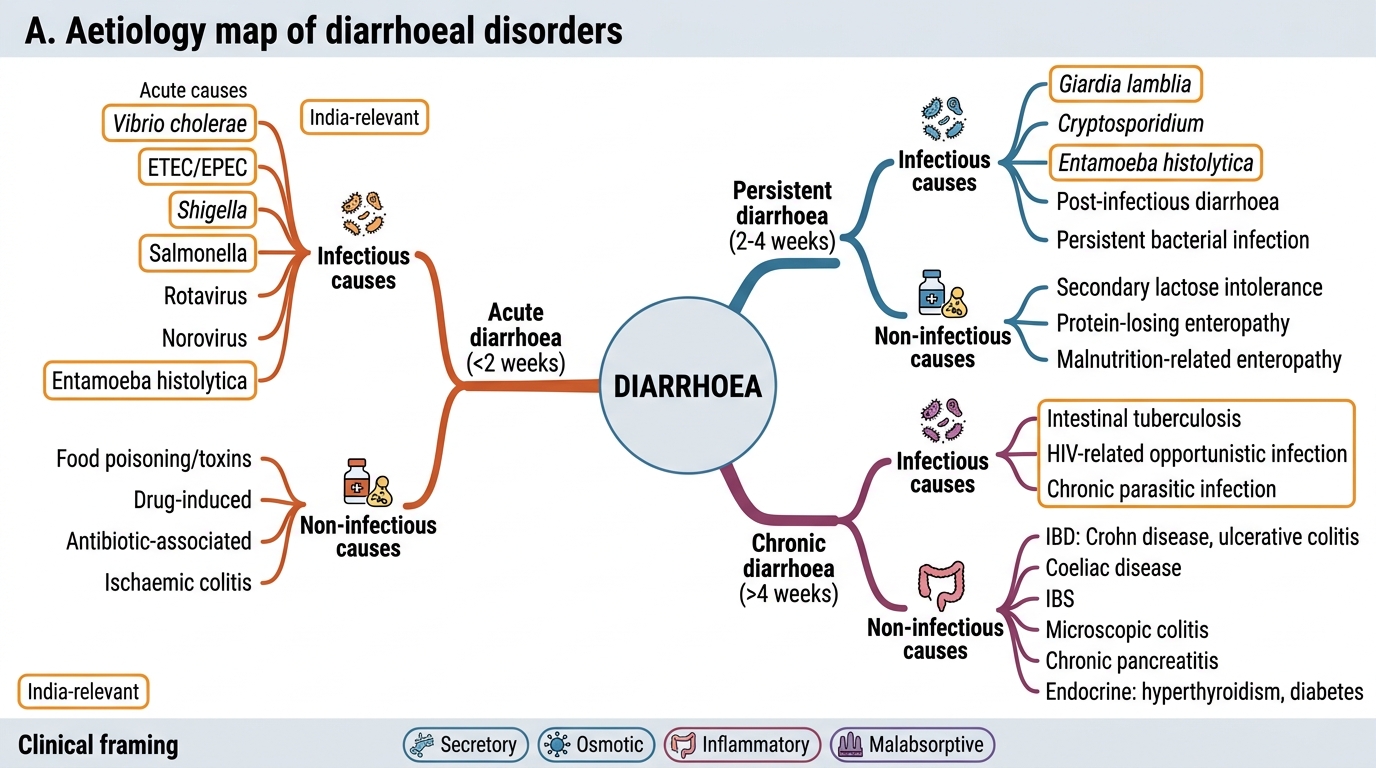
Aetiology Map of Diarrhoeal Disorders
Pathophysiology: Four Mechanisms and Their Clinical Signatures
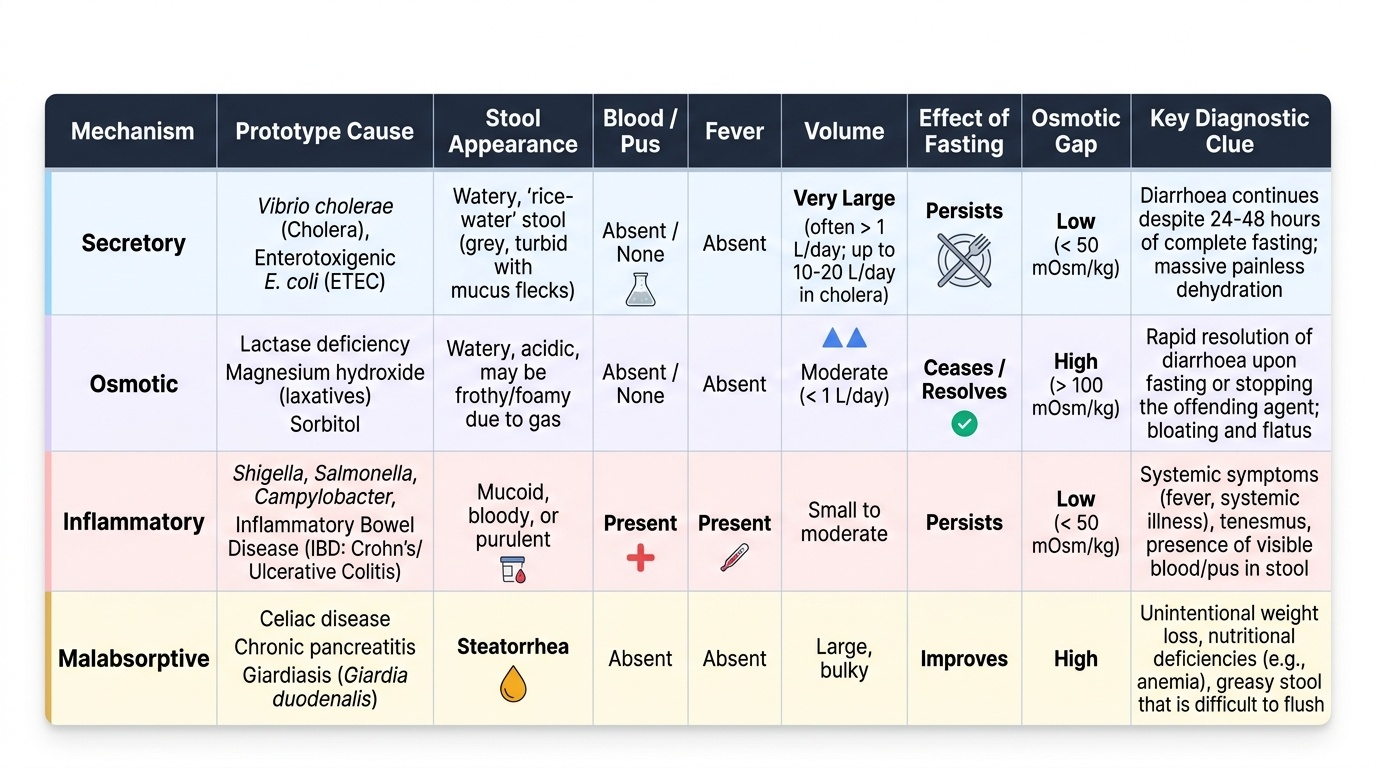
Every case of diarrhoea, regardless of the specific pathogen or disease, operates through one or more of four fundamental pathophysiological mechanisms. Recognising which mechanism(s) underlie a given presentation is the key to generating the correct differential diagnosis and selecting rational investigations and treatment. These four mechanisms are not merely academic classifications — they generate clinically distinguishable stool types, symptom patterns, and dehydration profiles that can be partially read at the bedside before a single investigation is ordered.
Provided image
1. Secretory diarrhoea occurs when intestinal epithelial cells are driven to secrete fluid and electrolytes into the intestinal lumen in excess of their absorptive capacity, typically via cAMP/cGMP-mediated activation of the cystic fibrosis transmembrane conductance regulator (CFTR) chloride channel. The archetype is cholera: V. cholerae produces cholera toxin (CT), which ADP-ribosylates the Gs alpha subunit of adenylate cyclase, constitutively activating it and producing massive intracellular cAMP. This drives chloride secretion into the lumen, and sodium and water follow osmotically. The result is a massive, painless, watery diarrhoea with stools that resemble rice-water (grey, slightly turbid with mucus flecks from shed epithelial cells). Key features of secretory diarrhoea: (a) large volume stools (may exceed 10–20 litres per day in severe cholera), (b) no blood or pus (no mucosal invasion), (c) no fever typically (toxin-mediated, no inflammation), (d) stool osmotic gap is low (stool electrolytes account for the osmolality), and (e) persists with fasting — a critically important feature that separates it from osmotic diarrhoea. ETEC uses a similar mechanism (heat-labile toxin activates cAMP; heat-stable toxin activates cGMP via guanylate cyclase).
2. Osmotic diarrhoea occurs when a non-absorbable, osmotically active solute is present in the intestinal lumen, retaining water by osmosis and overwhelming the colon's absorptive capacity. Examples include lactase deficiency (undigested lactose fermented to short-chain fatty acids and hydrogen gas, causing bloating and diarrhoea), magnesium hydroxide antacid overdose, sorbitol in sugar-free foods, and lactulose administration. Key features: (a) ceases with fasting (the solute is no longer ingested), (b) stool osmotic gap is high: calculated as [serum osmolality] − 2×([stool Na] + [stool K]), normally <50 mOsm/kg; a gap >125 mOsm/kg indicates osmotic diarrhoea, (c) moderate volumes, (d) may have bloating and flatulence from fermentation.
3. Inflammatory (exudative) diarrhoea results from invasion or ulceration of the intestinal mucosa by pathogens or inflammatory disease, causing loss of mucosal barrier integrity and exudation of blood, pus (neutrophil-rich), and mucus into the stool. This is dysentery in its clinical and pathophysiological sense. The pathogens involved include invasive bacteria (Shigella, EIEC, Campylobacter, Salmonella, C. difficile producing toxins A and B) and invasive parasites (E. histolytica producing flask-shaped ulcers in the caecum and ascending colon). In non-infectious inflammatory diarrhoea, Crohn's disease and ulcerative colitis (IBD) cause similar mucosal destruction via immune-mediated inflammation. Features: (a) blood and/or mucus in stool — the defining feature, (b) fever (systemic inflammatory response), (c) abdominal pain and tenesmus (colonic involvement), (d) moderate volume (limited by colon's maximum secretion from the damaged area), (e) faecal leucocytes (white cells) on microscopy — a useful bedside marker of mucosal invasion.
4. Malabsorptive diarrhoea results from failure to absorb nutrients, fat, carbohydrates, or vitamins in the small intestine, leading to osmotically active, incompletely absorbed substances in the lumen causing loose, bulky, floating, pale, foul-smelling steatorrhoeic stools. Steatorrhoea occurs when faecal fat exceeds 7 grams per day (normal <7 g/day on a 100 g fat diet). This mechanism underpins coeliac disease (gluten-induced villous atrophy → loss of absorptive surface), tropical sprue (mucosal damage of unclear aetiology in tropical regions → impaired fat and B12/folate absorption), chronic pancreatitis (exocrine insufficiency → inadequate lipase), giardiasis (attachment of trophozoites to proximal small intestinal mucosa → impaired absorption without mucosal invasion), and short bowel syndrome. Features: (a) fatty, pale, floating, foul-smelling stools, (b) no blood, (c) weight loss and nutritional deficiencies, (d) chronic course.
Osmotic gap calculation for bedside use: collect spot stool sample → measure Na and K in stool → osmotic gap = measured stool osmolality (or use serum osmolality as a surrogate) − 2 × (stool Na + stool K). If the gap is >125: osmotic. If <50: secretory. Gaps in between (50–125) may indicate a mixed mechanism.
SELF-CHECK
A 45-year-old man presents with six watery stools per day for three days. The stools are large-volume, grey, and odourless. He has no fever, no blood in stool, and no abdominal pain. He recalls eating at a roadside stall during a festival six days ago. Stool microscopy shows no leucocytes. His radial pulse is 120/min and skin turgor is reduced. Which mechanism BEST explains his diarrhoea?
A. Osmotic diarrhoea due to lactase deficiency
B. Inflammatory diarrhoea due to Shigella dysentery
C. Secretory diarrhoea due to Vibrio cholerae
D. Malabsorptive diarrhoea due to giardiasis
Reveal Answer
Answer: C. Secretory diarrhoea due to Vibrio cholerae
The classic features here are large-volume watery (rice-water) stools, absence of fever, absence of blood, absence of faecal leucocytes, and context of a community meal — this is the prototypic secretory diarrhoea of cholera (Vibrio cholerae). Cholera toxin constitutively activates adenylate cyclase via ADP-ribosylation of Gs-alpha, driving massive chloride secretion through CFTR. The resulting diarrhoea is large-volume, painless, and without systemic inflammation. Osmotic diarrhoea (lactase deficiency) would be smaller volume and would stop with fasting. Shigella dysentery would have fever, blood, mucus, and leucocytes. Giardiasis causes malabsorptive, fatty stools without this severity of dehydration acutely.
Acute Systemic Consequences: Fluid Balance and Dehydration
The systemic consequences of acute diarrhoea derive predominantly from the loss of isotonic fluid from the gastrointestinal tract, producing a spectrum from mild dehydration to hypovolaemic shock, metabolic acidosis, and end-organ failure. In secretory diarrhoea (especially cholera), fluid losses can exceed 1 litre per hour, making this the most medically urgent presentation in diarrhoeal disease. The fluid lost in diarrhoea approximates an iso-osmolar, isotonic solution similar to plasma in composition (Na ~130 mEq/L, K ~10 mEq/L, HCO₃ ~40 mEq/L, Cl ~90 mEq/L) — meaning the primary fluid compartment lost is the extracellular fluid (ECF), and the resulting dehydration is predominantly isotonic dehydration. As ECF and plasma volume shrink, the classic signs of dehydration appear in a progressive sequence.
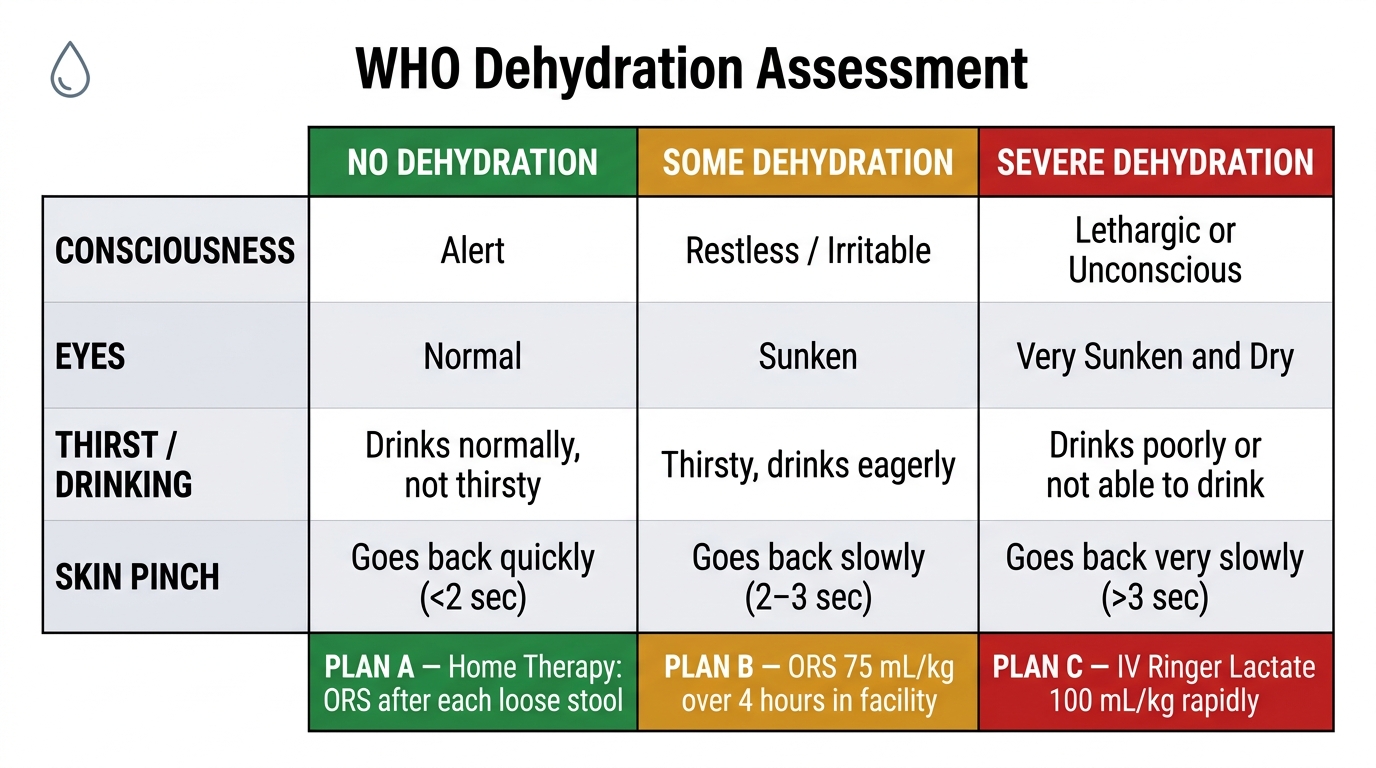
The WHO 3-plan dehydration assessment is the internationally standardised clinical tool for categorising severity and guiding treatment intensity:
Plan A — No dehydration (mild, <5% body weight fluid loss): Patient is alert, has normal skin turgor, normal eyes, drinks normally. Treatment: oral rehydration therapy (ORT) at home, increased fluids, continue feeding.
Plan B — Some dehydration (moderate, 5–9% body weight fluid loss): Two or more of: restless/irritable, sunken eyes, drinks eagerly/thirsty, skin pinch goes back slowly (>1 second but <2 seconds). Treatment: supervised ORS therapy in a health facility — 75 mL/kg of WHO low-osmolarity ORS over 4 hours.
Plan C — Severe dehydration (≥10% body weight fluid loss): Two or more of: lethargic/unconscious, sunken eyes, cannot drink/drinks poorly, skin pinch goes back very slowly (>2 seconds). Treatment: intravenous Ringer's Lactate (or normal saline if RL unavailable) — 100 mL/kg infused rapidly (30 mL/kg in 30 minutes for adults, then 70 mL/kg over next 2.5 hours).
WHO low-osmolarity ORS (2002 formulation) — the correct composition to memorise:
- Total osmolarity: 245 mOsm/L (reduced from the original 311 mOsm/L)
- Sodium: 75 mEq/L
- Glucose: 75 mmol/L (equimolar with Na — exploits sodium-glucose co-transporter SGLT1 which remains functional even when toxin-induced secretion is operating)
- Potassium: 20 mEq/L
- Chloride: 65 mEq/L
- Trisodium citrate (buffer): 10 mmol/L
The physiological basis for ORS is the sodium-glucose coupled transport (SGLT1 mechanism): glucose and sodium are co-transported into enterocytes by SGLT1 in a 1:1 ratio; water follows osmotically. Crucially, this transporter is not blocked by cholera toxin (which acts on CFTR channels, not SGLT1) — this is why ORS works even in severe secretory diarrhoea. The reduced-osmolarity ORS (245 vs 311) reduces the stool output by approximately 20% and reduces the need for unscheduled IV therapy.
Metabolic consequences of severe acute diarrhoea include:
- Metabolic acidosis: loss of bicarbonate (HCO₃ lost in stool is substantial), lactic acidosis from poor tissue perfusion
- Hypokalaemia: potassium loss in stool (stool K can be 30–80 mEq/L in secretory diarrhoea); manifests as muscle weakness, ileus, cardiac arrhythmias
- Hyponatraemia: if patient replaces fluid losses with plain water alone, diluting plasma sodium
- Uraemia and AKI: pre-renal AKI from severe hypovolaemia; renal tubular damage in prolonged shock
- Hypovolaemic shock: systolic BP <90 mmHg, oliguria/anuria, mental obtundation — life-threatening emergency
WHO Dehydration Assessment Table — Clinical Signs and Treatment Plans (A, B, C)