Page 9 of 21
IM17.6-9 | Headache Diagnostic Testing and Lumbar Puncture — SDL Guide
Learning Objectives
- Choose and justify the appropriate diagnostic investigation (CT, MRI, MRV, LP) for a headache presentation based on clinical features and red flags
- Enumerate the indications and absolute contraindications for lumbar puncture in headache management
- Describe the governing anatomical principles of LP and demonstrate correct technique including positioning, landmark identification, needle insertion, pressure measurement, and CSF collection
- Describe normal CSF reference values and interpret the characteristic CSF profiles of bacterial meningitis, viral meningitis, tuberculous meningitis, and subarachnoid haemorrhage
- Distinguish a traumatic tap from true SAH using the blood-clearance rule across collection tubes and xanthochromia on spectrophotometry
INSTRUCTIONS
This module covers diagnostic test selection, LP technique, and CSF interpretation for headache. The CSF pattern table is a high-yield memorisation target. LP technique will be assessed on a mannequin in OSCE. Study the four CSF archetypes until you can generate the full pattern from the diagnosis name and vice versa.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 17 — Headache and Appendix on LP and CSF Analysis (textbook)
- API Textbook of Medicine, 10th ed. — Lumbar Puncture and CSF Analysis (textbook)
- NICE Clinical Guideline CG176: Headache in Adults (guideline)
- British Infection Association Consensus on Tuberculous Meningitis Diagnosis, 2009 (guideline)
- IDSA Clinical Practice Guidelines for Cryptococcal Disease, 2010 (updated 2023) (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Arjun, a 29-year-old medical resident, brings his 52-year-old patient to you: 'Sir, she came in with a thunderclap headache three hours ago. CT brain is normal. The attendant is asking why we're asking for a lumbar puncture when the CT is already normal.' Meanwhile, in the next bed, a 68-year-old man with a two-month history of subacute progressive headache and a CD4 count of 85 cells/µL has a CT showing no obvious space-occupying lesion. His team is debating whether LP is safe and what to look for in the CSF. And in the casualty, a 35-year-old woman with fever, headache, and neck stiffness has a blood culture drawn but her senior is hesitant about LP because 'what if she herniates?' Three different headache scenarios, three different clinical rationales for lumbar puncture, three different CSF profiles you must be able to predict and interpret. By the end of this module you will know when to image, when to puncture, how to puncture safely, and how to read a CSF report as fluently as you read a haemogram.
WHY THIS MATTERS
Diagnostic testing in headache is a high-stakes clinical skill. The wrong decision — imaging when LP is needed, or performing LP without imaging in raised ICP — can result in avoidable blindness, herniation, or missed diagnosis. The NMC competencies IM17.6 (choose and interpret diagnostic testing including imaging based on clinical diagnosis), IM17.7 (enumerate LP indications and describe CSF findings in different types of meningitis), IM17.8 (demonstrate LP technique on a mannequin), and IM17.9 (interpret CSF analysis reports) collectively address a skill set that is tested at both the knowledge and demonstration level. In Indian practice, the burden of tuberculous meningitis makes CSF interpretation — specifically distinguishing TBM from bacterial and viral meningitis — a particularly critical competency.
RECALL
Recall from your headache foundations module: thunderclap headache mandates CT then LP ≥12 hours — CT sensitivity for SAH is ~98% at 6 hours but falls to ~50% by 1 week. From your neuroanatomy: the lumbar cistern (L2–S2) contains the cauda equina and is the site of LP because the spinal cord ends at L1–L2 in adults — inserting below L2 avoids cord injury. The standard LP landmark is the iliac crest level = L4 (or L3–L4 or L4–L5 interspaces). From pathology: blood in the CSF degrades — oxyhaemoglobin (pink/yellow) appears within hours; xanthochromia (yellow-brown) from bilirubin forms within 2–4 hours and persists up to 2 weeks. From physiology: normal CSF is crystal-clear (water-clear), with opening pressure 10–20 cmH₂O in the lateral decubitus position, protein 15–45 mg/dL, glucose 50–80 mg/dL (CSF:serum ratio >0.6), WBC 0–5 lymphocytes/mm³, no RBCs, no organisms.
When to Image: Choosing Diagnostic Tests for Headache
The first diagnostic decision in a headache presentation is whether investigation is required at all. In a typical primary headache — migraine, tension-type, cluster — with no red flags and a normal neurological examination, no investigation is necessary because the diagnosis is clinical. The appropriate indication for imaging or LP is guided by the SNNOOP10 red-flag screen and specific clinical patterns. Understanding which modality to choose, and in what sequence, is the clinical indication skill that IM17.6 tests at the SH level.
The choice between CT and MRI depends on the clinical question being asked. Non-contrast CT head is the first-line imaging modality for acute headache with red flags because it is fast (minutes versus 30–45 minutes for MRI), widely available in emergency departments, highly sensitive for acute blood (haemorrhage appears hyperdense on non-contrast CT within minutes of onset), and adequate for detecting most acute structural emergencies — herniation, large SOL, midline shift, obstructive hydrocephalus. It is the appropriate first test for: thunderclap headache (SAH protocol), suspected subarachnoid or intracerebral haemorrhage, trauma, and any situation requiring rapid decision-making under time pressure. However, CT has important limitations that must be understood: it is insensitive for posterior fossa pathology (bone artefact on standard sequences), isodense subacute subdural haematoma (may appear isodense to brain at 1–3 weeks), early cerebral infarction (<6 hours), early herpes encephalitis, leptomeningeal disease, and small pituitary lesions. For these indications, MRI is superior.
MRI brain (with gadolinium contrast where a mass lesion, infection, or leptomeningeal pathology is suspected) is indicated for: posterior fossa structures (brainstem, cerebellum — CT bone artefact is avoided), white matter disease, cortical venous thrombosis (requires MR venography), encephalitis (herpes simplex — characteristic temporal and insular lobe signal change on FLAIR/DWI), pituitary lesions, leptomeningeal carcinomatosis (FLAIR and post-gadolinium sequences), and subacute or chronic lesions where CT is negative but clinical suspicion persists. MRI with FLAIR sequences is more sensitive than CT for subarachnoid blood that is older than a few hours — the FLAIR signal in the sulci from SAH may persist for 48–72 hours.
CT angiography (CTA) is indicated when an intracranial aneurysm is suspected — after confirmation of SAH on CT or LP — to identify aneurysm location and anatomy before neurosurgical or endovascular intervention. MR angiography (MRA) is an alternative without radiation but less sensitive for small aneurysms (<3 mm). MR venography (MRV) is specifically required when cerebral venous thrombosis is suspected: progressive headache with papilloedema in a young woman on OCP or in the puerperium; headache with venous infarction pattern on MRI; raised ICP without structural cause.
The imaging algorithm for headache in practice: (1) Thunderclap headache → non-contrast CT head first; (2) Progressive headache with raised ICP features or focal deficit → MRI with contrast; (3) Suspected CVT → MRI + MRV; (4) Fever + meningism → CT first to exclude raised ICP before LP; (5) Typical primary headache, no red flags → no imaging required.
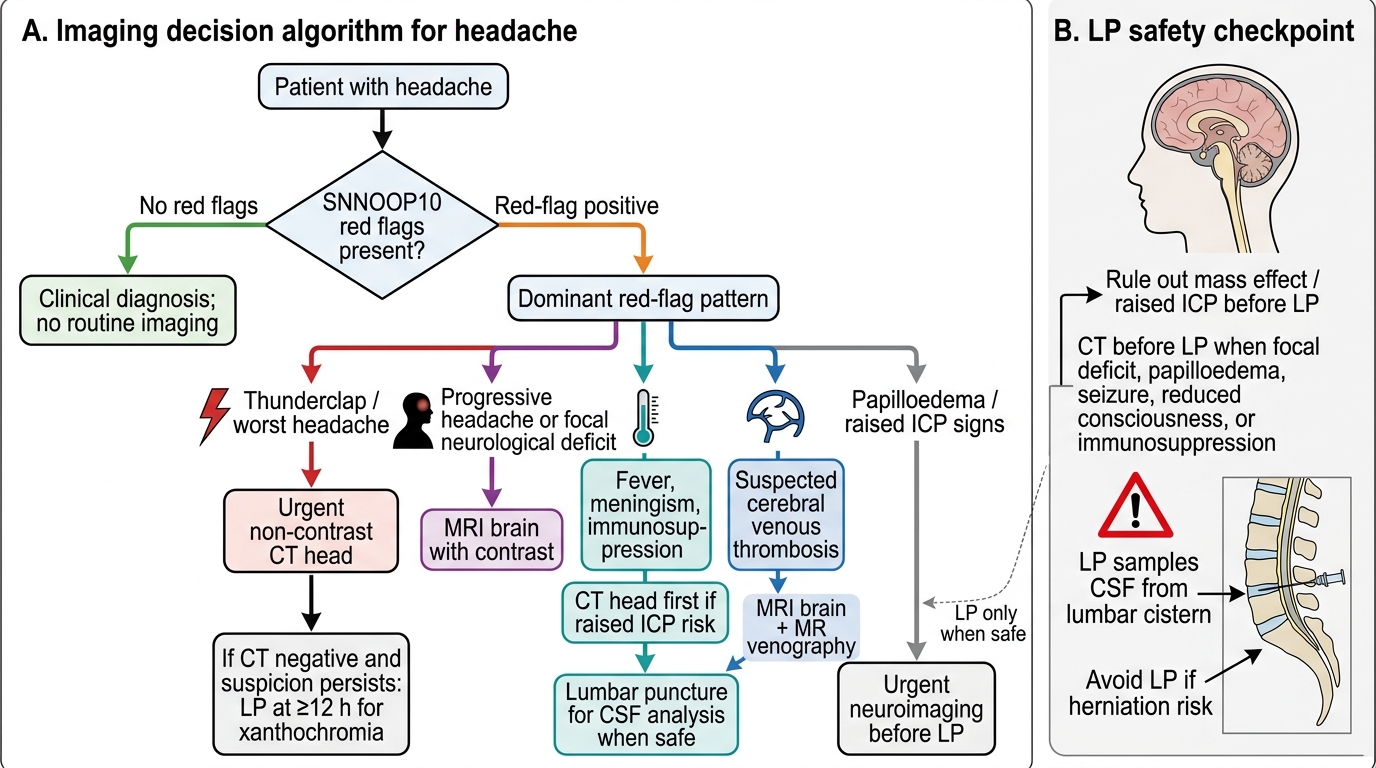
Imaging Algorithm for Headache Red Flags
Lumbar Puncture: Indications and Contraindications
Lumbar puncture (LP) is the direct sampling of cerebrospinal fluid from the lumbar cistern by needle insertion through the skin and into the subarachnoid space between L3–L4 or L4–L5. It is one of the most diagnostically powerful procedures in neurology and general medicine — the CSF analysis provides information that is unobtainable by any other means, including blood tests, CT, or MRI. Competence in its indication, technique, and interpretation is a required skill for every final-year MBBS student and junior doctor. Equally important is knowing when NOT to perform LP — because an LP done in the presence of significantly raised intracranial pressure can cause fatal brainstem herniation, making the contraindications as safety-critical as the indications. Understanding the precise indications and contraindications for LP is the essential first step in the IM17.7 competency.
The indications for lumbar puncture in headache and neurological disease are:
1. Suspected subarachnoid haemorrhage after negative CT head: CT performed within 6 hours excludes SAH in ~98% of cases; LP at ≥12 hours is required when CT is normal or equivocal, to detect xanthochromia.
2. Suspected meningitis or encephalitis: fever + headache + neck stiffness ± altered consciousness or rash. LP provides cell count, protein, glucose, Gram stain, culture to confirm diagnosis and guide antimicrobial therapy.
3. Suspected tuberculous meningitis (TBM): subacute headache with meningism in immunocompromised patients or TB contacts.
4. Suspected fungal meningitis (cryptococcal in HIV): India ink, cryptococcal antigen, and fungal culture.
5. Suspected carcinomatous meningitis: CSF cytology for malignant cells.
6. Idiopathic intracranial hypertension (IIH): measuring opening pressure and therapeutic CSF drainage.
7. Multiple sclerosis: CSF oligoclonal bands and IgG index.
The absolute contraindications to LP are:
- Evidence of raised ICP with risk of transtentorial herniation: papilloedema, focal neurological deficit, deteriorating consciousness, or CT showing midline shift, effaced basal cisterns, or posterior fossa mass. Performing LP in significantly elevated ICP can cause fatal coning.
- Infection at the LP site: risk of introducing infection into CSF.
- Uncorrected coagulopathy: platelet count <50,000/mm³ or INR >1.5 significantly increases spinal haematoma risk.
- Patient refusal (informed consent required).
Relative contraindications: anticoagulation, thrombocytopaenia in the 50,000–100,000 range, suspected spinal cord mass at LP level.
A critical clinical rule: CT before LP whenever any of the following are present: papilloedema, focal neurological deficit, altered or deteriorating consciousness, new onset seizure, immunocompromised state, or history of CNS mass. In a patient with fever, headache, and neck stiffness but GCS 15, no papilloedema, and no focal deficit — CT may not be required before LP if it will delay urgent antibiotic therapy; in this situation, start antibiotics immediately and perform LP within the hour.
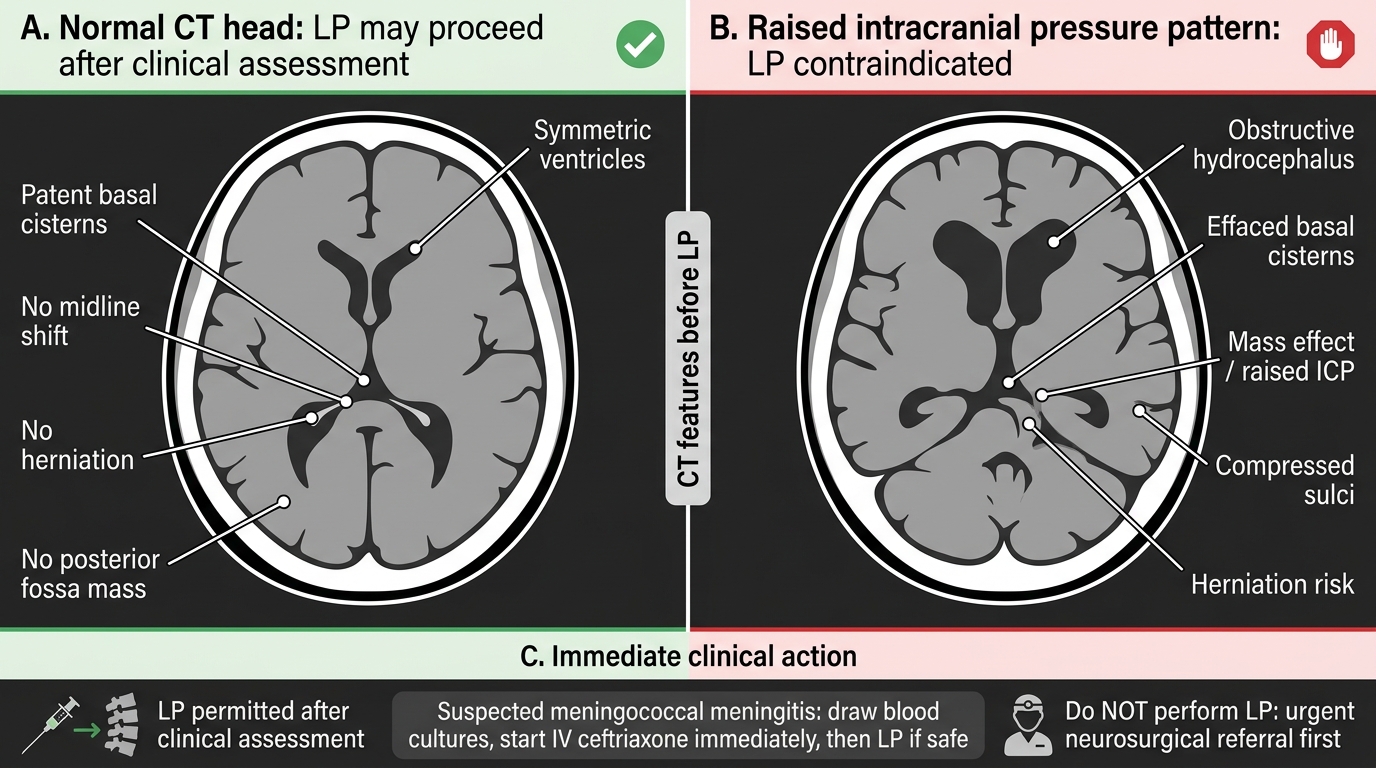
CT Head Features Before Lumbar Puncture
SELF-CHECK
A 22-year-old woman presents with fever (38.9°C), severe headache, and photophobia for 12 hours. On examination, she has neck stiffness (positive Kernig's sign) and a non-blanching petechial rash on her legs. She is alert with a GCS of 15. CT head is reported as normal with no papilloedema on fundoscopy. What is the most appropriate immediate management sequence?
A. MRI brain with contrast before any other intervention to characterise the meningeal disease
B. Lumbar puncture immediately, followed by IV ceftriaxone after CSF results return
C. IV ceftriaxone 2 g immediately, then LP within the next hour while antibiotics are running
D. Await blood culture results before starting antibiotics to preserve sensitivity
Reveal Answer
Answer: C. IV ceftriaxone 2 g immediately, then LP within the next hour while antibiotics are running
This presentation (fever, meningism, non-blanching petechial rash) is meningococcal meningitis/septicaemia until proven otherwise — a medical emergency. The correct sequence is: blood cultures drawn first (30 seconds), IV ceftriaxone 2 g started immediately without waiting for LP results, then LP performed as soon as safely possible. LP within the first 30–60 minutes after starting antibiotics still yields valuable CSF abnormalities: cell count, protein, and glucose remain abnormal, and Gram stain may still be positive. Delaying antibiotics to wait for LP significantly increases mortality. CT is already normal and MRI is not the urgent priority here. Awaiting blood cultures before antibiotics is dangerous in suspected meningococcaemia.
Lumbar Puncture Technique: Governing Principles
The governing anatomical and physiological principles that underpin safe LP must be mastered before the procedural steps can be understood. The lumbar puncture procedure requires correct patient positioning, precise landmark identification, and meticulous aseptic technique to minimise complications — and each of these requirements follows directly from anatomy.
The spinal cord in adults terminates at the conus medullaris at the level of L1–L2 (occasionally L2 in some individuals; at L3 in neonates). Below this level, the dural sac continues to S2 but contains only the cauda equina — a bundle of nerve roots descending to their respective foramina. Because these roots float freely in CSF rather than being fixed structures, a needle inserted into the lumbar cistern below L2 deflects them aside rather than transecting them. This anatomy is the reason LP is performed exclusively below L1–L2 in adults: above this level, the cord itself would be at risk of direct needle injury.
Tuffier's line — the horizontal line connecting the two posterior superior iliac crests — crosses the vertebral column at the L4 spinous process or the L4–L5 interspace. This is the primary surface landmark for identifying the LP site. The preferred interspace is L3–L4 (one space above Tuffier's line) or L4–L5 (at the landmark). The L3–L4 space is typically more reliably identifiable and avoids the lower dural sac where nerve roots are more densely packed.
The principle governing patient positioning for LP is lumbar flexion: flexing the lumbar spine opens the interspinous spaces and separates the spinous processes by stretching the interspinous ligaments, thereby creating a wider window for needle entry. The lateral decubitus (foetal) position — patient on their side, hips and knees maximally drawn up toward the chest, chin tucked — achieves maximum lumbar flexion. This is also the only position in which opening CSF pressure can be accurately measured, because in the sitting position the additional hydrostatic pressure from the column of CSF above the needle artificially elevates the reading.
The principle governing needle orientation relates to the microstructure of the dura mater: dural collagen fibres run longitudinally (craniocaudal). A needle bevel oriented parallel to these fibres separates rather than cuts them, resulting in a smaller functional dural defect that reseals more readily — the basis for the significantly reduced post-LP headache rate with parallel bevel orientation compared to perpendicular insertion.
The principle governing needle gauge: smaller gauge needles (22G, 25G) produce smaller dural defects and significantly reduce post-LP headache incidence (from ~30% with 18G to ~5% with 25G). The trade-off is slower CSF flow — a 25G needle may require several minutes to collect 5–10 mL of CSF. In emergency settings (suspected SAH, meningitis), a 22G needle balances speed and complication risk.
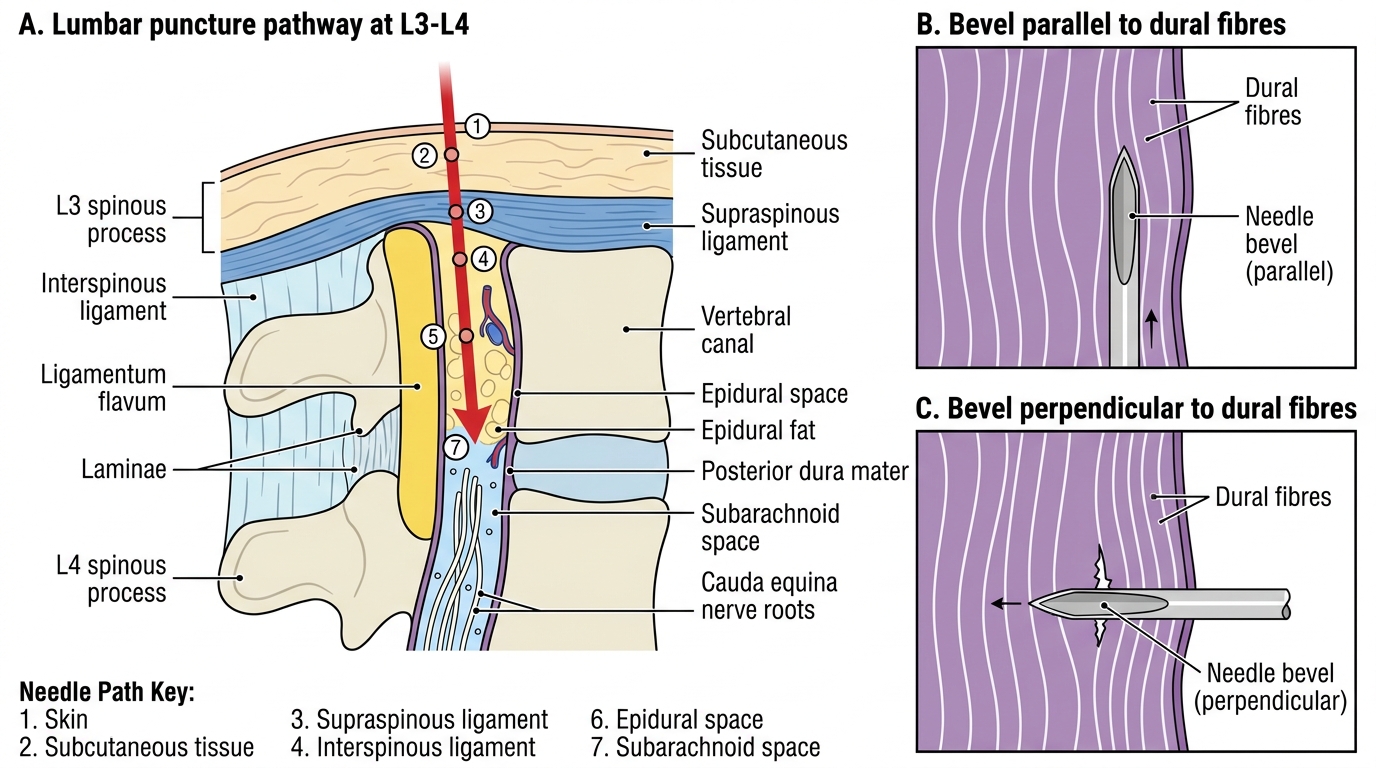
Lumbar Puncture Pathway at L3-L4