Page 1 of 21
IM17.{1,3} | Headache Foundations — SDL Guide
Learning Objectives
- Define headache and apply the ICHD-3 three-part classification framework to categorise headaches as primary, secondary, or cranial neuralgia
- Describe the distinguishing clinical features of migraine, tension-type headache, and cluster headache
- Classify migraine into its major subtypes including migraine with aura (classical) and without aura (non-classical), and identify key differences between them
- Apply the SNNOOP10 red-flag criteria to systematically screen for secondary headache causes
- Outline the initial investigation strategy for new-onset headache including the CT-then-LP protocol for thunderclap headache
INSTRUCTIONS
Headache is the most common neurological symptom in clinical practice. This module establishes the foundational classification framework — primary versus secondary headache — and provides the clinical criteria for diagnosing the major primary headache syndromes, with particular emphasis on migraine subtypes. Mastery of this framework enables every subsequent clinical decision in headache management.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 17 — Headache (textbook)
- API Textbook of Medicine, 10th ed. — Headache and Migraine (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed. — Headache (textbook)
- International Classification of Headache Disorders, 3rd edition (ICHD-3), International Headache Society, 2018 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajesh, a 34-year-old software engineer, presents to your outpatient clinic with a 3-year history of recurrent, debilitating headaches that he describes as a throbbing pain on the right side of his head. Each episode lasts 8–16 hours, begins with brief visual disturbances — zigzag lines and a blind spot — and is accompanied by nausea, vomiting, and such extreme light sensitivity that he retreats to a dark room. He has been self-medicating with paracetamol and ibuprofen almost daily. Now contrast Sunita, a 28-year-old nurse who presents with a constant, bilateral, pressure-like tightness 'like a band around my head' that worsens over long shifts, responds well to over-the-counter analgesics, and has no nausea or light sensitivity. Both complain of headache — yet the mechanism, classification, prognostic implication, and treatment approach are entirely different. And then there is Pankaj, a 45-year-old hypertensive man who tells you: 'I suddenly got the worst headache of my life while straining in the toilet.' For Pankaj, the headache is not a primary disorder at all — it is a warning sign of a potentially lethal intracranial catastrophe. Understanding headache begins with the ability to classify it correctly, because classification drives every subsequent clinical decision.
WHY THIS MATTERS
Headache is the most common neurological complaint in outpatient practice and is among the top five reasons for emergency department visits worldwide. In India, migraine alone affects an estimated 14–25% of the adult population, making it a major contributor to disability, lost productivity, and quality-of-life impairment. General Medicine requires competence in headache not merely to prescribe an analgesic, but to distinguish the benign and highly prevalent primary headaches from the rare but life-threatening secondary headaches that demand urgent investigation. Missing a subarachnoid haemorrhage, bacterial meningitis, or malignant hypertension in a headache presentation is among the most consequential errors in clinical medicine. The NMC competencies IM17.1 and IM17.3 require you to define and classify headache and to distinguish classical from non-classical migraine — the foundation on which all subsequent headache management rests.
RECALL
Activate your existing knowledge of intracranial anatomy and pain pathways. Recall that the brain parenchyma itself is pain-insensitive — nociceptors are present in the meninges (particularly the dura mater and its associated sinuses), the proximal segments of large intracranial vessels, the periosteum of the skull, and extracranial structures including the scalp muscles, sinuses, and cervical structures. Central sensitisation of the trigeminovascular system — which carries pain signals from meningeal blood vessels via the trigeminal nerve to the trigeminal nucleus caudalis in the brainstem — is the dominant mechanism for primary headache pain. Recall also from physiology that cortical spreading depression (CSD) — a wave of neuronal depolarisation followed by suppression, propagating at 3–5 mm/min across the cortex — is the electrophysiological correlate of the migraine aura. From pathology, recall that blood in the subarachnoid space is intensely meningeal irritant, producing the sudden catastrophic headache of subarachnoid haemorrhage. These foundational concepts will structure your understanding of how different causes produce different headache phenotypes.
Definition and Classification of Headache
Headache is defined as pain or discomfort arising from the head or upper neck. While this definition appears straightforward, its clinical importance lies not in the symptom itself but in identifying its cause and category — because the management, prognosis, and urgency of investigation differ dramatically across headache types. The International Classification of Headache Disorders, 3rd edition (ICHD-3), published by the International Headache Society (IHS) in 2018, is the globally accepted diagnostic framework and provides operationalised criteria for over 200 headache diagnoses. Understanding the top-level classification is essential for structured clinical reasoning at the final-year MBBS level.
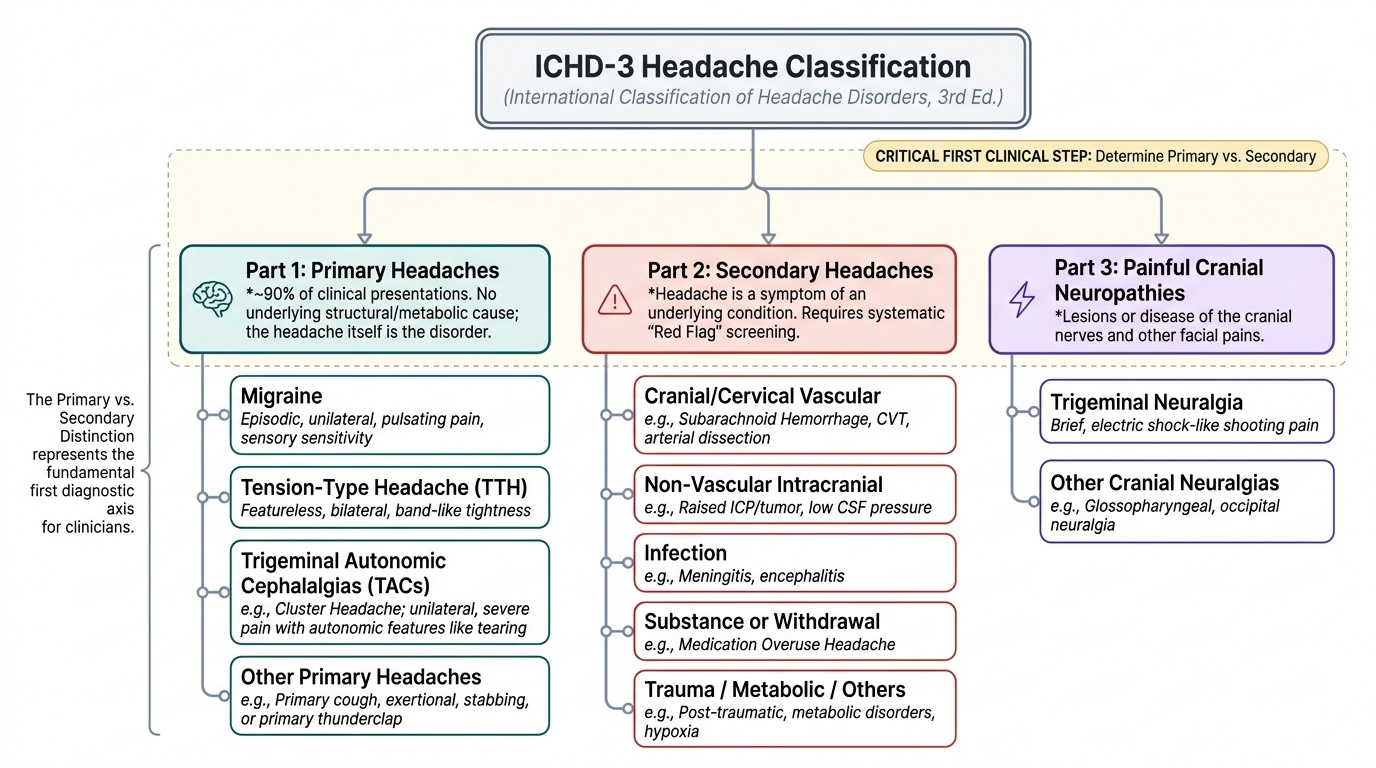
Provided image
The ICHD-3 divides all headaches into three major groups. Part 1: Primary headaches are those in which the headache itself constitutes the disorder — there is no underlying structural, vascular, infectious, or metabolic cause. The pain arises from altered pain-processing in the central nervous system, particularly through trigeminovascular sensitisation. The four primary headache diagnoses are: (1) migraine, (2) tension-type headache (TTH), (3) trigeminal autonomic cephalalgias (TACs) — of which cluster headache is the most important, and (4) other primary headache disorders (including primary stabbing, primary cough, primary exertional, and primary thunderclap headaches — but note that spontaneous thunderclap headache is secondary until proven otherwise). Primary headaches collectively account for over 90% of all headaches presenting in general practice.
Part 2: Secondary headaches are those caused by another underlying condition — the headache is a symptom, not the primary disorder. Secondary headaches are classified by their attributed cause, using the format 'headache attributed to [cause]'. Major secondary headache categories include: headache attributed to head or neck trauma, headache attributed to cranial or cervical vascular disorders (including subarachnoid haemorrhage, cerebral venous thrombosis, arterial dissection), headache attributed to non-vascular intracranial disorders (raised intracranial pressure from tumour or hydrocephalus, low CSF pressure from post-dural puncture), headache attributed to infection (meningitis, encephalitis), headache attributed to a substance or its withdrawal (medication-overuse headache, alcohol, carbon monoxide), headache attributed to disorders of homoeostasis (hypertensive emergency, hypoglycaemia, altitude sickness), and headache attributed to psychiatric disorders.
Part 3: Painful lesions of the cranial nerves and other facial pain — including trigeminal neuralgia, glossopharyngeal neuralgia, and persistent idiopathic facial pain.
The diagnostic implication of this three-part framework is precise: the first task in every headache consultation is to decide whether the headache is primary or secondary, because this single binary decision determines whether the patient can be reassured and treated symptomatically versus urgently investigated for a life-threatening cause. The ICHD-3 specifies that a diagnosis of primary headache may only be assigned when secondary causes have been reasonably excluded — it is never a default diagnosis of exclusion in an undifferentiated new-onset headache.
Primary Headache Syndromes: Overview
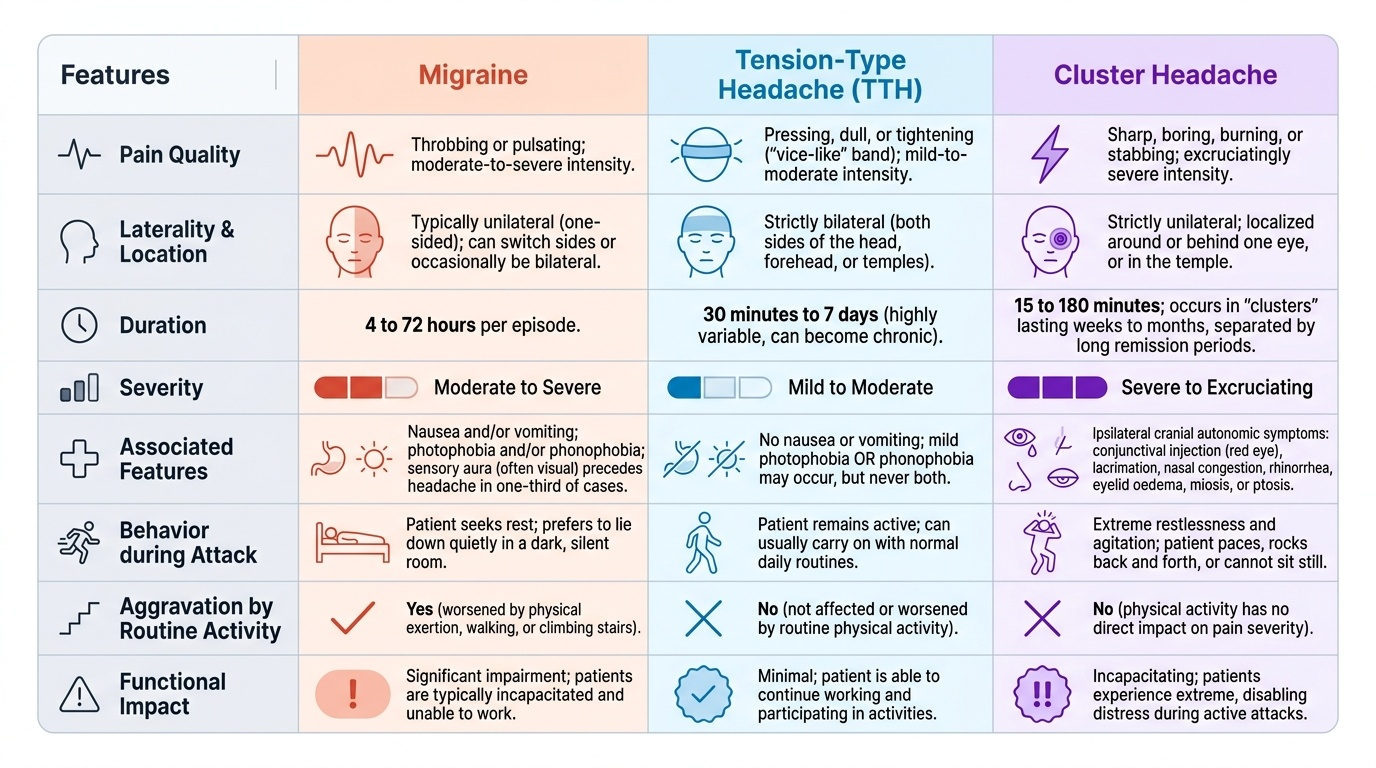
Among the primary headaches, three syndromes account for the overwhelming burden of disease in clinical practice and must be distinguished by their characteristic clinical profiles. Each has a distinct mechanism, demographic profile, temporal pattern, and set of associated features that allow bedside diagnosis without imaging in the majority of cases. The ability to differentiate these three syndromes confidently — migraine, tension-type headache, and cluster headache — using history alone is one of the most important clinical skills in general medicine.
Provided image
Migraine is characterised by recurrent episodes of moderate-to-severe unilateral (though not always) pulsating headache, typically lasting 4–72 hours, aggravated by routine physical activity, and associated with nausea and/or vomiting and photophobia and/or phonophobia. In one-third of patients, the headache is preceded by a transient, fully reversible aura — focal neurological symptoms that develop over 5–20 minutes and last up to 60 minutes. The most common aura type is visual. Migraine significantly impairs function — patients are typically unable to continue work or daily activities during an attack.
Tension-type headache (TTH) is the most prevalent headache disorder globally, affecting up to 70% of the adult population at some point in their lives. The pain is bilateral, pressing or tightening in quality (non-pulsating), mild to moderate in severity, and NOT aggravated by routine physical activity. Nausea is absent, and photophobia or phonophobia (but not both) may be present. TTH lacks the hallmark features of migraine — no pulsating quality, no unilaterality (typically), no functional impairment requiring rest, no aura.
Cluster headache belongs to the trigeminal autonomic cephalalgias and is arguably the most severe primary headache syndrome, described by patients as the most excruciating pain imaginable. It is characterised by strictly unilateral periorbital or temporal pain, severe to very severe in intensity, lasting 15–180 minutes, with a characteristic periodicity (occurring in 'clusters' of weeks to months separated by remission periods). The defining feature is ipsilateral cranial autonomic activation: lacrimation, conjunctival injection, nasal congestion or rhinorrhoea, eyelid oedema, miosis, and ptosis (partial Horner syndrome). Unlike migraine patients who prefer stillness, cluster headache patients are typically agitated and pace restlessly during attacks.
Pathophysiology of Primary Headache
Understanding the mechanism of primary headache explains not only why these syndromes occur, but why certain drugs work for certain headache types and not others. The dominant current model implicates the trigeminovascular system as the common final pathway for headache pain in both migraine and cluster headache, while tension-type headache appears to involve central sensitisation with altered pain thresholds.
In migraine, the sequence of events begins in the cortex and brainstem. In patients with aura, cortical spreading depression (CSD) — a slow wave of electrochemical neuronal depolarisation followed by prolonged suppression, propagating across the cortex at 3–5 mm/minute — generates the aura symptoms, with the specific symptom type depending on the cortical area affected (visual cortex: visual aura; somatosensory cortex: tingling/numbness). CSD also appears to activate trigeminal afferents innervating the meningeal vessels. In migraine without aura, the trigeminovascular activation likely originates in the brainstem (migraine generator regions including the locus coeruleus, dorsal raphe nucleus, and periaqueductal grey). Activation of the trigeminal sensory nerve terminals around meningeal vessels releases neuropeptides — primarily calcitonin gene-related peptide (CGRP) — causing vasodilation and neurogenic inflammation of the meningeal vessels. The pain signal is then transmitted via the trigeminal ganglion to the trigeminal nucleus caudalis (TNC) in the medullary dorsal horn, and then rostrally to the thalamus and cortex. Over repeated attacks, central sensitisation at the TNC level causes allodynia — where even non-painful stimuli (combing hair, touching skin) become painful.
In cluster headache, the episodic clustering pattern and circadian periodicity implicate the hypothalamus — specifically the posterior hypothalamus — as the generator, possibly through hypothalamic modulation of the trigeminal-autonomic reflex arc. Activation of the trigeminal system drives headache pain, while simultaneous activation of the parasympathetic outflow through the sphenopalatine ganglion produces the ipsilateral cranial autonomic features. PET and fMRI studies confirm hypothalamic activation during cluster attacks; this finding distinguishes cluster headache from migraine (which activates the brainstem, not the hypothalamus).
In tension-type headache, the mechanism involves reduced pain inhibition at the level of the central nervous system, probably mediated by decreased activity of descending pain-inhibitory pathways from the brainstem. Peripheral sensitisation of pericranial myofascial tissues (scalp, neck, and temporomandibular muscles) plays a greater role in episodic TTH, while central sensitisation becomes dominant in chronic TTH. The absence of trigeminovascular activation explains why TTH lacks nausea, vomiting, photophobia, and phonophobia as cardinal features.
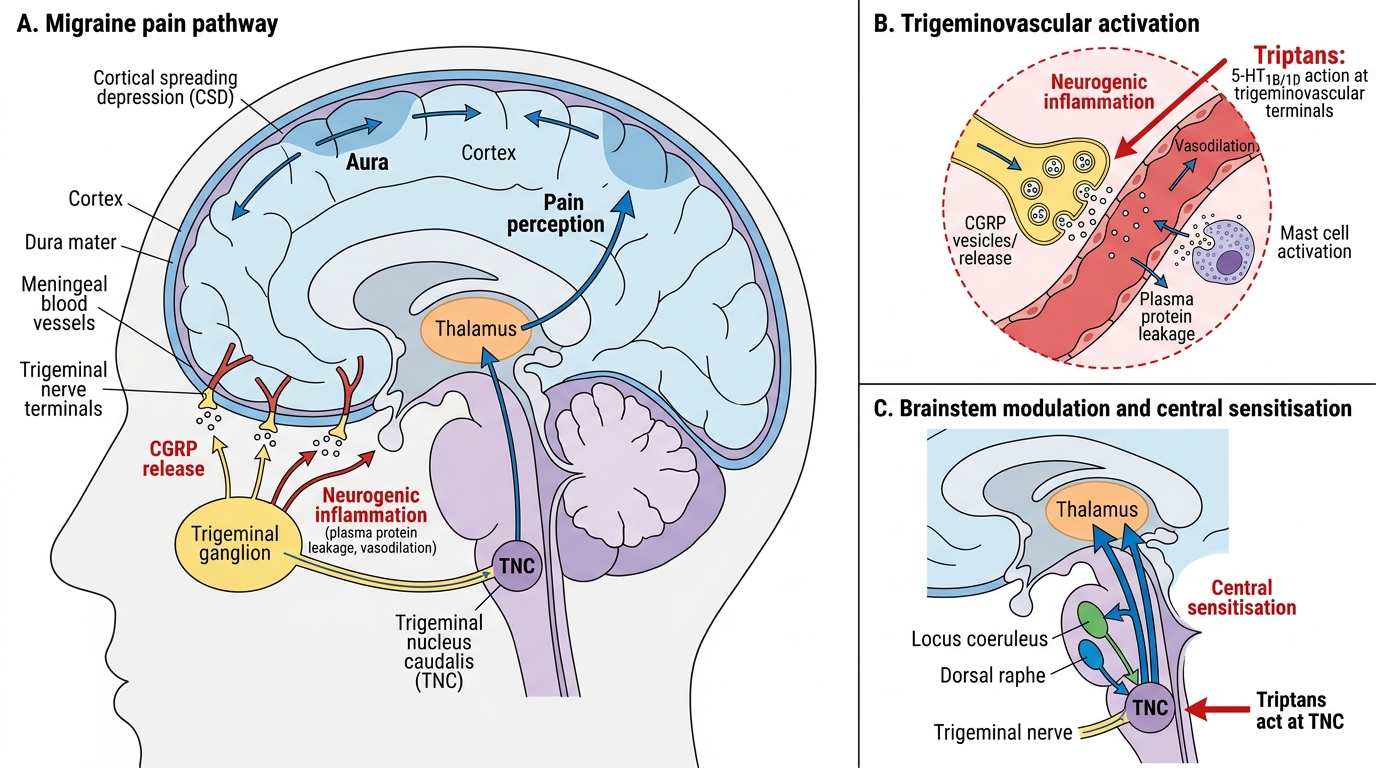
Migraine Pathophysiology and Triptan Targets