Page 8 of 21
IM18.8-9 | Stroke Diagnostic Testing — SDL Guide (Part 2)
Interpreting Stroke Imaging — Systematic Approach
Interpreting stroke imaging in clinical practice requires an integrated read — synthesising the imaging findings with the clinical story to reach a diagnostic and management conclusion. Isolated pattern recognition (identifying a hyperdense spot) without clinical context produces errors; the correct interpretation is always 'in this patient, in this clinical context, with this history and these vital signs, this finding means X and leads to action Y.' A systematic reading routine prevents the most common errors: missing a subtle haematoma, under-calling early ischaemic changes, or over-interpreting normal anatomical variants as pathology. This section provides a five-step CT read that can be completed in under two minutes at the bedside, and applies it to representative cases that directly mirror what you will encounter in ward rounds, OSCE radiology stations, and the first days of your internship in a casualty setting.
Systematic CT brain read in acute stroke — 5 steps, under 2 minutes:
- Window correctly: brain window (W:80, L:40) for parenchyma; bone window (W:3000, L:600) if structural concern
- Scan for hyperdensity bilaterally and symmetrically: acute blood (HU 60–80) = hyperdense. Hypertensive ICH sites: putamen (most common), thalamus, cerebellum, pons. Hyperdense vessel = large vessel thrombus
- Look for early ischaemic changes: loss of insular ribbon, sulcal effacement, grey-white blurring at basal ganglia. These are subtle — if uncertain, document 'early ischaemic changes cannot be confidently excluded' and proceed
- Score ASPECTS: mentally note the 10 MCA regions and count those with early change; subtract from 10
- Review CTA (if acquired): identify vessel occlusion site, characterise cervical vessels for stenosis or dissection
MRI interpretation in stroke:
DWI is the key sequence. Bright DWI + dark ADC = acute restricted diffusion = ischaemic infarction (minutes after onset). Check FLAIR: if DWI-positive area is dark on FLAIR = infarct <4.5–6 hours (DWI-FLAIR mismatch). If FLAIR also bright = infarct >6 hours. Check GRE/SWI for haemorrhage (blooming dark signal) and microbleeds.
Applied clinical cases:
Case 1: NCCT: 25 mm × 20 mm hyperdense lesion in the right putamen in a 62-year-old hypertensive patient. → Acute hypertensive ICH. No thrombolysis. Management: BP control (target systolic <140 mmHg), coagulation screen, neurosurgical assessment, CTA for spot sign.
Case 2: NCCT: normal. CTA: non-opacification of left M1 MCA. CTP: core 25 mL, penumbra 90 mL. Patient within 90 minutes. → Left M1 MCA occlusion with large penumbra. Candidate for both IV thrombolysis AND mechanical thrombectomy. Activate thrombectomy team immediately.
Case 3: NCCT: early ischaemic changes in 6 of 10 MCA territory regions. ASPECTS = 4. → Large established infarct, ASPECTS 4. High risk of haemorrhagic transformation; NOT an ideal thrombectomy candidate. Conservative management unless clinical severity is extreme.
Case 4: MRI: DWI bright in right lateral medulla, ADC dark. T1 fat-sat neck: crescent of T1 hyperintensity within the right vertebral artery wall. → Acute right lateral medullary infarction from right vertebral artery dissection. Management: antiplatelet therapy (most centres) or anticoagulation if embolic mechanism; investigate for connective tissue disease.
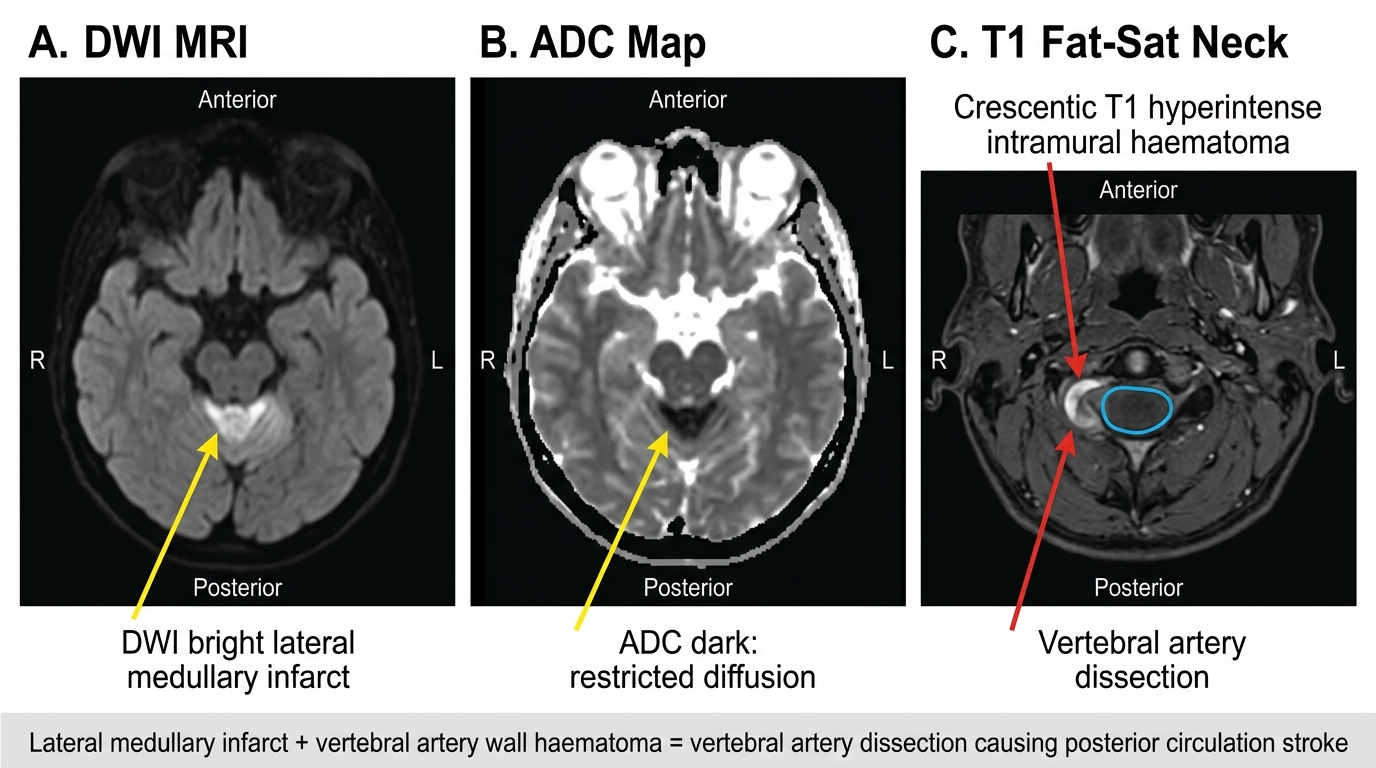
MRI Findings in Vertebral Artery Dissection with Lateral Medullary Infarct
Investigation of Haemorrhagic Stroke
Haemorrhagic stroke — both intracerebral haemorrhage (ICH) and subarachnoid haemorrhage (SAH) — requires a systematic investigative approach beyond simply confirming the haemorrhage. The key questions are: what is the underlying cause (hypertensive, anticoagulant-related, AVM, tumour, CAA, vasculitis, or aneurysm)? Is there a surgically correctable lesion? Is haematoma expansion in progress? Does the patient need neurosurgical intervention? Getting these questions right determines the management and the risk of rebleeding.
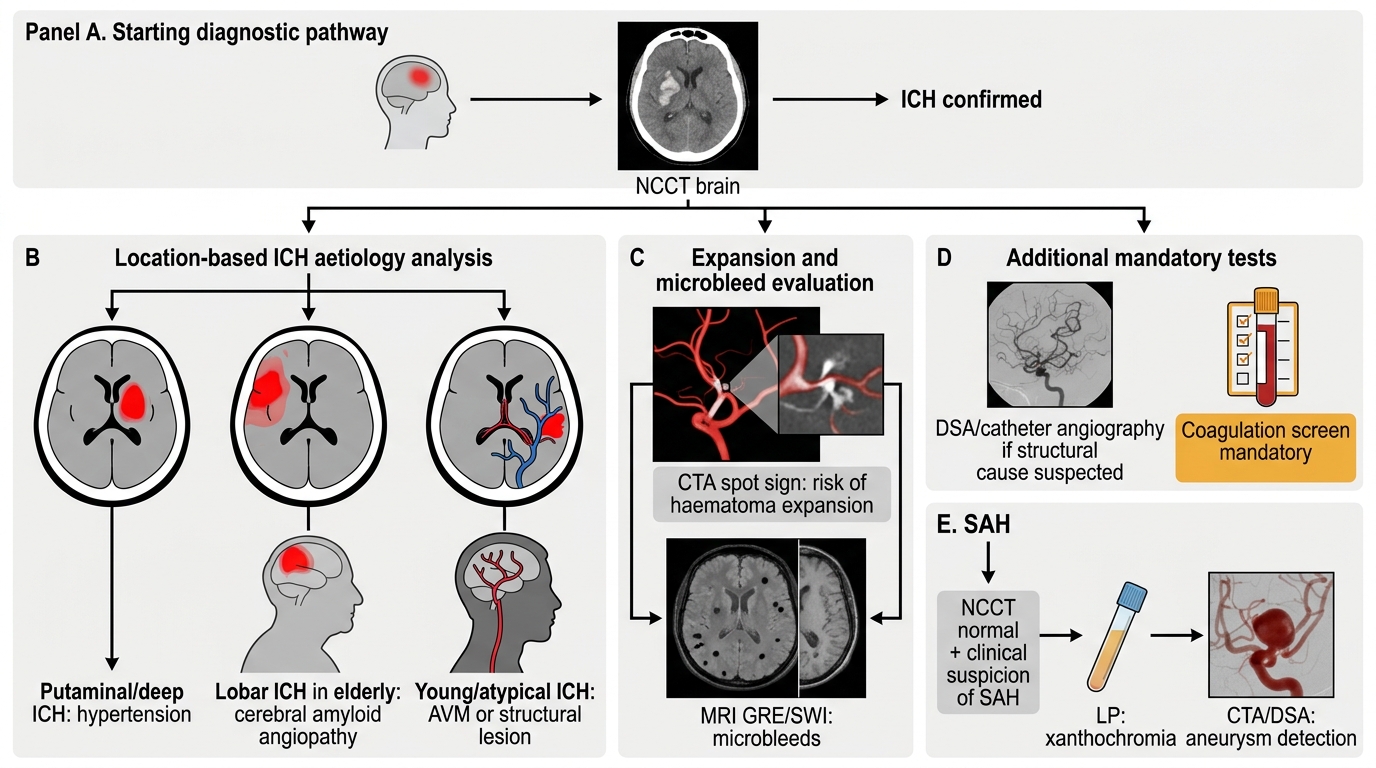
Investigation of ICH:
NCCT confirms haemorrhage and location. The location itself is the most important diagnostic clue. Characteristic sites of hypertensive ICH (from Charcot-Bouchard microaneurysm rupture) are: putamen (50%), thalamus (15%), cerebellum (10%), pons (10%), and lobar white matter (15%). In a hypertensive patient with putaminal haemorrhage, the diagnosis is almost certain. By contrast, lobar ICH in an elderly patient with cortical/subcortical haemorrhage and microbleeds on GRE/SWI = cerebral amyloid angiopathy (CAA). In a young patient with non-hypertensive lobar ICH = suspect AVM, cavernous malformation, tumour bleed, or CVST with haemorrhagic infarction.
Additional imaging for ICH:
- CTA 'spot sign': active extravasation of contrast into the haematoma on CTA = ongoing bleeding and haematoma expansion in progress; associated with early neurological deterioration and high 30-day mortality — a high-urgency finding
- MRI GRE/SWI: multiple microbleeds in a lobar distribution = CAA; multiple deep microbleeds = hypertensive small vessel disease
- MRI with contrast enhancement: ring-enhancing lesion = underlying tumour or abscess; AVM nidus or cavernous malformation
- Catheter digital subtraction angiography (DSA): gold standard for AVM and aneurysm — indicated when a structural lesion is suspected and CTA is inconclusive, particularly in young patients or atypical location without hypertension
Coagulation screen is mandatory in all ICH: INR >1.7 = anticoagulant-related ICH requiring urgent reversal; APTT prolonged = heparin effect or factor deficiency; thrombocytopenia = DIC or ITP.
CSF examination in SAH:
When SAH is clinically suspected (thunderclap headache — sudden-onset worst headache of the patient's life) but NCCT brain is normal, lumbar puncture is mandatory. NCCT misses approximately 2–5% of SAH (small volume bleeds or early presentation). CSF diagnostic finding: xanthochromia (yellow discolouration of the centrifuged supernatant due to bilirubin from oxyhaemoglobin breakdown) — appears 2–4 hours after onset, persists up to 2 weeks; distinguishes true SAH from traumatic tap (fresh blood without xanthochromia that clears across successive tubes). Spectrophotometry for xanthochromia is more sensitive than visual inspection alone.
Cerebral angiography after SAH:
CTA or catheter DSA is mandatory after SAH to identify and characterise the causative aneurysm — its size, neck-to-dome ratio, and relationship to surrounding vessels — before neurosurgical clipping or endovascular coiling.
ICH and SAH Investigation Algorithm
Self-Assessment: Stroke Diagnostic Testing
The investigation of stroke spans neuroimaging, vascular imaging, cardiac workup, and laboratory testing — with different priorities for the acute phase versus the aetiological workup phase, and a fundamentally different strategy for young stroke. The self-assessment below applies the full diagnostic framework across the range of presentations you will encounter in exams and clinical practice. Work through each scenario independently before reading the analysis, noting not only the correct investigation but also the reasoning chain that selects it.
Scenario A: A 67-year-old diabetic hypertensive woman presents with sudden right hemiplegia at 14:30. Last known well: 13:45. NIHSS = 12. NCCT brain: normal (no haemorrhage). CTA: proximal left M1 MCA not opacified. CTP: core 18 mL, penumbra 85 mL (mismatch ratio 4.7). BP 190/100 mmHg. What is the immediate imaging-driven management?
Analysis: NCCT normal → no haemorrhage → thrombolysis not contraindicated on imaging. CTA shows M1 occlusion → large vessel occlusion = mechanical thrombectomy indicated. CTP shows large penumbra-core mismatch → substantial salvageable tissue. BP 190/100 → must reduce to <185/110 before giving IV thrombolysis (labetalol 10–20 mg IV). Time from onset: 45 minutes — well within thrombolysis window. Plan: IV alteplase/tenecteplase + immediate thrombectomy activation (tandem strategy). Aetiological workup to follow: ECG, Holter, TTE, carotid duplex, fasting lipids, HbA1c.
Scenario B: A 40-year-old man with no known vascular risk factors has acute right capsular ischaemic stroke. Standard workup (ECG, TTE, carotid duplex, routine labs) is unrevealing. What constitutes the young stroke extended workup and in what order?
Analysis: Extended workup for young cryptogenic stroke: (1) T1 fat-saturation MRI of neck bilaterally — dissection (#1 cause in young adults); (2) TOE with bubble contrast — PFO (40–50% of young cryptogenic stroke); (3) Prolonged cardiac monitoring (Holter 24h minimum, ICM if remains cryptogenic); (4) Thrombophilia screen: protein C/S, AT-III, factor V Leiden, prothrombin G20210A, homocysteine; (5) APS panel (lupus anticoagulant, anticardiolipin, anti-β2GP1) — repeat in 12 weeks if positive; (6) Vasculitis screen: ANA, ANCA, anti-dsDNA, complement, ESR, CRP; (7) Haematological screen: FBC, peripheral smear, sickle cell test; (8) MRI with MRV for CVST; (9) Social history: OCP use, illicit drugs; (10) Genetic testing if family history of early stroke.
Scenario C: A 72-year-old man on warfarin for AF (INR 3.6) presents with a 35 mL right thalamic ICH with intraventricular extension. BP 186/104 mmHg. What investigations confirm the diagnosis and guide immediate management?
Analysis: NCCT confirms ICH (thalamic location). CTA immediately for spot sign (active expansion?). Coagulation screen confirms INR 3.6. Immediate reversal: vitamin K 10 mg IV PLUS 4-factor prothrombin complex concentrate (PCC) — preferred over FFP (faster reversal, lower volume). Target INR <1.5. BP management: target systolic <140 mmHg (INTERACT-2/ATACH-2 evidence). Neurosurgery review: intraventricular extension → consider external ventricular drain for obstructive hydrocephalus. Do NOT restart warfarin acutely; re-evaluate at 4–8 weeks with neurology and cardiology for anticoagulation restart decision.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
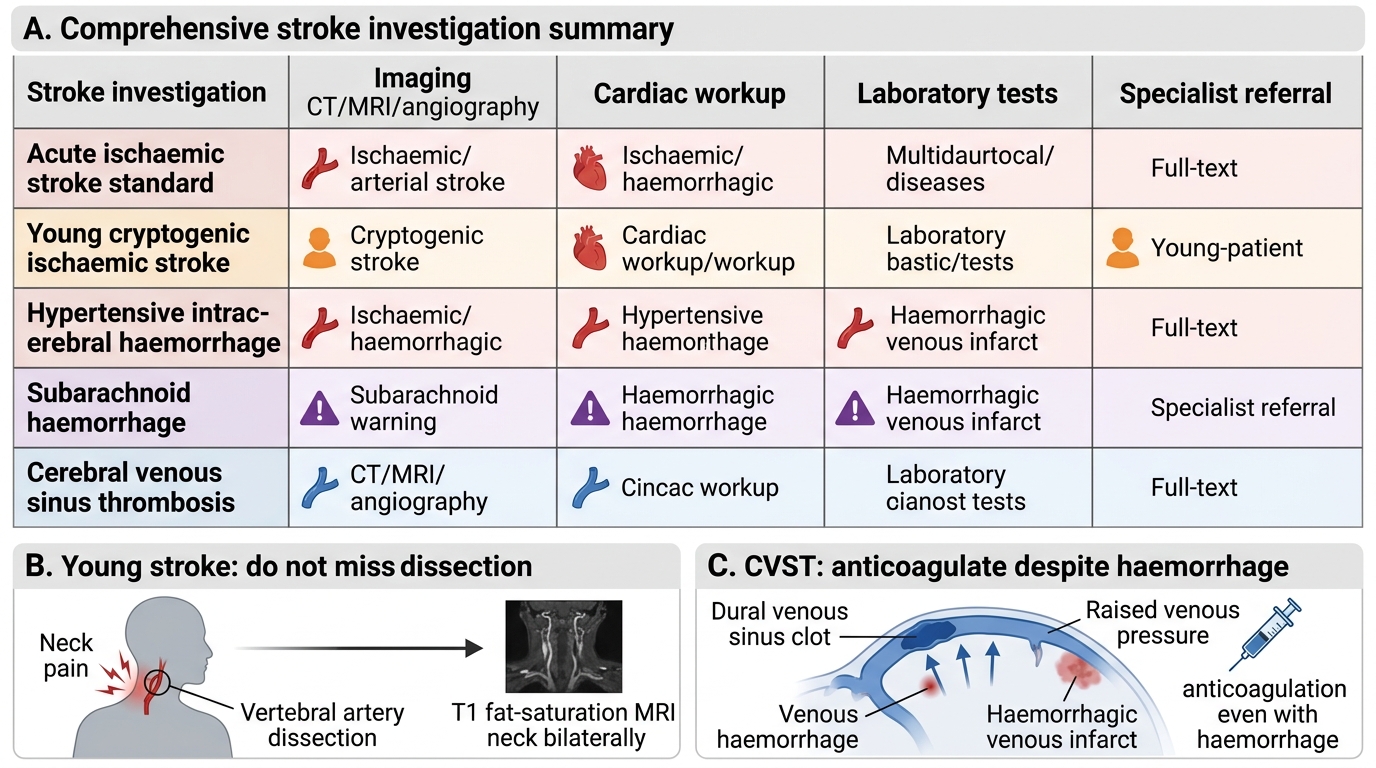
Comprehensive Stroke Investigation Summary
CLINICAL PEARL
In young stroke, the most commonly missed diagnosis is arterial dissection — and the most commonly missed investigation is T1 fat-saturation MRI of the neck bilaterally. A standard MRI brain does not image the cervical vessels adequately. The history clue is neck or head pain in the days before the stroke, or minor trauma. A young person with a lateral medullary syndrome and ipsilateral neck pain has vertebral artery dissection until proven otherwise.
A second pearl: CVST is treated with anticoagulation EVEN when the CT shows haemorrhage. The haemorrhage in CVST is venous (from raised venous pressure), not arterial. Anticoagulation stops thrombosis propagation, reduces venous hypertension, and actually reduces further haemorrhagic risk. Withholding anticoagulation in CVST because of CT haemorrhage is a potentially fatal error — one of the most important exceptions in stroke medicine.