Page 1 of 21
IM18.1-2 | Stroke Foundations — SDL Guide
Learning Objectives
- Describe the vascular anatomy of the brain — anterior and posterior circulations, Circle of Willis, perforating arteries — and correlate arterial territory with clinical stroke syndromes
- Classify cerebrovascular accidents into ischaemic (TOAST subtypes) and haemorrhagic (ICH, SAH) categories with their respective aetiologies and pathogenic mechanisms
- Enumerate genetic and acquired risk factors for both ischaemic and haemorrhagic stroke and explain their pathogenic contributions
- Explain the ischaemic penumbra concept and its therapeutic implications for the thrombolysis and thrombectomy windows
- Apply the initial clinical approach — FAST/BEFAST, blood glucose check, NIHSS, NCCT brain — to a patient presenting with acute focal neurological deficit
INSTRUCTIONS
This module covers the foundational knowledge for stroke — vascular anatomy, pathological classification, aetiology, risk factors, and the ischaemic penumbra concept. It is the prerequisite for all subsequent stroke modules on clinical evaluation, imaging, acute management, and rehabilitation. Read the vascular anatomy section with the cerebral territory map at your side; the clinical syndromes will then follow logically from the anatomy rather than requiring rote memorisation.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 427 — Ischaemic Stroke (textbook)
- API Textbook of Medicine, 10th ed. — Cerebrovascular Diseases (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 26 — Stroke (textbook)
- AHA/ASA Guidelines for the Early Management of Patients with Acute Ischaemic Stroke, 2019 (updated 2021) (guideline)
- Indian Stroke Association Consensus Statement on Stroke, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At 3 am, a 62-year-old hypertensive male is brought to the casualty by his wife. He woke suddenly with the left side of his body unresponsive — left arm hanging limp, left leg dragging on the floor, and speech coming out as slurred, effortful monosyllables. He had been completely well at midnight. She noticed that the left corner of his mouth drooped as he tried to speak. By the time he reaches the emergency department, 40 minutes have elapsed. His blood pressure is 182/104 mmHg. You have just 4 hours and 10 minutes left before the thrombolysis window closes. Every minute of delay translates into approximately 1.9 million neurons, 14 billion synapses, and 12 km of myelinated axon fibres irreversibly lost. To act correctly in these minutes, you need to know precisely which artery has occluded, why it has occluded, and what the pathophysiology inside that vessel and its territory now looks like. This module builds that foundational knowledge — the vascular anatomy, the stroke classifications, and the aetiologies that determine both the clinical picture and the treatment.
WHY THIS MATTERS
Stroke is the second leading cause of death and the leading cause of adult acquired disability worldwide. In India, the burden is substantial and growing: stroke accounts for approximately 1.5–2.0 million new cases annually, with case-fatality rates in the range of 20–30% at 30 days in hospital settings, and over half of survivors remaining disabled. The NMC competency IM18.1–IM18.2 requires you to describe the functional and vascular anatomy of the brain and to classify cerebrovascular accidents — knowledge that is the obligatory first step before any clinical decision-making. For a final-year MBBS student, stroke is a day-one emergency in your internship: you will be the first point of contact in the casualty, the person who decides whether to call for urgent CT, and the one who starts initial management. Understanding the anatomy underpins every clinical sign you elicit, and understanding the aetiology determines the secondary prevention strategy you must explain to the patient and family.
RECALL
Before proceeding, activate what you already know. From your earlier neuroscience and anatomy studies, recall that the brain is supplied by two major systems: the anterior circulation arising from the internal carotid arteries and the posterior circulation arising from the vertebral arteries, which unite to form the basilar artery. These two systems are joined at the base of the brain by the Circle of Willis (circulus arteriosus), which allows collateral flow between the two circulations. Recall that neurons are exquisitely sensitive to ischaemia — they begin to die after approximately 4–6 minutes of complete ischaemia, which is why the stroke slogan 'time is brain' is biologically grounded. Recall from pathology your knowledge of atherosclerosis — the process of endothelial injury, lipid accumulation, plaque formation, and eventual luminal narrowing or plaque rupture — because this is the shared mechanism underlying both cerebral and coronary vascular disease. Also recall that blood pressure is the single most important modifiable risk factor for stroke, and that hypertension accelerates both large-vessel atherosclerosis and small-vessel lipohyalinosis.
Functional and Vascular Anatomy of the Brain
A detailed understanding of the vascular anatomy of the brain is indispensable for stroke localisation and is the anatomical foundation upon which every clinical decision in stroke medicine rests. The brain receives approximately 750 mL of blood per minute — 15% of cardiac output — despite comprising only 2% of body weight, reflecting its extraordinary and unrelenting metabolic demands. Unlike other organs, the brain cannot tolerate more than a few minutes of ischaemia without irreversible injury because it has negligible glycogen stores and relies entirely on continuous delivery of glucose and oxygen via the bloodstream. This supply arrives via four arteries: the right and left internal carotid arteries (ICA) and the right and left vertebral arteries. The internal carotid arteries constitute the anterior circulation and supply the majority of the cerebral hemispheres. The vertebral arteries constitute the posterior circulation and supply the brainstem, cerebellum, and occipital lobes. Knowing which artery supplies which territory is the key to localising a stroke from clinical signs alone — before any imaging is obtained.
The anterior circulation (carotid system) consists of the following vessels and their territories:
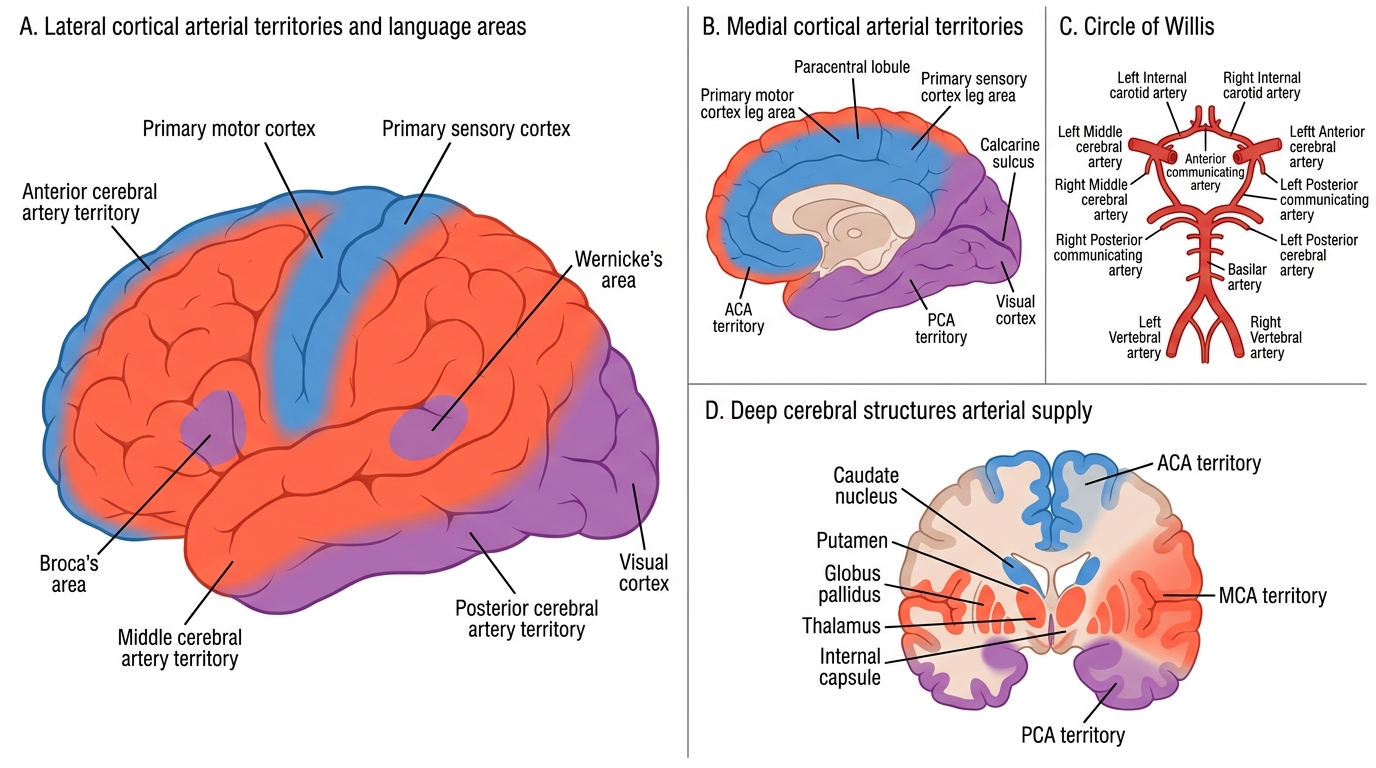
- Middle cerebral artery (MCA): the largest branch of the ICA; it supplies the lateral surface of the frontal, parietal, and temporal lobes, including the primary motor cortex (lateral portion — arm, face), primary sensory cortex (lateral), Broca's area (inferior frontal gyrus, left hemisphere), Wernicke's area (superior temporal gyrus, left hemisphere), and deep white matter including the internal capsule via lenticulostriate branches. MCA occlusion is the most common stroke syndrome, producing contralateral hemiplegia (arm > leg because the face-arm area is lateral), hemisensory loss, and aphasia if the dominant hemisphere is involved.
- Anterior cerebral artery (ACA): supplies the medial surface of the frontal and parietal lobes; the leg area of the primary motor and sensory cortex lies on this medial surface. ACA occlusion classically causes contralateral leg weakness greater than arm weakness — the reverse of MCA stroke — along with primitive reflexes (grasp, suck) and abulia.
- Anterior choroidal artery: a direct branch of the ICA that supplies the posterior limb of the internal capsule, the optic tract, and parts of the medial temporal lobe. Its occlusion causes a classic triad of contralateral hemiplegia, hemianopia, and hemisensory loss.
The posterior circulation (vertebrobasilar system) includes:
- Posterior cerebral artery (PCA): supplies the occipital lobe and inferomedial temporal lobe. PCA occlusion produces contralateral homonymous hemianopia as the most prominent feature; if the thalamus (supplied by thalamo-perforating branches) is involved, thalamic pain, hemisensory loss, and sometimes memory impairment occur.
- Basilar artery and its branches: supply the pons, midbrain, and cerebellum. Basilar occlusion is a catastrophic event producing coma, quadriplegia, and locked-in syndrome (intact consciousness but unable to move any limbs, only able to blink — because the corticospinal and corticobulbar tracts are compressed or infarcted in the pons while the reticular formation is spared).
- Posterior inferior cerebellar artery (PICA): supplies the lateral medulla and posterior inferior cerebellum. Its occlusion produces Wallenberg syndrome (lateral medullary syndrome) — ipsilateral facial numbness, contralateral body numbness (spinothalamic), ipsilateral Horner syndrome (ptosis, miosis, anhidrosis), ipsilateral limb ataxia, dysphagia, and dysarthria.
- Anterior inferior cerebellar artery (AICA) and superior cerebellar artery (SCA): supply different parts of the cerebellum and pons; their occlusion produces cerebellar ataxia, vertigo, and various pontine signs.
The Circle of Willis at the base of the brain connects the anterior and posterior circulations. It is formed by the anterior communicating artery (connecting the two ACAs), the posterior communicating arteries (connecting the ICA with the PCA on each side), and the proximal segments of the ACA, MCA, PCA, and basilar artery. The clinical importance of the Circle of Willis is that it provides a route for collateral flow when one major vessel is occluded, potentially limiting infarct size — though the Circle is anatomically complete in only approximately 20–25% of individuals.
Perforating (deep) arteries arise at right angles from the major surface arteries and penetrate deep into the brain to supply the basal ganglia, thalamus, internal capsule, and brainstem. These are small-calibre, end arteries — the lenticulostriate arteries (from the MCA), the thalamoperforating arteries (from the PCA and basilar), and the basilar perforating arteries. Because they are end arteries (no collateral flow), occlusion of a single perforating artery produces a small, round infarct called a lacune (from the Latin for 'gap'). The absence of collateral flow means lacunar infarcts are clinically well-circumscribed, producing the classic lacunar syndromes.
Cerebral Arterial Territories and Circle of Willis
The functional anatomy relevant to stroke localisation follows directly from the vascular territories:
- Motor function: primary motor cortex (precentral gyrus); fibres descend as the corticospinal tract through the internal capsule (posterior limb) → cerebral peduncle → pyramidal decussation at the medullary-cervical junction → lateral corticospinal tract → anterior horn cells. This long route means that a single lesion anywhere from cortex to spinal cord can produce an upper motor neuron (UMN) pattern — ipsilateral cranial nerve signs + contralateral body weakness if supratentorial; crossed signs if brainstem.
- Speech/language: Broca's area (posterior inferior frontal gyrus, left hemisphere) = motor/expressive speech production; Wernicke's area (posterior superior temporal gyrus, left hemisphere) = receptive/language comprehension. The arcuate fasciculus connects them; damage to it produces conduction aphasia.
- Visual fields: the optic radiation sweeps through the temporal and parietal lobes en route to the primary visual cortex (calcarine cortex, occipital lobe). Partial optic radiation injury produces quadrantanopia; complete occipital cortex injury produces homonymous hemianopia with macular sparing (dual blood supply of the macular cortex).
Classification of Cerebrovascular Accidents
Cerebrovascular accident (CVA) — or stroke — is defined clinically as a rapidly developing episode of focal or global neurological dysfunction lasting more than 24 hours (or leading to death), caused by vascular pathology of the brain. The 24-hour criterion distinguishes a completed stroke from a transient ischaemic attack (TIA), in which symptoms resolve within 24 hours (though the modern imaging-based definition defines TIA as transient neurological symptoms with no infarction on diffusion-weighted MRI, even if symptoms last less than 24 hours). The pathological classification is the most clinically important, as it directly determines management.
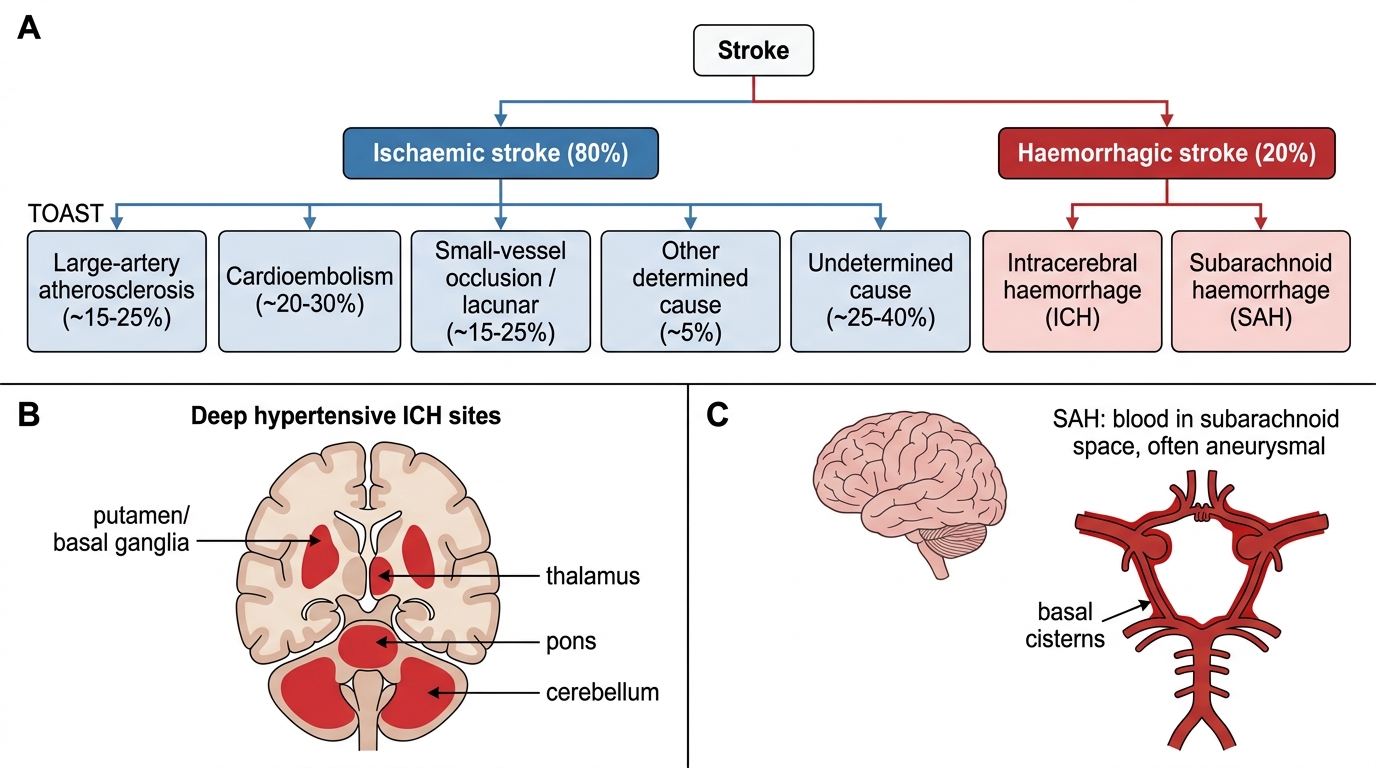
1. Ischaemic stroke (approximately 80% of all strokes): caused by focal cerebral ischaemia from arterial occlusion. Ischaemic stroke is further classified by mechanism using the TOAST classification (Trial of Org 10172 in Acute Stroke Treatment), which identifies five subtypes:
- Large artery atherosclerosis (20–25% of ischaemic stroke): stenosis or occlusion of a major intracranial or extracranial artery (carotid, MCA, vertebrobasilar) due to atherosclerotic plaque. The two mechanisms are (a) thrombosis in situ — plaque rupture with platelet-rich thrombus formation at the stenotic segment, and (b) artery-to-artery embolism — a fragment of the thrombus dislodges and occludes a more distal vessel. Risk factors: hypertension, diabetes mellitus, hypercholesterolaemia, smoking. CT/MRI shows a cortical or subcortical infarct in the territory of the stenosed artery; carotid duplex or CT angiography shows the stenosis.
- Cardioembolism (20–25% of ischaemic stroke): a thrombus forming in the heart embolises to a cerebral artery. The commonest cardiac sources are atrial fibrillation (AF) — the left atrial appendage is the site of thrombus formation due to stagnant blood in AF — rheumatic mitral stenosis, mechanical heart valves, recent myocardial infarction (mural thrombus), dilated cardiomyopathy, endocarditis (septic or marantic emboli), and patent foramen ovale (paradoxical embolism). In India, rheumatic heart disease (predominantly mitral stenosis with AF) remains an important cardioembolic cause, unlike in high-income countries where non-valvular AF predominates. Cardioembolic infarcts tend to be large (because emboli are large), cortical, and may be haemorrhagic (due to reperfusion into infarcted tissue). Multiple simultaneous infarcts in different arterial territories strongly suggest a cardiac embolic source.
- Small vessel occlusion (lacunar, 20–25% of ischaemic stroke): occlusion of a single deep perforating artery, causing a small spherical infarct of diameter ≤15 mm in the basal ganglia, internal capsule, thalamus, or pons. The underlying vessel pathology is lipohyalinosis (hyaline thickening and narrowing of the vessel wall, driven by chronic hypertension and diabetes) rather than atherosclerosis. Lacunar infarcts do not involve the cortex; therefore, there is no aphasia, no homonymous hemianopia, and no disturbance of consciousness. The classic lacunar syndromes are: (a) pure motor hemiplegia — face, arm, and leg weakness without sensory loss (internal capsule or pons); (b) pure sensory stroke — hemisensory loss without motor deficit (thalamus); (c) ataxic hemiparesis — ipsilateral ataxia with contralateral hemiparesis (pons or internal capsule); (d) dysarthria-clumsy hand syndrome — dysarthria, dysphagia, and clumsiness of one hand (pons); (e) sensorimotor stroke — combined motor and sensory deficit (thalamo-capsular area).
- Stroke of other determined aetiology (5%): includes hypercoagulable states (antiphospholipid syndrome, protein C/S deficiency, factor V Leiden), vasculitis (CNS vasculitis, systemic lupus erythematosus, giant cell arteritis), arterial dissection (spontaneous or traumatic — vertebral or carotid artery), haematological disorders (sickle cell disease, polycythaemia, thrombocythaemia), venous sinus thrombosis, migraine with aura (migrainous infarction, rare), and CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy). This category is disproportionately represented in young stroke (age <45 years).
- Cryptogenic stroke (30–35%): no cause identified despite adequate evaluation. Some of these are later found to be due to paroxysmal AF (detected on prolonged cardiac monitoring) or Patent Foramen Ovale (PFO) with paradoxical embolism.
2. Haemorrhagic stroke (approximately 20% of all strokes): caused by rupture of a blood vessel with bleeding into brain tissue or the subarachnoid space. Haemorrhagic stroke carries higher early mortality than ischaemic stroke.
- Intracerebral haemorrhage (ICH, approximately 10–15% of all strokes): spontaneous bleeding into brain parenchyma. The most common cause (80–85% of ICH) is hypertensive small vessel disease — long-standing hypertension causes microaneurysm formation (Charcot-Bouchard microaneurysms) at bifurcations of deep perforating arteries; rupture of these microaneurysms causes haemorrhage into characteristic locations: putamen (50% of hypertensive ICH), thalamus (15%), cerebellum (10%), pons (10%), lobar (white matter, 15%). The other important cause of lobar ICH, particularly in the elderly, is cerebral amyloid angiopathy (CAA) — deposition of amyloid-beta in the walls of cortical and leptomeningeal vessels, making them fragile and prone to rupture. ICH due to CAA causes lobar haemorrhages, which may be recurrent. Other causes include anticoagulant therapy (warfarin, DOACs), haemorrhagic transformation of ischaemic infarction, arteriovenous malformation (AVM), venous sinus thrombosis with haemorrhagic infarction, and brain tumour.
- Subarachnoid haemorrhage (SAH, approximately 5% of all strokes): bleeding into the subarachnoid space (between the arachnoid and pia mater). The classic cause is rupture of an intracranial saccular ('berry') aneurysm — typically located at the bifurcations of the Circle of Willis (AComm-ACA junction, PCom-ICA junction, MCA bifurcation, basilar tip). SAH produces the classic 'thunderclap headache' — sudden onset of the worst headache of the patient's life — which is pathognomonic. SAH is dealt with in detail in neurosurgery; for this cluster, the emphasis is on distinguishing SAH from ICH and ischaemic stroke.
Classification of Stroke
Transient ischaemic attack (TIA) deserves special mention because it is a medical emergency in its own right. The risk of stroke after TIA is highest in the first 48 hours — approximately 10–15% within the first 2 days without treatment. The ABCD2 score (Age ≥60 [1]; BP ≥140/90 at presentation [1]; Clinical features — unilateral weakness [2] or speech disturbance without weakness [1]; Duration — ≥60 min [2] or 10–59 min [1]; Diabetes [1]) predicts short-term stroke risk after TIA. A score ≥4 indicates high risk and warrants immediate inpatient investigation and initiation of dual antiplatelet therapy.
Risk Factors and Pathogenesis of Stroke
The pathogenesis of stroke differs fundamentally between ischaemic and haemorrhagic subtypes, yet both share a common upstream driver — hypertension — which is the single most important and modifiable risk factor for stroke globally. Understanding both the genetic and acquired risk factors, and the pathogenic mechanisms they activate, is essential for designing appropriate secondary prevention strategies.
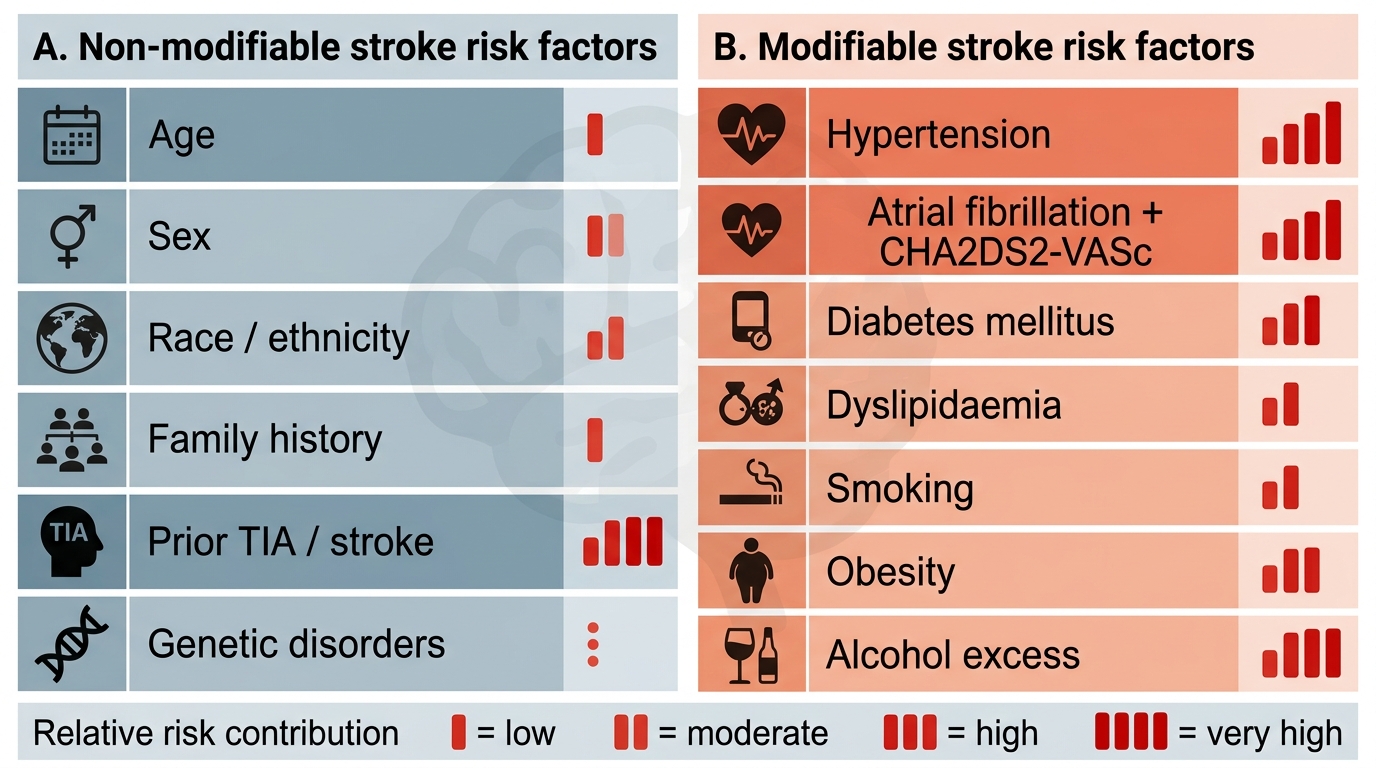
Non-modifiable risk factors include age (risk doubles for each decade over 55), sex (males have higher incidence, but females have higher lifetime risk due to longer life expectancy), race and ethnicity (higher incidence in South Asians and Africans compared to Europeans), family history of stroke (first-degree relative with stroke approximately doubles risk), and a prior personal history of stroke or TIA. Genetic risk factors include rare single-gene disorders — CADASIL (NOTCH3 mutation), MELAS (mitochondrial), Fabry disease (GLA mutation), sickle cell disease (HbS/HbS) — and more common polygenic contributions to hypertension, diabetes, and dyslipidaemia. Thrombophilias (Factor V Leiden, prothrombin gene mutation, protein C/S deficiency, antiphospholipid syndrome) increase the risk of ischaemic stroke particularly in young patients.
Modifiable risk factors — acquired — are the target of primary and secondary prevention:
- Hypertension (the single most important modifiable risk factor for both ischaemic and haemorrhagic stroke): chronic elevated blood pressure accelerates large-vessel atherosclerosis and drives small-vessel lipohyalinosis and microaneurysm formation. Even a 10 mmHg reduction in systolic blood pressure reduces stroke risk by approximately 30–40%. Blood pressure control is obligatory in all stroke survivors.
- Atrial fibrillation: the CHA₂DS₂-VASc score — Congestive heart failure (1), Hypertension (1), Age ≥75 (2), Diabetes (1), Stroke/TIA prior (2), Vascular disease (1), Age 65–74 (1), Sex category female (1) — determines anticoagulation need. A score ≥2 in males (≥3 in females) warrants oral anticoagulation (NOAC preferred over warfarin in non-valvular AF). The absolute stroke rate in untreated AF is approximately 5% per year.
- Diabetes mellitus: accelerates atherosclerosis, predisposes to lacunar infarction (via small vessel disease), and roughly doubles stroke risk. Glycaemic control reduces microvascular complications including stroke.
- Dyslipidaemia: elevated LDL-cholesterol drives large-vessel atherosclerosis and intracranial arterial atherosclerosis (particularly common in South and East Asians). High-intensity statins (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) are mandatory in ischaemic stroke secondary prevention, targeting LDL <70 mg/dL (or <55 mg/dL if very high risk).
- Smoking: directly damages endothelial cells, increases platelet aggregability, and accelerates large-vessel atherosclerosis. Risk returns to near baseline within 2–5 years of cessation.
- Obesity, physical inactivity, excessive alcohol consumption: each independently associated with elevated stroke risk, largely mediated through hypertension, diabetes, dyslipidaemia, and AF.
Stroke Risk Factors and Relative Contribution
Pathogenesis of ischaemic stroke — from vascular occlusion to neuronal death:
Once arterial occlusion occurs, the territory immediately downstream is deprived of oxygen and glucose. Within minutes, the core of the ischaemic region — the area of densest ischaemia where blood flow has fallen below 10–15 mL/100 g/min — undergoes irreversible neuronal death via glutamate-mediated excitotoxicity (massive calcium influx → mitochondrial failure → cell lysis). Surrounding the core is a zone of less severe ischaemia — the ischaemic penumbra — where blood flow is insufficient for normal function but above the threshold for immediate cell death. Penumbral tissue is electrically silent but metabolically viable; it can be salvaged if perfusion is restored within the therapeutic window. This penumbra-versus-core distinction is the biological rationale for thrombolysis and mechanical thrombectomy — both aim to restore flow before the penumbra is recruited into the infarct core. Penumbral tissue progressively dies over 6–12 hours; by 24 hours, it is largely gone. Hence the urgency: time is brain.
Pathogenesis of intracerebral haemorrhage — haematoma expansion, oedema, and herniation:
After vessel rupture, a haematoma forms; the initial haemostatic plug is imperfect, and haematoma expansion occurs in 30–40% of patients within the first few hours. Haematoma expansion is associated with early worsening and is one of the key targets of acute ICH management. The haematoma itself causes direct mechanical displacement and compression of surrounding structures; the perihematomal oedema that develops over 24–72 hours amplifies mass effect. If the haematoma is large enough, transtentorial or tonsillar herniation follows, which is the commonest mechanism of death in large ICH.
SELF-CHECK
A 58-year-old hypertensive patient presents with sudden-onset left-sided weakness — arm and face more affected than the leg — without sensory loss, visual disturbance, or aphasia. There is no history suggesting embolism. CT brain shows no haemorrhage. MRI DWI shows a small 12 mm spherical infarct in the right posterior limb of the internal capsule. Which TOAST subtype is most likely?
A. Large artery atherosclerosis
B. Cardioembolism
C. Small vessel occlusion (lacunar)
D. Stroke of other determined aetiology
Reveal Answer
Answer: C. Small vessel occlusion (lacunar)
The key features here are the small (<15 mm) spherical infarct in the deep perforating artery territory (posterior limb of internal capsule), the pure motor clinical pattern (no cortical signs), and the context of hypertension. These are the hallmarks of lacunar (small vessel) infarction caused by lipohyalinosis of a lenticulostriate perforating artery. Large artery atherosclerosis and cardioembolism produce larger, cortical or subcortical infarcts, often with cortical signs (aphasia, hemianopia). The absence of cortical features (aphasia, hemianopia, sensory loss) rules out large MCA territory occlusion. Lacunar infarcts in the internal capsule classically produce pure motor hemiplegia — one of the five classic lacunar syndromes.
SELF-CHECK
A 35-year-old woman presents with acute ischaemic stroke. She has no hypertension, diabetes, or AF. Her serum homocysteine is elevated, and she has a history of two previous deep vein thromboses. Lupus anticoagulant is positive on two occasions 12 weeks apart. Which category of stroke aetiology best fits this presentation?
A. Large artery atherosclerosis
B. Cardioembolism due to AF
C. Stroke of other determined aetiology — antiphospholipid syndrome
D. Cryptogenic stroke
Reveal Answer
Answer: C. Stroke of other determined aetiology — antiphospholipid syndrome
The combination of young age, prior DVT, positive lupus anticoagulant on two occasions 12 weeks apart, and elevated homocysteine all point to antiphospholipid syndrome (APS) — a hypercoagulable state that causes arterial and venous thrombosis and is a recognised 'other determined aetiology' in the TOAST classification. APS satisfies the Sapporo (Sydney) criteria: clinical (venous/arterial thrombosis or obstetric morbidity) + laboratory (lupus anticoagulant or anti-cardiolipin antibodies on ≥2 occasions ≥12 weeks apart). Cryptogenic applies when no cause is found after adequate investigation — this patient has a clear cause. Large artery atherosclerosis is unlikely at age 35 without traditional risk factors. AF is not mentioned.