Page 8 of 14
IM19.7-8 | Movement Disorder Investigation and Parkinson Therapy — SDL Guide (Part 2)
Management: Pharmacology of Antiparkinson Drugs
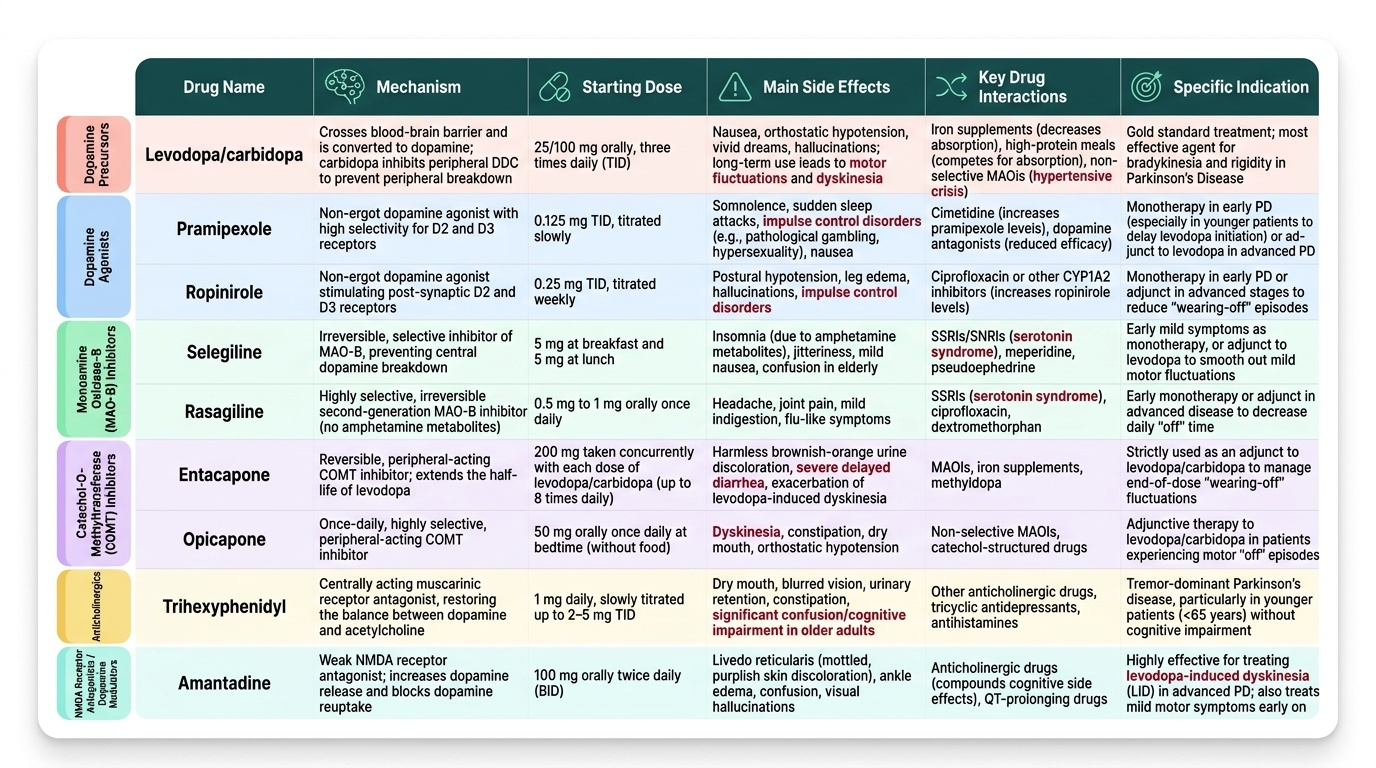
The pharmacotherapy of Parkinson's disease is built on restoring dopaminergic tone in the striatum through six major drug classes: levodopa, dopamine agonists, MAO-B inhibitors, COMT inhibitors, anticholinergics, and amantadine. Each class addresses the dopamine deficit through a distinct mechanism, has a distinct side-effect profile, and carries specific drug interactions that the prescribing clinician must know before initiating therapy. Understanding these pharmacological properties is the core of NMC IM19.8.
1. Levodopa + peripheral dopa-decarboxylase inhibitor (carbidopa or benserazide)
Mechanism: Levodopa (L-DOPA) is the metabolic precursor of dopamine, actively transported across the blood-brain barrier by the large neutral amino acid (LNAA) transporter, then converted to dopamine in the brain by aromatic amino acid decarboxylase (AAAD) in residual nigrostriatal terminals and striatal glia. The peripheral dopa-decarboxylase inhibitor (carbidopa in Sinemet; benserazide in Madopar) cannot cross the BBB and inhibits peripheral conversion of L-DOPA to dopamine OUTSIDE the brain — reducing peripheral dopamine side effects (nausea, vomiting, orthostatic hypotension), reducing the required L-DOPA dose by approximately 75%, and increasing the fraction reaching the brain. Standard formulations contain L-DOPA 100 mg + carbidopa 25 mg.
Starting dose: Levodopa/carbidopa 25/100 mg three times daily; titrate upward as needed based on motor response. Taking levodopa 30–60 minutes before protein-rich meals reduces competition with dietary amino acids for LNAA transport.
Long-term motor complications (the central clinical challenge of chronic levodopa therapy):
- Wearing-off (end-of-dose deterioration): parkinsonism returns predictably before the next dose as disease progresses and nigrostriatal buffering capacity is further depleted. Duration of benefit shortens from 4–6 hours initially to 2–3 hours after 3–5 years. Management: add COMT inhibitor (entacapone) or MAO-B inhibitor (rasagiline) to extend levodopa effect; increase dose frequency; controlled-release formulations.
- Peak-dose dyskinesias: involuntary choreiform movements occurring at peak plasma levodopa concentration (~60–90 min after dose), reflecting excessive striatal dopamine stimulation. Management: lower individual dose (if tolerated), add amantadine.
- On-off fluctuations: unpredictable, rapid oscillations between a mobile ON state and an immobile OFF state in advanced disease; managed with continuous drug delivery (subcutaneous apomorphine infusion, levodopa-carbidopa intestinal gel) or deep brain stimulation.
Key drug interactions:
- Non-selective MAO inhibitors (phenelzine, tranylcypromine, isocarboxazid): ABSOLUTE CONTRAINDICATION with levodopa — concurrent use causes hypertensive crisis from accumulation of dopamine. Note: selective MAO-B inhibitors (selegiline, rasagiline) are SAFE and are used therapeutically.
- Pyridoxine (Vitamin B6) in large doses: accelerates peripheral decarboxylation of L-DOPA, reducing brain delivery. This interaction is clinically relevant ONLY when L-DOPA is given WITHOUT carbidopa. With the combination preparation (L-DOPA + carbidopa), pyridoxine at standard supplementation doses does not significantly reduce brain L-DOPA delivery.
- Dietary large neutral amino acids (protein-rich meals): compete with L-DOPA for the intestinal and BBB LNAA transporter, reducing brain L-DOPA delivery. Patients with wearing-off should take levodopa 30–60 minutes before protein-rich meals.
- Antipsychotics (D2 blockers): reduce clinical effectiveness of levodopa. If antipsychotic therapy is needed in PD, use quetiapine or clozapine at low doses — the only antipsychotics with sufficiently low striatal D2 affinity that do not significantly worsen parkinsonism.
- Domperidone: safe peripheral antiemetic for levodopa-induced nausea (does not cross BBB). Avoid metoclopramide and prochlorperazine (central D2 blockers — worsen parkinsonism).
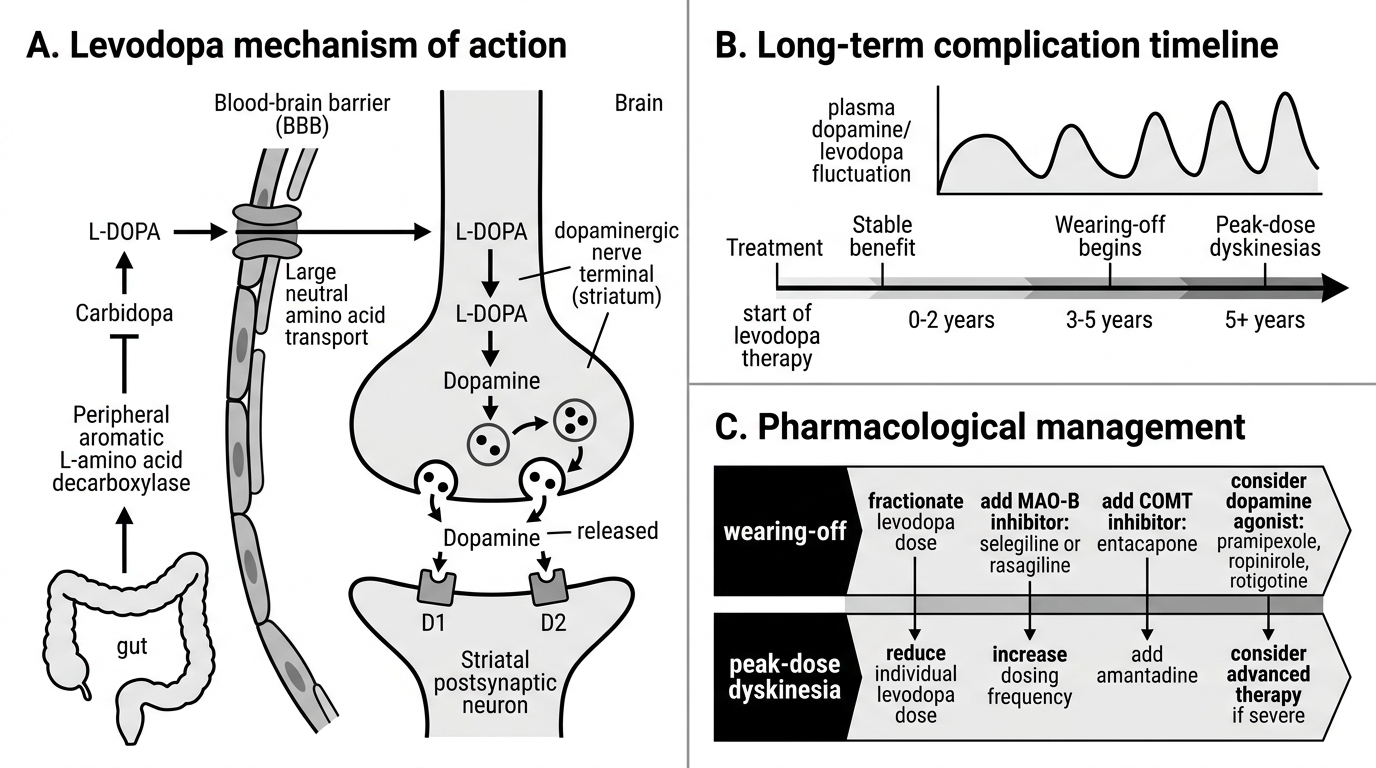
Levodopa Mechanism and Long-Term Complications
2. Dopamine agonists (DAs)
Examples: Non-ergot: pramipexole (oral, most common; 0.125 mg three times daily starting, titrate to 0.5–1.5 mg three times daily), ropinirole (oral; 0.25 mg three times daily starting), rotigotine (transdermal patch). Ergot-derived (avoid — fibrotic complications): cabergoline, bromocriptine.
Mechanism: Direct stimulation of postsynaptic D2/D3 dopamine receptors in the striatum, bypassing presynaptic conversion. Longer half-life than levodopa produces more sustained receptor stimulation and less wearing-off. Used as monotherapy in younger patients (<70) to delay levodopa initiation.
Side effects: Nausea, orthostatic hypotension (similar to levodopa), excessive daytime sleepiness and sudden sleep attacks (warn: do not drive until established as absent), impulse control disorders (gambling, hypersexuality, binge eating — a D3 mesolimbic class effect; ask at every clinic visit), hallucinations (more common than levodopa), ankle oedema, livedo reticularis.
3. MAO-B inhibitors (selegiline, rasagiline)
Mechanism: Selective inhibition of monoamine oxidase type B, the primary enzyme catabolising dopamine in the striatum, increasing intrasynaptic dopamine levels. Selective for MAO-B (not MAO-A) at therapeutic doses — do NOT cause the 'cheese effect' (tyramine hypertensive crisis) of non-selective MAOIs.
Dose: Selegiline 5–10 mg/day (take in the morning — metabolised to amphetamine, causes insomnia if taken later); rasagiline 1 mg/day.
Use: Monotherapy for mild early PD; adjunct to levodopa to reduce wearing-off.
Key interactions:
- Pethidine (meperidine): ABSOLUTE CONTRAINDICATION — fatal serotonin syndrome or excitatory crisis.
- Tramadol: serotonergic drug interaction — risk of serotonin syndrome; AVOID.
- SSRIs/SNRIs: risk of serotonin syndrome; caution; lowest risk with sertraline and citalopram.
- Non-selective MAOIs: additive MAO inhibition — do not combine.
4. COMT inhibitors (entacapone, opicapone)
Mechanism: Inhibit catechol-O-methyltransferase, an enzyme degrading levodopa and dopamine peripherally, extending levodopa plasma half-life by approximately 1.5–2 hours and increasing brain bioavailability. Only effective in COMBINATION with levodopa/carbidopa — no antiparkinsonian effect as monotherapy.
Dose: Entacapone 200 mg with each levodopa dose; opicapone 50 mg once daily at bedtime.
Side effects: Diarrhoea (may be severe, dose-limiting), orange/brownish discolouration of urine (harmless), exacerbation of levodopa side effects (reduce levodopa dose by 10–30% if dyskinesias emerge after adding entacapone). Tolcapone (earlier agent): hepatotoxicity — largely replaced by entacapone and opicapone.
5. Anticholinergics (trihexyphenidyl/benzhexol, procyclidine)
Mechanism: Block muscarinic M1 receptors in the striatum, correcting the relative excess of cholinergic over dopaminergic tone in parkinsonism caused by loss of the dopaminergic inhibition of tonically active cholinergic interneurons.
Dose: Trihexyphenidyl 2–6 mg/day in divided doses.
Specific uses in movement disorders: (a) Tremor-predominant PD in YOUNG patients only (<70 years) — preferential anti-tremor effect; (b) Acute drug-induced dystonic reaction — procyclidine or benztropine IM/IV gives rapid relief; (c) Sialorrhoea (drooling) in PD.
Side effects and contraindications: AVOID in patients over 70 years and in those with cognitive impairment — central anticholinergic syndrome (acute confusional state, hallucinations, delirium, memory impairment, potentially precipitating irreversible cognitive decline). Peripheral: dry mouth, urinary retention (men with BPH), constipation, blurred vision (mydriasis), tachycardia.
6. Amantadine
Mechanism: Multiple: weak dopamine releaser from presynaptic terminals; dopamine reuptake inhibitor; mild anticholinergic; most importantly, NMDA glutamate receptor antagonist (uncompetitive). The anti-glutamatergic mechanism is responsible for its primary current use: reducing levodopa-induced peak-dose dyskinesias by modulating striatal glutamatergic transmission from the subthalamic nucleus.
Dose: 100 mg twice daily (requires renal dose reduction in CKD — amantadine is renally cleared).
Clinical uses: (a) Early mild PD as monotherapy; (b) Adjunct for anti-dyskinesia — currently the best-evidenced oral agent for reducing peak-dose dyskinesias; (c) Drug-induced extrapyramidal side effects.
Side effects: Confusion and hallucinations (avoid in cognitively impaired), ankle oedema, livedo reticularis (mottled bluish-purple skin discolouration — benign, common, dose-dependent, reversible on discontinuation), urinary retention, nausea.
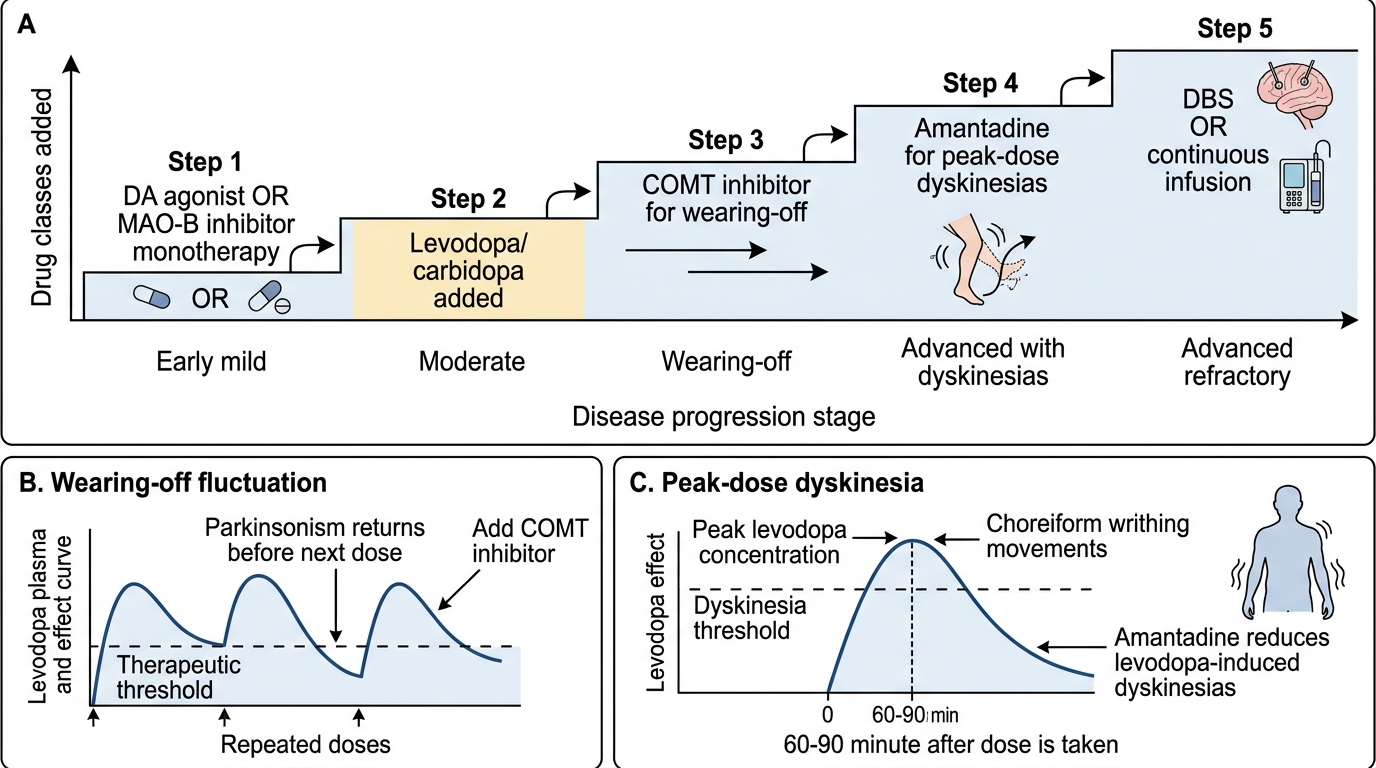
Parkinson Disease Pharmacotherapy Ladder
SELF-CHECK
A 68-year-old man with Parkinson's disease on levodopa/carbidopa 25/100 mg four times daily develops involuntary, writhing, dance-like movements of his arms and trunk approximately 90 minutes after each levodopa dose. The movements disappear after 2–3 hours. What is this complication, and which drug has the best evidence for reducing it?
A. Wearing-off — add a COMT inhibitor (entacapone) with each levodopa dose
B. Peak-dose dyskinesias — amantadine has the best evidence for reducing levodopa-induced dyskinesias
C. Biphasic dyskinesias — reduce the levodopa dose and switch to a dopamine agonist
D. On-off fluctuations — add a MAO-B inhibitor (rasagiline) to extend levodopa duration
Reveal Answer
Answer: B. Peak-dose dyskinesias — amantadine has the best evidence for reducing levodopa-induced dyskinesias
Peak-dose dyskinesias are involuntary choreiform or dystonic movements occurring at peak plasma levodopa concentrations, approximately 60–90 minutes after a dose — coinciding with maximum dopaminergic stimulation. They are distinct from wearing-off (parkinsonism returning BEFORE the next dose) and on-off fluctuations (rapid, unpredictable transitions). Amantadine, via NMDA glutamate receptor antagonism, has the best evidence among oral agents for reducing peak-dose dyskinesias. COMT inhibitors extend the duration of levodopa effect (useful for wearing-off) but do not reduce peak-dose dyskinesias and may worsen them. Reducing levodopa dose can reduce dyskinesias but may worsen parkinsonism.
Self-Assessment: Integrating Imaging and Pharmacotherapy
At this stage you have covered both core competency areas of this SDL: the selection and interpretation of diagnostic imaging modalities for movement disorders (IM19.7) and the pharmacology of the major antiparkinson drugs with their doses, side effects, and interactions (IM19.8). The self-assessment scenarios below integrate these two competency areas into clinical case formats that mirror the style of NMC clinical examinations. For each scenario, identify the correct investigation, interpret the expected result, and determine the appropriate pharmacotherapeutic response before reading the analysis. This clinical synthesis — moving from diagnostic question to investigation selection to drug choice — is the integrated skill this SDL prepares you for. The ability to draw on both imaging knowledge and pharmacology simultaneously in a single patient encounter reflects the NMC KH-level expectation for IM19.8 and the SH-level expectation for IM19.7.
Provided image
Scenario A: Mr Venkataraman, now confirmed to have idiopathic PD by clinical diagnosis, is started on levodopa/carbidopa 25/100 mg three times daily. After 5 years of good control, he notices that his parkinsonism returns about 2 hours after each dose, before the next one is due. His wife also notes he has started to have involuntary writhing movements of his arms 1 hour after the midday dose. What are these two phenomena and what pharmacological interventions address each?
Analysis: Two distinct levodopa motor complications:
1. Wearing-off: parkinsonism returning BEFORE the next dose — caused by progressive loss of nigrostriatal dopaminergic buffering capacity and short levodopa half-life. Options: add entacapone 200 mg with each dose (COMT inhibitor, extends levodopa half-life); add rasagiline 1 mg/day (MAO-B inhibitor, reduces dopamine breakdown); increase dose frequency; extended-release formulation.
2. Peak-dose dyskinesias: involuntary movements at peak plasma levodopa — too much dopamine at the striatum. Option: add amantadine 100 mg twice daily (NMDA antagonist, reduces dyskinesias without worsening motor symptoms). Consider modest reduction in individual levodopa dose. Advanced refractory: deep brain stimulation of STN or GPi.
Scenario B: A 55-year-old woman with schizophrenia on risperidone develops symmetric bilateral rest tremor and bradykinesia. DAT-SPECT shows normal bilateral comma-shaped striatal uptake symmetrically. Risperidone is switched to quetiapine. Three months later, her tremor and bradykinesia resolve completely. What does the normal DAT-SPECT confirm, and why was quetiapine preferred?
Analysis: Normal DAT-SPECT confirms drug-induced parkinsonism (DIP) — intact presynaptic dopaminergic terminals; postsynaptic D2 receptor was being blocked by risperidone, preventing dopaminergic signalling. Resolution on switching confirms drug causation. Quetiapine was chosen because it has the lowest striatal D2 receptor binding affinity at clinical doses (along with clozapine), and does not significantly block the nigrostriatal D2 receptors. Risperidone, haloperidol, and olanzapine have high striatal D2 affinity and should be avoided in patients at risk for DIP or those with PD requiring antipsychotic therapy.
Scenario C: A 62-year-old man with PD well-controlled on levodopa/carbidopa and rasagiline is prescribed tramadol by an orthopaedic surgeon for back pain. Within 2 hours of the first tramadol dose, he develops diaphoresis, hyperthermia, confusion, and myoclonus. What is the diagnosis and mechanism?
Analysis: Serotonin syndrome — caused by the interaction between rasagiline (selective MAO-B inhibitor with some serotonin-related effects) and tramadol (serotonin-norepinephrine reuptake inhibitor with weak opioid activity). Tramadol inhibits serotonin reuptake; the combination with a MAO inhibitor leads to excess serotonergic neurotransmission. The clinical triad of serotonin syndrome: mental status change (confusion, agitation), autonomic instability (hyperthermia, diaphoresis, tachycardia), and neuromuscular abnormality (clonus, myoclonus, hyperreflexia). Treatment: stop both drugs, supportive care, cyproheptadine (5-HT2A antagonist) for moderate-severe cases, benzodiazepines for agitation. Prevention: this interaction must be flagged for ANY PD patient on rasagiline or selegiline before prescribing tramadol, pethidine, linezolid, or SSRIs/SNRIs.
CLINICAL PEARL
The two most dangerous drug interactions in Parkinson's disease pharmacotherapy that every clinician must know before entering clinical practice are:
- Levodopa + non-selective MAOI (phenelzine, tranylcypromine): ABSOLUTE CONTRAINDICATION. Causes hypertensive crisis from peripheral and central accumulation of dopamine and noradrenaline. This interaction is avoidable — check for any MAOI in the drug history before starting levodopa. Selective MAO-B inhibitors (selegiline, rasagiline) are SAFE with levodopa.
- MAO-B inhibitor (rasagiline/selegiline) + pethidine (meperidine): ABSOLUTE CONTRAINDICATION — risk of fatal serotonin syndrome or excitatory crisis. Tramadol and SSRIs/SNRIs carry significant caution with MAO-B inhibitors and should be avoided or used under specialist guidance only.
In addition, remember the anticholinergic rule: NEVER prescribe trihexyphenidyl or other anticholinergics for tremor in a patient over 70 years of age or in any patient with cognitive impairment — the central anticholinergic side effects (acute confusional state, hallucinations, delirium) can be severe, may be irreversible, and are entirely avoidable.