Page 15 of 24
IM2.{17,21-22,24} | ACS Resuscitation and Rehabilitation — SDL Guide (Part 2)
Cardiac Rehabilitation: Structure, Components, and Evidence
Cardiac rehabilitation (CR) is an evidence-based, multidisciplinary programme designed to optimise physical, psychological, and social recovery after a cardiac event and to reduce the risk of recurrent events through structured exercise, risk factor modification, patient education, and psychosocial support. Despite strong evidence of benefit, CR remains severely underutilised in India — only an estimated 3–5% of eligible post-MI patients in India access formal CR — making CR education and discharge counselling by attending physicians, trainees, and medical students critically important as partial substitutes.
Evidence base for cardiac rehabilitation:
The 2016 Cochrane review of 63 randomised trials (14,486 patients) of exercise-based CR demonstrated: 26% reduction in cardiovascular mortality, 18% reduction in hospital readmissions, and significant improvements in quality of life and exercise capacity compared to usual care. The 2019 ACC/AHA guidelines give CR a Class I recommendation (Level A evidence) for all post-ACS patients and a Class I recommendation for patients with stable angina and heart failure. The mechanism of benefit is multi-factorial: exercise training improves endothelial function, increases HDL, reduces LDL and blood pressure, improves insulin sensitivity, promotes weight loss, and reduces sympathetic activation. Psychosocial support addresses the high prevalence of depression after MI (occurs in ~20–30% of post-MI patients and independently doubles one-year mortality).
Components of a structured CR programme:
Phase I (Inpatient, hospital phase — days 1–7 post-MI):
Goal: early mobilisation, patient education, risk factor identification, discharge planning. Key activities: sitting up at bedside on day 2–3, standing with assistance on day 3–4, ward ambulation by day 5–6 (if no haemodynamic instability or mechanical complication), stair climbing before discharge. Education: explanation of the disease, medications and their purpose, warning symptoms requiring urgent return to hospital, and initial dietary counselling. Psychosocial screening: PHQ-2/PHQ-9 for depression, GAD-7 for anxiety.
Phase II (Outpatient, supervised exercise — weeks 2–12 post-event):
Goal: supervised exercise training with physiological monitoring, intensive risk factor management, patient education programme, psychosocial counselling. Setting: hospital-based CR centre or community health centre with cardiac monitoring capability. Frequency: 2–3 supervised sessions/week for 8–12 weeks. Exercise prescription (FITT principle): Frequency 3–5 times/week; Intensity 50–80% of peak heart rate reserve (determined by baseline symptom-limited exercise test) or RPE (Borg scale 12–14); Type: aerobic exercise (walking, cycling, swimming); Time: 20–45 minutes per session, building gradually. Resistance training (light weights, 2–3 times/week) added after 4 weeks. Contraindications to exercise testing/training: decompensated HF, unstable angina, severe symptomatic aortic stenosis, uncontrolled arrhythmia, SBP >200 mmHg, recent PE or DVT.
Phase III (Maintenance, long-term — beyond 12 weeks):
Goal: sustain gains from phase II, maintain lifestyle changes independently. Most patients transition to unsupervised home or community exercise. The challenge in India: the majority of post-MI patients never reach Phase II CR (limited centres, distance, cost, cultural factors). Home-based CR programmes (telephone-supported, app-based, or community health worker-delivered) have been shown to produce equivalent outcomes to centre-based CR and are particularly relevant for the Indian population.
Risk factor modification counselling (the key discharge conversation):
- Smoking cessation: most important single lifestyle intervention — cessation reduces CAD risk by 50% within 1 year; approach: brief intervention (5 As — Ask, Advise, Assess, Assist, Arrange), nicotine replacement therapy (NRT — patch + lozenge/gum), or varenicline (first-line pharmacotherapy — doubles quit rate at 1 year; safe post-ACS per EAGLES trial)
- Diet: Mediterranean diet or DASH dietary pattern; reduce saturated fat (<7% total calories), eliminate trans-fats; increase omega-3 (oily fish, walnuts, flaxseed); increase fibre (fruits, vegetables, whole grains); restrict sodium (<2 g/day if HF or hypertension)
- Physical activity: return to light activity at 2 weeks post-discharge (walking); moderate-intensity aerobic exercise (150 min/week) by 4–6 weeks; sexual activity resumption safe at 4–6 weeks if able to climb 2 flights of stairs without angina; driving: resume after 4 weeks (ACS event) or 1 week (after elective PCI) if no haemodynamic complication
- Weight management: BMI target 18.5–24.9 kg/m²; waist circumference <90 cm (Indian men), <80 cm (Indian women); even 5–10% body weight loss significantly improves lipid profile, blood pressure, and insulin resistance
- Alcohol: recommended ≤14 units/week (men), ≤7 units/week (women) for secondary prevention; encourage reduction or abstinence in patients with hypertension, AF, or HF
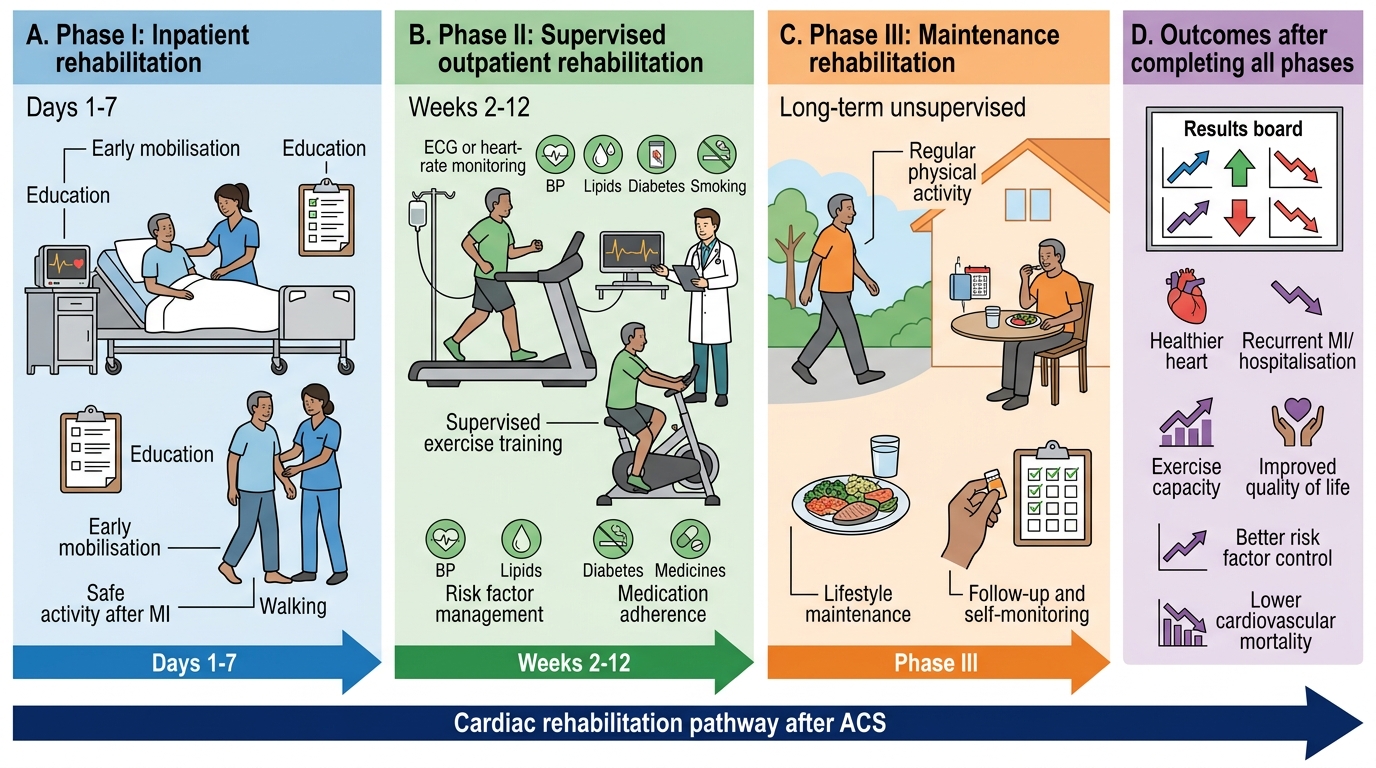
Three Phases of Cardiac Rehabilitation After ACS
Applied Practice: Patient Counselling After ACS
The NMC competency IM2.24 requires the ability to counsel and communicate with patients with empathy about lifestyle after ACS. Effective post-ACS counselling is a clinical skill — not merely a recitation of facts — that requires the ability to assess the patient's readiness to change, tailor the message to their understanding and life circumstances, address emotional responses (fear, denial, depression), and motivate sustained behaviour change through a patient-centred conversation rather than a one-way lecture.
Principles of effective post-ACS counselling:
Empathic opening and emotional validation: Many post-MI patients experience significant fear, depression, and uncertainty in the first days after their event. A counselling session that begins with 'You need to stop smoking and lose weight' will be received defensively by a patient who is still processing the existential impact of 'I nearly died.' Begin with: 'How are you feeling about what has happened? What questions or worries do you have?' This opens the dialogue and establishes trust before clinical recommendations are made.
Addressing common patient questions (the 5 most frequent post-MI questions in India):
1. 'When can I go back to work?' — Light office work: 2–4 weeks (desk job, no physical exertion); physical labour: 6–8 weeks (clearance after stress test); driving: 4 weeks (private vehicle); commercial driving: requires medical clearance and may be permanently restricted after complex MI.
2. 'Can I have sex again?' — Sexual activity resumes at 4–6 weeks when the patient can walk briskly or climb two flights of stairs without chest pain, breathlessness, or undue fatigue. The cardiac workload of sexual activity is equivalent to moderate-intensity exercise (~5 METs). PDE5 inhibitors (sildenafil) are contraindicated with nitrates — discuss this explicitly if the patient is prescribed nitrates.
3. 'Do I have to take all these tablets for the rest of my life?' — Explain the rationale for each drug: aspirin prevents clot formation on the stent; ticagrelor/clopidogrel prevents stent thrombosis (must not stop for ≥12 months without cardiologist advice — sudden discontinuation causes acute stent thrombosis); statin reduces plaque progression; beta-blocker protects the heart after the attack; ACE inhibitor helps the heart recover. Medication literacy and adherence are the strongest predictors of post-MI outcomes in India.
4. 'Will this happen again?' — Be honest but hopeful: 'The risk of another heart attack is significantly higher than in someone who has never had one. But taking these medications, stopping smoking, exercising regularly, and controlling your diabetes/blood pressure reduces that risk substantially. Cardiac rehabilitation will help you recover safely.'
5. 'What should I eat?' — Practical guidance: reduce fried foods, use healthier cooking oils (rice bran, olive oil, mustard oil), increase vegetables and dal, reduce red meat and processed foods, reduce salt if hypertensive. Cultural dietary nuance matters: vegetarian patients in India can achieve Mediterranean-pattern diet easily; the main challenge is often hidden sugar and refined carbohydrate in traditional diets.
Motivational interviewing (MI) principles are the evidence-based framework for behaviour change counselling in chronic disease:
- Open questions ('What would you need to feel confident about stopping smoking?') rather than closed questions ('Have you stopped smoking?')
- Reflective listening (repeat back what the patient says to confirm understanding and validate their experience)
- Affirm positive steps already taken
- Explore discrepancy between current behaviour and stated health goals ('You mentioned wanting to see your grandchildren grow up — how does smoking fit with that goal?')
- Roll with resistance — if the patient is ambivalent, do not argue; explore their ambivalence non-judgementally
Family engagement is particularly important in the Indian context: family members are frequently the primary drivers of medication adherence, dietary change, and smoke-free household maintenance. Include the spouse or primary family caregiver in the counselling session where possible.
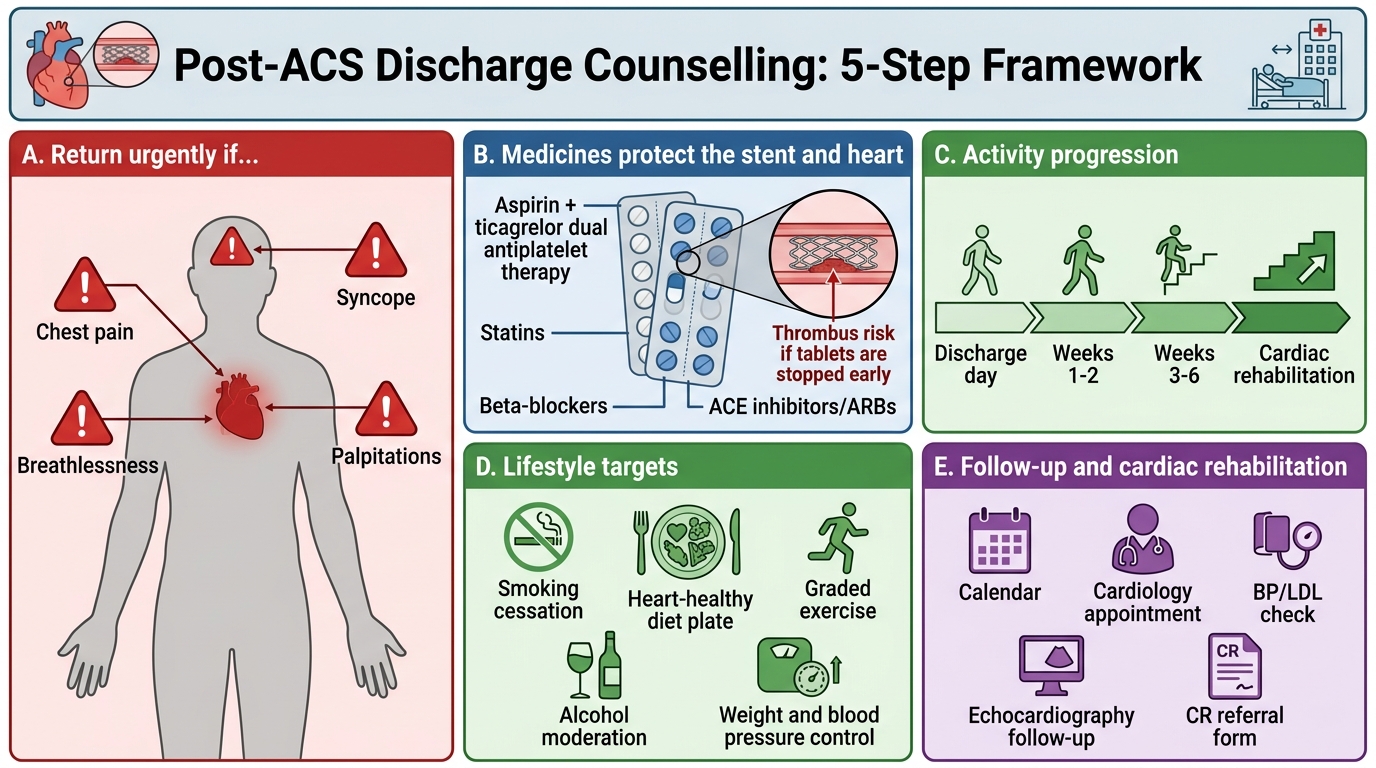
Post-ACS Discharge Counselling Framework
SELF-CHECK
A 55-year-old post-STEMI patient (anterior MI, primary PCI 5 days ago, LVEF 42%) is about to be discharged. He is a smoker (30 pack-years), overweight (BMI 29), and mildly hypertensive. He asks about his ticagrelor tablet: 'My friend told me I can stop it after 3 months because the stent will be fully healed.' What is the CORRECT response?
A. Your friend is correct — ticagrelor can be stopped after 3 months if the stent is drug-eluting; aspirin alone is sufficient
B. The minimum recommended duration of dual antiplatelet therapy (aspirin + ticagrelor) after ACS with stenting is 12 months; early discontinuation risks acute stent thrombosis, which is a life-threatening emergency
C. Ticagrelor can be replaced with aspirin alone after 6 months if your LDL is well controlled on a statin
D. You should switch from ticagrelor to clopidogrel after 3 months — it is safer for long-term use
Reveal Answer
Answer: B. The minimum recommended duration of dual antiplatelet therapy (aspirin + ticagrelor) after ACS with stenting is 12 months; early discontinuation risks acute stent thrombosis, which is a life-threatening emergency
Dual antiplatelet therapy (DAPT) with aspirin plus ticagrelor (or clopidogrel) must be continued for a minimum of 12 months after ACS and PCI with drug-eluting stent insertion. Premature DAPT discontinuation — even for a single missed dose — is associated with a significant risk of acute in-stent thrombosis, which presents as sudden STEMI and carries a 15–45% mortality rate. The healing of the stent's drug-eluting polymer coating requires 12 months before the in-stent thrombosis risk drops sufficiently to allow DAPT cessation. Reducing to aspirin monotherapy before 12 months without explicit cardiologist instruction is contraindicated. The duration may be extended to 24–36 months in high-ischaemic-risk patients, or shortened to 3–6 months only in very high bleeding risk (PRECISE-DAPT score ≥25), always by the treating cardiologist.
Self-Assessment: BLS, ACLS, and CR Integration
This self-assessment covers the three competency areas of this module — BLS technique, ACLS decision-making, and cardiac rehabilitation counselling — through structured scenarios and critical thinking prompts. Work through each before reading the analysis. The BLS and ACLS scenarios test applied procedural reasoning rather than protocol recall; the CR scenario tests the ability to individualise a rehabilitation plan and conduct a patient-centred counselling conversation. Together they represent the full scope of IM2.17, IM2.21, IM2.22, and IM2.24 at the level of final-year clinical competence.
Scenario A (BLS technique): While doing ward rounds, you witness a 65-year-old patient suddenly collapse in the corridor outside the ward. You find him unresponsive with no breathing and no palpable carotid pulse. The crash trolley with defibrillator is two minutes away. You are alone. What are your immediate first five actions, and what are the two most common CPR technique errors you will deliberately avoid?
Analysis: (1) Confirm safety (no hazard). (2) Check responsiveness — tap shoulders firmly, shout. (3) Shout loudly for help and direct a specific person to call emergency code and bring the crash trolley. (4) Position the patient supine on the corridor floor (firm surface). (5) Begin chest compressions immediately: heel of hand on lower sternum, depth 5–6 cm, rate 100–120/min, complete recoil. Do NOT leave the patient to get the defibrillator yourself — someone else must do this while you maintain compressions. If alone with no help, call emergency services with your phone on speaker while beginning compressions. Two most common errors to avoid: (a) inadequate compression depth (<5 cm) — arm fatigue causes depth to drop; lock elbows and use body weight, not arm strength; (b) leaning on the chest between compressions — incomplete recoil reduces venous return by 30–40%; fully release after every compression.
Scenario B (ACLS decision-making): A 72-year-old woman in the CCU 36 hours after an inferior STEMI (successfully thrombolysed) develops sudden haemodynamic collapse. Monitor shows a regular wide-complex tachycardia at 160 bpm. BP is 70/40 mmHg. She is drowsy but responds to voice. No IV access is currently in place. What rhythm is this, and what is the ACLS management?
Analysis: Regular wide-complex tachycardia in the context of acute MI with haemodynamic compromise = sustained ventricular tachycardia (VT) until proven otherwise. Management: (a) this is haemodynamically unstable VT → do NOT wait to establish IV access for drug therapy; perform synchronised DC cardioversion immediately (120–200 J biphasic; synchronised mode to avoid delivering shock on T-wave which would cause VF). If IV access obtained rapidly in parallel, IV amiodarone 150 mg over 10 minutes may be given for pharmacological conversion if there is a brief delay in charging, but synchronised cardioversion is the definitive treatment. (b) After successful cardioversion: IV amiodarone infusion (900 mg over 24 hours) for VT suppression; correct electrolytes (K+ target 4.0–4.5 mmol/L, Mg2+ target ≥0.8 mmol/L); assess for ischaemia and reperfusion status.
Scenario C (CR counselling): A 48-year-old construction worker with anterior STEMI (primary PCI 5 days ago, LVEF 48%), heavy smoker (40 pack-years), BMI 32, and type 2 diabetes presents for discharge counselling. He is anxious about losing his income if he cannot return to work quickly. Outline the key elements of your discharge counselling and CR plan, with culturally sensitive recommendations.
Analysis: Empathic opening: acknowledge the financial concern directly ('I understand your worry about work — let's make a clear plan so you know exactly when you can safely return'). Activity plan: light indoor work in 3–4 weeks; physical construction labour at 8–10 weeks after symptom-limited exercise test confirms adequate exercise capacity. Smoking: address directly but empathically — 'The single most important thing you can do to prevent another heart attack is stop smoking. I can prescribe varenicline which doubles your chance of success.' Diabetes: explain the link between poor glycaemic control and repeat MI; optimise HbA1c to <7%. Medications: review each drug (aspirin, ticagrelor, statin, ACE inhibitor, beta-blocker — explaining why each is essential). CR referral: if hospital-based CR not available locally, provide written home exercise programme (walking 20–30 min daily, increasing gradually) and dietary advice sheet in regional language. Follow-up: 2 weeks with GP, 4–6 weeks with cardiologist; echo at 6–8 weeks to recheck LVEF (if LVEF <40%, ICD implantation may be indicated).
CLINICAL PEARL
The most common cause of CPR failure in in-hospital cardiac arrest is insufficient compression depth — not insufficient rate. Compression depth of <4 cm generates minimal forward blood flow. Rescuers in real arrests consistently underestimate their compression depth. Use the full weight of your body (not just arm strength) and lock your elbows; many hospitals now use feedback devices on mannequins that beep when depth is adequate. The second most common failure is the 'I'll stop compressions for a moment to give drugs' error — never interrupt compressions for drug preparation; the drug is given during the 2-minute CPR cycle, not during a pause.
For cardiac rehabilitation: in India, the 'will this medication cause addiction?' concern about beta-blockers and the belief that 'once the stent is in, the heart is fixed and no further treatment is needed' are the two most common barriers to post-MI medication adherence. Address both directly in the discharge counselling: beta-blockers are not addictive or sedating; and the stent only treated one blocked vessel — the underlying atherosclerotic process in all other coronary arteries continues to need medical therapy.