Page 14 of 20
IM21.9 | Bee Sting and Other Envenomation — SDL Guide (Part 2)
Management Principles: Stabilisation and Specific Treatments
Across all envenomation types covered in this module, three management principles apply universally and form a mental framework for the first minutes of any encounter. First, identify the mechanism — IgE-mediated anaphylaxis requires adrenaline IM as the only life-saving first-line treatment, while direct toxic envenomation (massive stings, haemolysis, organ injury) requires supportive intensive care and aggressive fluid replacement. Second, remove the source — extract bee stingers by scraping (not pinching), pick off jellyfish tentacles without rubbing, leave snake fangs/stingers if embedded deeply and plan surgical removal under anaesthesia if needed. Third, treat the complication, not just the acute event — monitor for AKI in massive envenomation, biphasic anaphylaxis in single sting cases, and late serum sickness in antivenom recipients. Applying these three principles within the first five minutes converts a chaotic emergency encounter into a structured management sequence.
Provided image
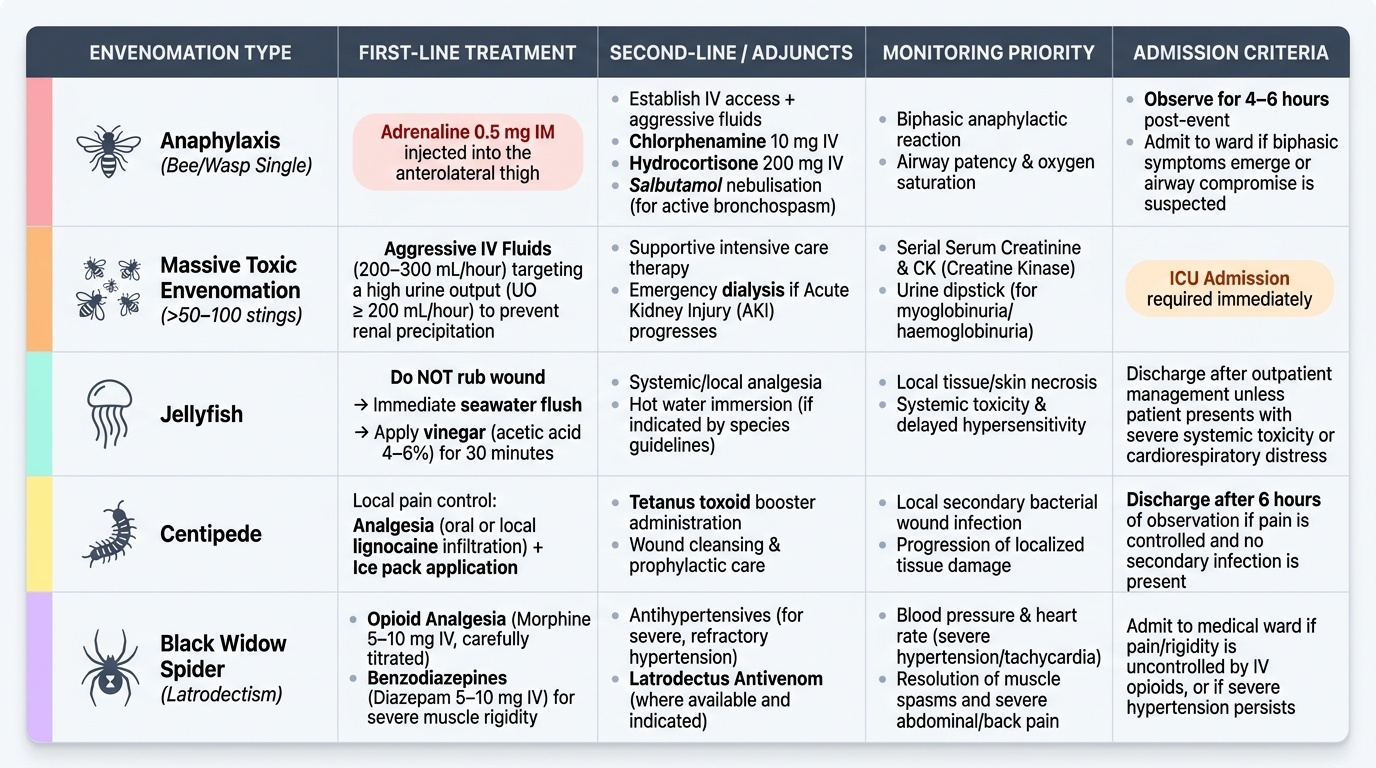
For anaphylaxis from any cause (bee, wasp, jellyfish, antivenom): adrenaline 0.5 mg IM anterolateral thigh → IV access + fluids → adjuncts (chlorphenamine 10 mg IV, hydrocortisone 200 mg IV) → salbutamol nebulisation for bronchospasm → observe 4–6 hours for biphasic reaction.
For massive envenomation with organ toxicity (>50–100 bee stings, any species): IV fluids 200–300 mL/hour targeting UO ≥200 mL/hour → serial creatinine, CK, urine dipstick → ICU admission → dialysis if AKI progresses.
For jellyfish: do not rub → seawater flush → vinegar 30 min → analgesia.
For centipede: analgesia (oral or local lignocaine) + ice + tetanus toxoid + 6 hours observation.
For black widow spider (latrodectism): opioid analgesia (morphine 5–10 mg IV titrated) + benzodiazepine (diazepam 5–10 mg IV) for muscle rigidity + antihypertensive for severe hypertension + antivenom where available.
Self-Assessment: Integrated Envenomation Management
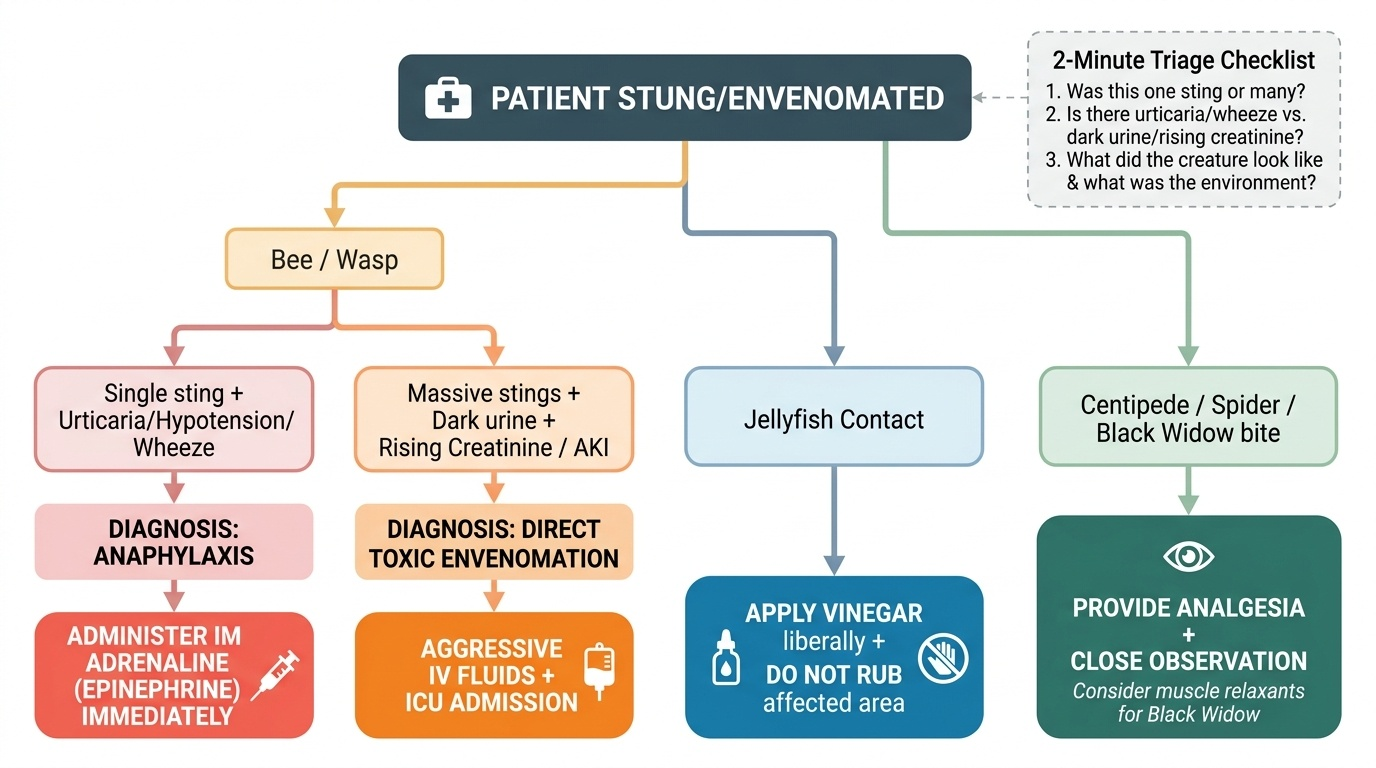
The self-assessment scenarios below consolidate the key diagnostic and management principles across the spectrum of envenomation covered by IM21.9. The unifying clinical skill is rapid syndrome recognition — identifying within the first two minutes of assessment whether the patient has anaphylaxis (single sting, sensitised, requires adrenaline immediately), direct toxic envenomation (massive stings, unsensitised, requires supportive care and aggressive fluids), or a specific arthropod presentation (jellyfish requiring vinegar, centipede requiring analgesia, black widow requiring muscle relaxants). The scenarios below are designed to train this rapid pattern-recognition across the range of common presentations that an Indian physician in any practice setting may encounter. Work through each scenario independently before reading the analysis. The key differentiating questions are always the same: Was this one sting or many? Is there urticaria and wheeze (anaphylaxis) or dark urine and rising creatinine (toxic)? What did the creature look like and what environment did the patient come from? Systematic application of these three questions within the first two minutes of any envenomation encounter will direct you to the correct treatment before investigation results are available.
Provided image
Scenario A: A 45-year-old beekeeper is brought in after being stung approximately 300 times when a swarm attacked him. He has no history of allergy. He is conscious but distressed, has diffuse oedema, and his urine is dark red-brown. Serum creatinine is 2.8 mg/dL on admission. There is no urticaria or wheeze. What is the primary threat and immediate management priority?
Analysis: Massive toxic envenomation — NOT anaphylaxis (no urticaria, no wheeze, no history of allergy). Primary threat: pigment nephropathy (haemoglobinuria + myoglobinuria) leading to AKI. Immediate priority: aggressive IV fluid hydration (normal saline at 200–300 mL/hour) to achieve urine output ≥200 mL/hour and flush pigment casts. Serial creatinine, urine dipstick, CK, LDH monitoring. ICU admission. No role for adrenaline — this is direct toxicity, not anaphylaxis.
Scenario B: A 28-year-old tourist in Goa develops immediate burning pain and linear erythematous tracks on the thigh after swimming. She comes to the beach clinic in distress. The marks are branching and there are gelatinous fragments attached to the skin. What is the correct sequence of first aid?
Analysis: Jellyfish envenomation. Correct sequence: (1) do NOT rub; (2) pick off gelatinous tentacle fragments with a card-edge or tweezers; (3) flush with seawater (NOT fresh water); (4) apply 5% vinegar for 30 minutes; (5) analgesia (paracetamol or tramadol); (6) observe for systemic features. If anaphylaxis develops (urticaria, hypotension): adrenaline 0.5 mg IM.
SELF-CHECK
A 60-year-old man presents with severe abdominal cramps, muscle rigidity, and diaphoresis after what he describes as a 'small spider bite' on the leg 3 hours ago. There is no visible wound necrosis. BP is 180/110 mmHg and HR is 120/min. This presentation is most consistent with:
A. Brown recluse spider bite causing dermonecrotic toxin reaction
B. Black widow spider (latrodectism) — systemic neurotoxin causing catecholamine release, muscle spasm, and autonomic storm
C. Giant centipede bite causing systemic haemolysis
D. Bee sting anaphylaxis presenting atypically with abdominal pain
Reveal Answer
Answer: B. Black widow spider (latrodectism) — systemic neurotoxin causing catecholamine release, muscle spasm, and autonomic storm
Latrodectism (black widow spider envenomation) presents with severe abdominal cramps and muscle rigidity that classically mimic an acute abdomen, along with diaphoresis, hypertension, and tachycardia — caused by the spider's alpha-latrotoxin triggering massive neurotransmitter release (catecholamines and acetylcholine). Brown recluse spider causes local necrosis (dermonecrosis) with minimal systemic effects initially. Centipede bite causes local pain and rarely systemic features. Bee sting anaphylaxis causes urticaria and bronchospasm — not abdominal cramps and muscle rigidity. Management of latrodectism: opioid analgesia, benzodiazepines for spasm, antihypertensives, and antivenom where available.
CLINICAL PEARL
The most important clinical distinction in bee sting management is: single sting plus urticaria/hypotension/wheeze = anaphylaxis = adrenaline IM immediately; multiple (>50) stings plus dark urine plus no urticaria = toxic massive envenomation = aggressive IV fluids and organ monitoring. These two patients look superficially similar (both critically ill after bee stings) but need entirely different treatments, and confusing them leads to giving adrenaline where it is not needed (toxic envenomation) or withholding adrenaline where it saves life (anaphylaxis).
For jellyfish: the single most important 'do not' is do not rub, do not use fresh water. Rubbing and fresh water trigger nematocyst discharge and transform a manageable local sting into an extensively envenomated surface. Vinegar (acetic acid) and seawater are the correct topical agents. Teach this to every nurse and healthcare worker in any coastal posting — they encounter jellyfish stings far more often than the doctor does.