Page 8 of 20
IM21.7 | Snake Bite Antivenom Therapy — SDL Guide (Part 2)
Adverse Reactions: Recognition and Management
Adverse reactions to antivenom are common — early reactions occur in 20–80% of patients in various series from India and South Asia, depending on the formulation and infusion rate. The majority are mild to moderate anaphylactoid reactions rather than true IgE-mediated anaphylaxis, because most patients have not been previously sensitised. However, the clinical presentation of severe anaphylactoid reaction is indistinguishable from anaphylaxis and must be treated identically. The fear of adverse reactions should never be a reason to withhold antivenom from a patient with systemic envenomation — antivenom-related deaths are exceptionally rare when managed correctly, while untreated systemic envenomation carries a high mortality. The clinician's role is to anticipate, monitor, and manage reactions promptly.
Provided image
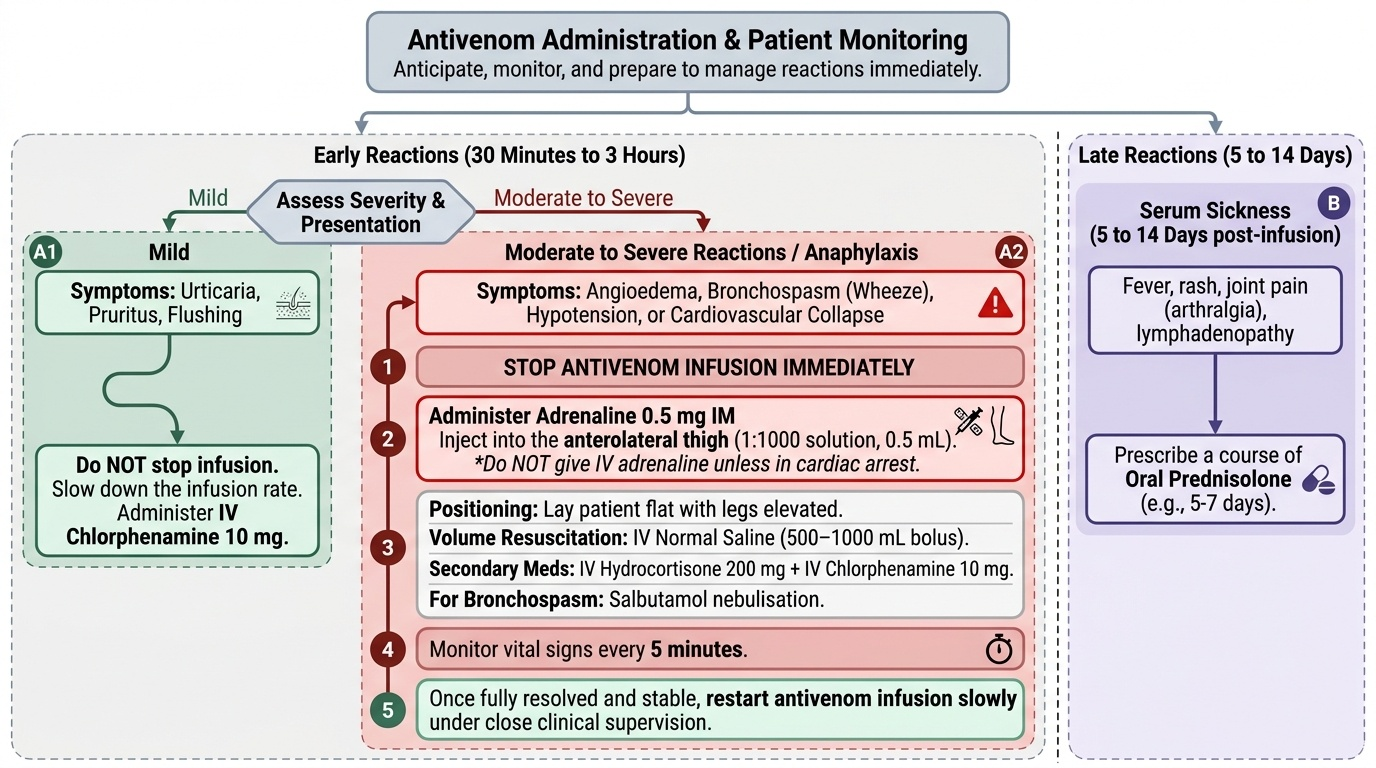
Early reactions (within 30 minutes to 3 hours of starting infusion):
These are the most common and clinically important reactions. They result from complement activation by the aggregated equine IgG protein (anaphylactoid mechanism) or from true IgE-mediated sensitisation in previously exposed patients. Clinical presentations range from mild to severe:
- Urticaria, pruritus, flushing: Mild cutaneous reactions; do not require stopping the infusion — slow the rate and administer IV chlorphenamine 10 mg.
- Angioedema: Swelling of the face, lips, tongue, or throat; stop the infusion and treat as for anaphylaxis if airway involvement occurs.
- Bronchospasm (wheeze): Stop the infusion immediately. Administer adrenaline 0.5 mg IM into the anterolateral thigh (1:1000 solution, 0.5 mL). Salbutamol nebulisation for bronchospasm. Do NOT give adrenaline IV unless the patient is in cardiac arrest — IV adrenaline carries risk of fatal arrhythmia.
- Hypotension and cardiovascular collapse (anaphylaxis): Stop the infusion. Adrenaline 0.5 mg IM (1:1000, 0.5 mL) into the anterolateral thigh is the first and most important action — do this before calling for help, before IV antihistamines, before anything else. Lay the patient flat with legs elevated. IV normal saline 500–1000 mL bolus for haemodynamic resuscitation. IV hydrocortisone 200 mg (onset delayed 4–6 hours but prevents biphasic reactions). IV chlorphenamine 10 mg (adjunct). Monitor every 5 minutes.
Management summary for anaphylaxis from antivenom:
1. Stop antivenom infusion immediately.
2. Administer adrenaline 0.5 mg IM (anterolateral thigh) — repeat every 5–15 minutes if response is inadequate.
3. Lay flat, elevate legs (if no respiratory compromise).
4. IV normal saline bolus for hypotension.
5. IV hydrocortisone 200 mg + IV chlorphenamine 10 mg as adjuncts.
6. Once the patient has stabilised (usually within 15–30 minutes), the antivenom infusion can be cautiously restarted at a slower rate under close observation.
7. Document the reaction and the management.
Premedication: Routine premedication with subcutaneous adrenaline 0.25 mg SC was previously recommended before antivenom infusion to reduce the incidence of early reactions. A landmark Sri Lankan trial (Premawardhena et al., 1999) showed that SC adrenaline 0.25 mg significantly reduced the incidence and severity of early reactions. However, this practice is not universally adopted across India — follow local institutional protocol and WHO recommendation (premedication is reasonable in settings with limited monitoring capacity).
Late reactions (serum sickness, 5–14 days post-infusion):
Serum sickness is a type III hypersensitivity reaction (immune complex deposition) occurring 5–14 days after antivenom administration. It presents with fever, urticaria, arthralgia, lymphadenopathy, and sometimes glomerulonephritis or vasculitis. It is more common with higher total doses of antivenom. Treatment is with oral prednisolone 1 mg/kg/day for 5–7 days and antihistamines. Patients should be warned at discharge to return if they develop these symptoms in the second week after the bite.
SELF-CHECK
Ten minutes into an antivenom infusion for Russell's viper VICC, a 35-year-old man develops wheeze, urticaria over his trunk, and his blood pressure drops to 80/50 mmHg. What is the FIRST action?
A. Administer IV hydrocortisone 200 mg immediately and continue the infusion at a slower rate
B. Stop the antivenom infusion and administer adrenaline 0.5 mg intramuscularly into the anterolateral thigh
C. Administer IV chlorphenamine 10 mg and observe for 15 minutes before stopping the infusion
D. Give salbutamol nebulisation for the wheeze and IV normal saline for the hypotension
Reveal Answer
Answer: B. Stop the antivenom infusion and administer adrenaline 0.5 mg intramuscularly into the anterolateral thigh
This is anaphylaxis — wheeze, urticaria, and hypotension together constitute a severe early reaction to antivenom. The FIRST action is to stop the infusion immediately, then administer adrenaline 0.5 mg IM into the anterolateral thigh (1:1000 solution). Adrenaline is the only proven life-saving treatment for anaphylaxis — it must come first, before antihistamines, before steroids, before anything else. IV hydrocortisone has a delayed onset of 4–6 hours and is adjunctive. Chlorphenamine alone is insufficient for anaphylaxis. Salbutamol is adjunctive for bronchospasm. Once stabilised, the antivenom can be carefully restarted at a slower rate as the patient still requires treatment for VICC.
Supportive Management and Monitoring After Antivenom
Antivenom neutralises circulating venom but does not immediately restore all the physiological damage it has caused. Supportive management directed at the complications of envenomation must run in parallel with antivenom therapy and continue after the infusion is complete. The intensity and duration of supportive care depend on the severity of the initial envenomation and the speed of response to antivenom.
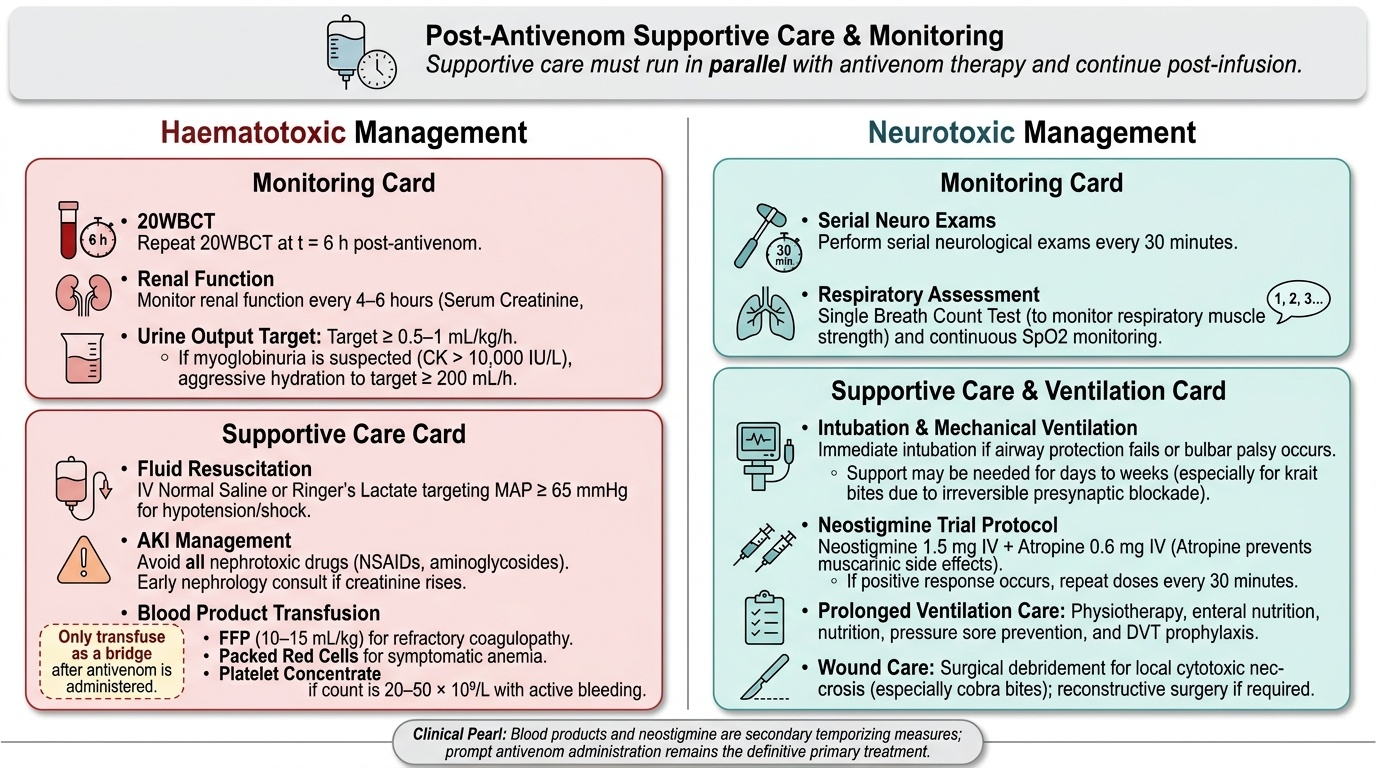
Provided image
For haematotoxic envenomation, the critical supportive priorities are: fluid resuscitation for hypotension and shock (IV normal saline or Ringer's lactate targeting MAP ≥65 mmHg); management of acute kidney injury (AKI) with IV hydration targeting urine output ≥0.5–1 mL/kg/hour, avoiding nephrotoxic drugs (NSAIDs, aminoglycosides), and early nephrology consultation if creatinine rises despite fluids; monitoring for myoglobinuria (aggressive hydration targeting urine output ≥200 mL/hour when CK > 10,000 IU/L); and blood product transfusion only as a bridge to antivenom effect — fresh frozen plasma (FFP) 10–15 mL/kg for refractory coagulopathy after antivenom, packed red cells for symptomatic anaemia, and platelet concentrate for count <20–50 × 10⁹/L with active bleeding. Blood products are temporising measures; they will be consumed again by circulating venom if antivenom has not been given first.
For neurotoxic envenomation, the critical priority is ventilatory support. If the patient requires intubation, mechanical ventilation may be necessary for days to weeks in krait envenomation (pre-synaptic blockade resolves only as new presynaptic terminals regenerate). Physiotherapy, enteral nutrition, pressure care, and DVT prophylaxis are required for prolonged ventilation. For cobra (post-synaptic) envenomation, a trial of neostigmine 1.5 mg IV + atropine 0.6 mg IV can be given after antivenom and may partially restore neuromuscular transmission — repeat doses every 30 minutes if an initial response is seen (atropine must be given each time to prevent muscarinic side effects). Wound care for local necrosis (especially cobra bites) may require surgical debridement; reconstructive surgery is sometimes needed for large areas of cytotoxic necrosis.
Monitoring after antivenom: Repeat the 20WBCT at 6 hours post-antivenom to assess coagulation recovery. Serial neurological examination every 30 minutes in neurotoxic cases. Repeat renal function and urine output monitoring every 4–6 hours. All patients with systemic envenomation should be admitted for minimum 24-hour observation; severe cases warrant ICU admission.
Self-Assessment: Antivenom Decision-Making
The competency assessed by IM21.7 integrates pharmacological knowledge (ASV mechanism, equine IgG, complement-mediated reactions) with clinical decision-making (indications, dose, adverse reaction management). Self-assessment in this domain means being able to answer four questions about any given snakebite patient: Does this patient have an indication for antivenom? If yes, how many vials and by what route? What am I watching for during the infusion, and what will I do if a reaction occurs? What is the 6-hour endpoint that tells me whether the dose was adequate? Working through the scenarios below with these four questions in mind will consolidate your antivenom competency. The final exam question at this level is always a case scenario where the indication must be identified correctly and the management sequenced correctly — knowing the correct answer to all four questions secures full marks.
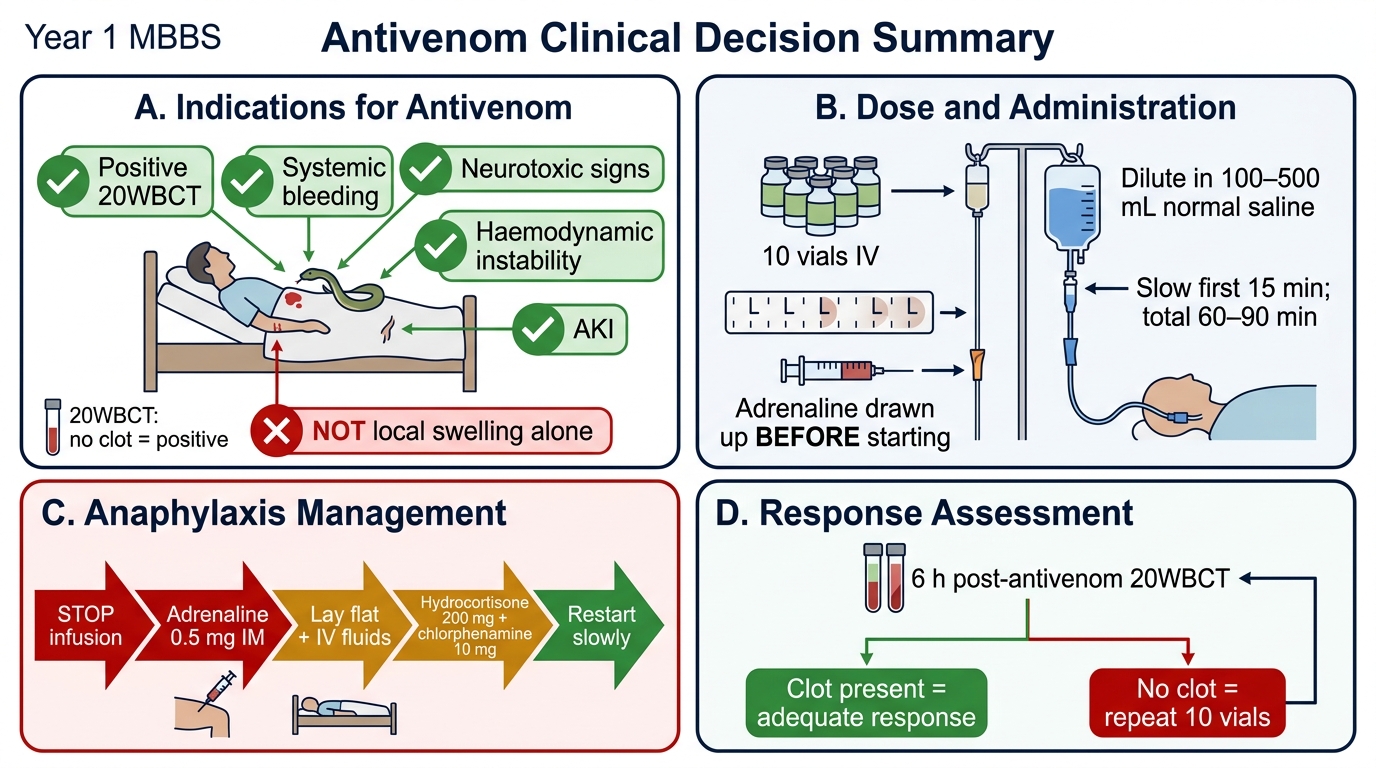
Antivenom Clinical Decision Summary
Scenario A: A 30-year-old woman has a positive 20WBCT and gingival bleeding 90 minutes after a viper bite. She has a history of asthma. Should antivenom be given? What precaution does the asthma history indicate?
Analysis: YES — positive 20WBCT plus active systemic bleeding are both absolute indications. Asthma increases the risk of severe bronchospasm during anaphylactoid reaction to ASV, so the risk is higher — but the risk of untreated VICC (intracranial haemorrhage, exsanguination) is even higher. Antivenom must be given. Precautions: have salbutamol nebuliser ready, have adrenaline drawn up before starting, begin the infusion at a very slow rate (half the usual starting rate), and have airway equipment available. Consider premedication (SC adrenaline 0.25 mg) as per local protocol.
Scenario B: A 55-year-old man bitten 4 hours ago has a 20WBCT that shows a clot (negative test). He has no bleeding, no ptosis, and BP is 120/80 mmHg. His right leg has swelling to mid-thigh from the ankle bite. A junior colleague insists antivenom should be given 'because the swelling is so bad'. How do you respond?
Analysis: The 20WBCT is negative, there is no systemic bleeding, no neurotoxic signs, and no haemodynamic compromise. Local swelling alone is NOT an indication for antivenom. The venom causing local tissue damage has already deposited in the tissue and is unreachable by circulating antivenom — giving ASV now exposes the patient to anaphylaxis risk without therapeutic benefit. The correct management is continued monitoring: repeat 20WBCT hourly for 6 hours, serial neurological exam, and antivenom only if any systemic criterion develops.
SELF-CHECK
A patient with confirmed Russell's viper VICC receives 10 vials of polyvalent ASV. Six hours later the 20WBCT still shows no clot and gingival bleeding continues. What is the most appropriate next step?
A. Administer fresh frozen plasma (FFP) as the antivenom has clearly failed and the patient needs clotting factors
B. Administer a second dose of 10 vials of antivenom as the 6-hour 20WBCT is still positive
C. Wait a further 6 hours as coagulation recovery takes 12 hours after the first dose
D. Perform a plasmapheresis to remove circulating venom complexes
Reveal Answer
Answer: B. Administer a second dose of 10 vials of antivenom as the 6-hour 20WBCT is still positive
A positive 20WBCT at 6 hours post-antivenom with ongoing bleeding indicates that the first 10 vials were insufficient to neutralise all circulating venom — a second dose of 10 vials is indicated. The 6-hour time point is specifically the assessment point for repeat dosing. FFP may be given as a supportive adjunct but if given without additional antivenom in the presence of still-circulating venom, the transfused clotting factors will themselves be consumed and the benefit will be transient. FFP is not a substitute for antivenom. Waiting a further 6 hours risks continued intracranial or visceral haemorrhage. Plasmapheresis has no proven role in routine snakebite management.
CLINICAL PEARL
The single most important rule in antivenom management: have adrenaline drawn up and ready before you start the infusion, not after the reaction starts. The window between onset of severe anaphylaxis and cardiovascular collapse can be as short as 2–3 minutes. In a busy emergency department where the doctor is called to the bedside after the reaction starts, the time to locate a vial of adrenaline, draw it up, and administer it may exceed the safe window. The rule is operationally simple: no antivenom infusion starts without adrenaline 0.5 mg already drawn up in a syringe, labelled, and lying on the patient's bedside tray.
A second pearl: do not give blood products before antivenom in VICC. Fresh frozen plasma, cryoprecipitate, or platelets given before antivenom will be consumed by still-circulating viper venom enzymes within hours, wasting expensive products and providing only transient benefit. The correct sequence is: antivenom first → then blood products if required after the 6-hour reassessment shows persistent coagulopathy despite adequate antivenom. This sequence is frequently tested in examinations because it is the opposite of what many students and clinicians intuitively try first.