Page 14 of 27
IM22.7 | Phosphide Poisoning — SDL Guide (Part 2)
Management and Prognosis
The management of aluminium phosphide poisoning is almost entirely supportive — there is no antidote, no chelating agent, and no pharmacological reversal of the mitochondrial injury. The clinician's task is to maintain perfusion of vital organs by external haemodynamic support while the body metabolises and excretes the phosphine, and to prevent secondary injury from hypoxia, acidosis, and arrhythmia. Despite the absence of a specific antidote, the quality of supportive care significantly influences outcome — patients who die from AlP poisoning in poorly resourced settings often die from preventable complications (untreated hypotension before the arrhythmia phase, unrecognised arrhythmia, or delays in ventilatory support) rather than from the toxin per se. The following management principles, applied systematically and urgently, represent the current standard of care.
Immediate resuscitation:
- IV access (two large-bore cannulas); continuous ECG monitoring; pulse oximetry; urinary catheter for hourly urine output monitoring.
- Haemodynamic support: IV fluids (normal saline 500 mL bolus) for hypotension — but be cautious of fluid overload given myocardial dysfunction and risk of pulmonary oedema (target mean arterial pressure > 65 mmHg with careful reassessment after each bolus). Vasopressors (noradrenaline first-line, adrenaline as second-line adjunct) for shock not responding to fluids; dopamine has been studied but noradrenaline is preferred. Intra-aortic balloon pump (IABP) or mechanical circulatory support should be considered in refractory cardiogenic shock in centres with this capability — it can support the failing heart while phosphine is excreted.
- High-flow oxygen (100% FiO₂ via non-rebreather mask or mechanical ventilation) to maximise aerobic metabolism in surviving mitochondria. Intubate and ventilate for respiratory failure.
- Sodium bicarbonate for severe metabolic acidosis (pH < 7.1) to prevent arrhythmia worsening (acidosis increases QTc and arrhythmia risk); target pH > 7.2.
What NOT to do:
- NO gastric lavage in the emergency department — controversial and potentially harmful: lavage agitates the tablet, increases phosphine liberation rate, and creates phosphine-laden vomit and gas in the room (risk to healthcare workers); most guidelines advise against routine lavage except in very early presentations (< 30 minutes) with adequate airway protection and staff with respirators.
- NO magnesium sulphate by NGT — although some case reports and small studies from India and Pakistan have suggested magnesium may reduce phosphine toxicity (by competing with phosphine for mitochondrial binding sites or by antioxidant effects), there is insufficient evidence to recommend it routinely and it may worsen hypotension.
- Avoid ipecac/emesis — already vomiting; induced emesis increases phosphine gas exposure.
Coconut oil: An interesting Indian practice supported by some observational data: administration of coconut oil (30–60 mL orally if the patient is conscious) before or shortly after AlP ingestion may reduce the amount of phosphine liberated by forming a lipid layer over the tablet, limiting the water contact needed for the liberation reaction. This is based on the low-moisture hydrophobic environment created by the oil layer. The evidence is limited (case series, no RCTs) but it is inexpensive, safe, and widely used as a first-aid measure in farming communities in India. It is not a treatment but a potentially useful harm-reduction measure if given early.
Antioxidant therapies: Vitamin C, vitamin E, N-acetylcysteine, and glutathione have been studied as potential adjuncts to limit phosphine-mediated oxidative damage. None has shown convincing survival benefit in controlled studies. They are not standard of care but some centres use NAC as an adjunct given its good safety profile.
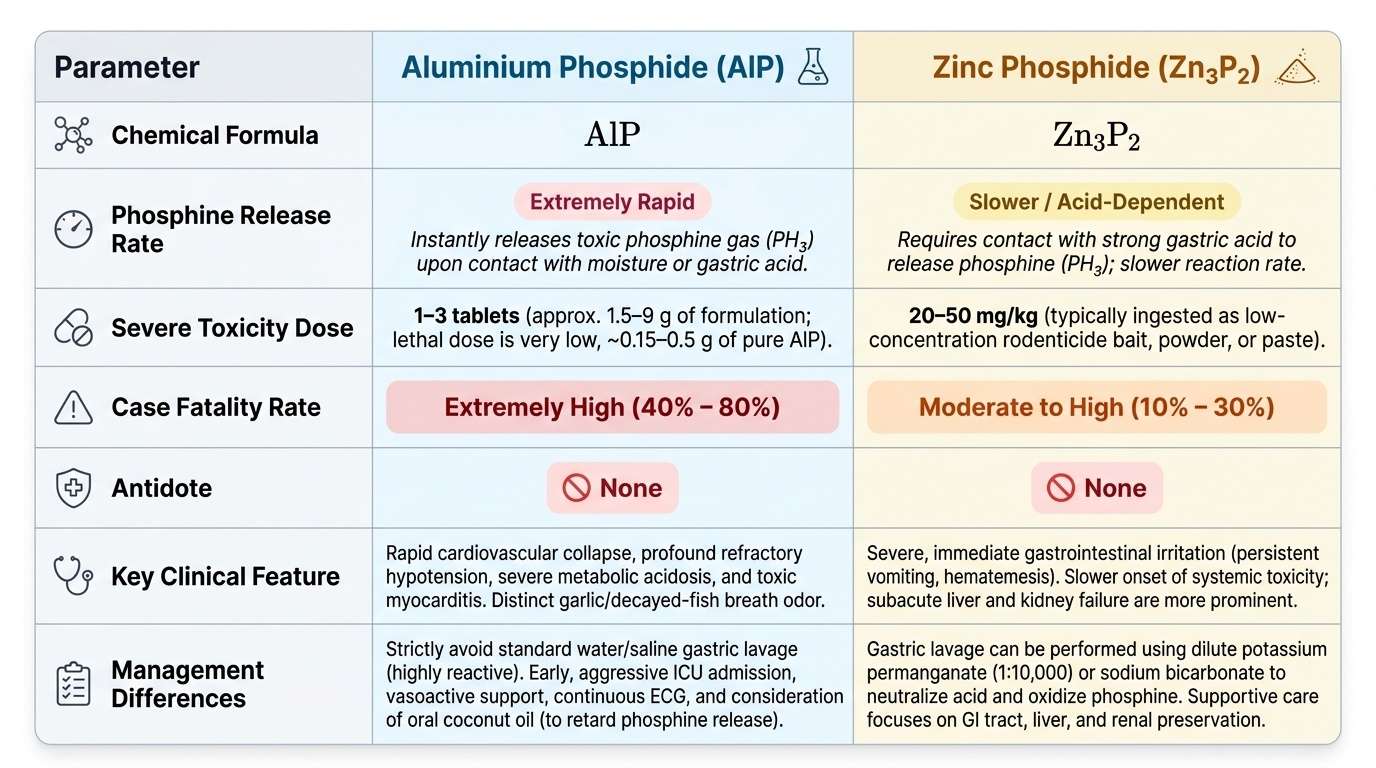
Prognosis: The case fatality rate of AlP poisoning with ingestion of 2 or more tablets is 60–90% even in tertiary care settings. Patients who present within 2 hours, ingest a single tablet, and have only mild haemodynamic changes have a chance of survival with aggressive supportive care. The family must be counselled early, honestly, and with compassion about the nature of this poisoning and its prognosis — this conversation cannot be deferred to after cardiac arrest. Zinc phosphide poisoning has a somewhat better prognosis due to lower phosphine release per ingested mass.
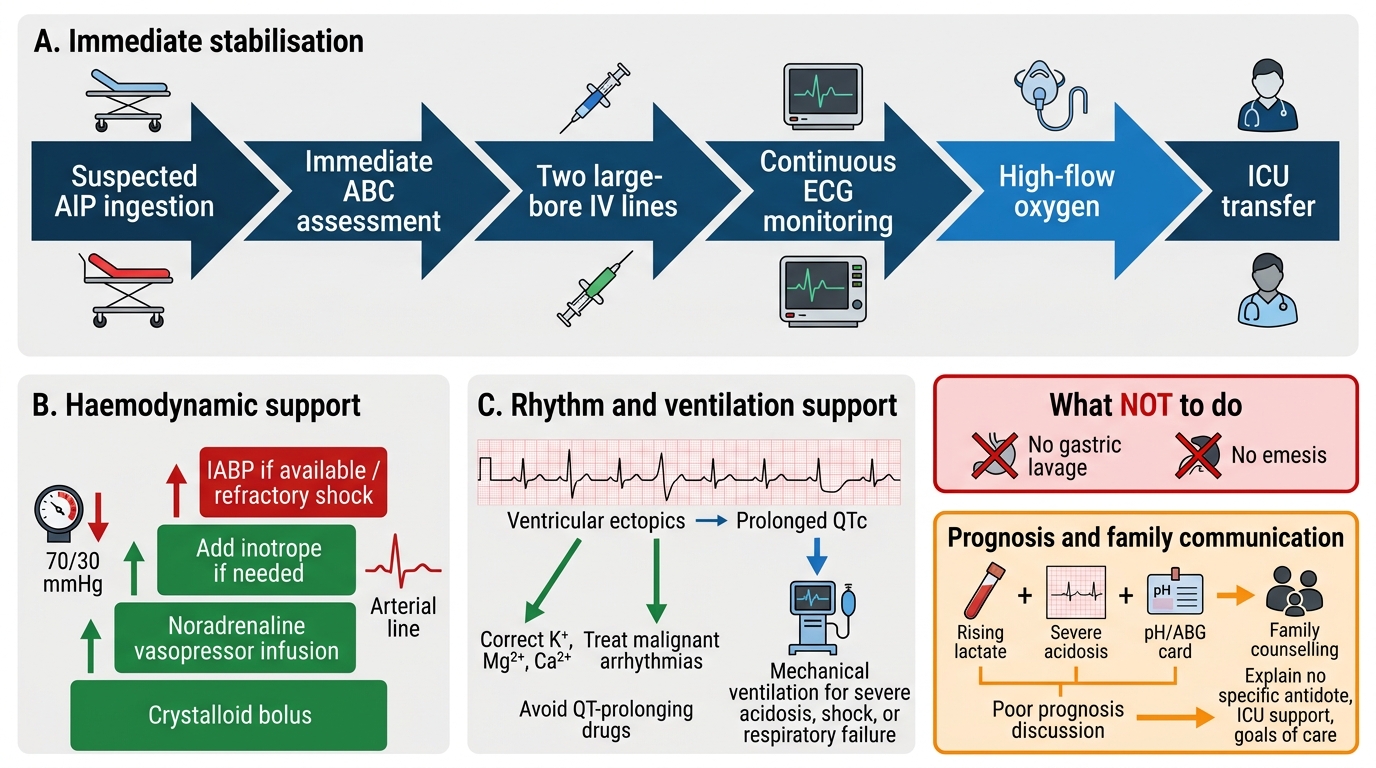
Management Flowchart for Aluminium Phosphide Poisoning
SELF-CHECK
A 22-year-old woman ingested 3 AlP tablets 4 hours ago. BP 70/30 mmHg despite 2 L of IV normal saline. Serum lactate 12 mmol/L and rising. ECG shows frequent ventricular ectopics and QTc 560 ms. Her ABG pH is 7.08. What is the MOST important management step at this point?
A. Start IV N-acetylcysteine as the specific antidote for phosphine toxicity
B. Start IV sodium bicarbonate, vasopressor support (noradrenaline), and consider mechanical ventilation while counselling family regarding poor prognosis
C. Perform urgent gastric lavage to remove the unabsorbed tablets
D. Give IV pralidoxime 1 g immediately to reactivate mitochondrial enzymes
Reveal Answer
Answer: B. Start IV sodium bicarbonate, vasopressor support (noradrenaline), and consider mechanical ventilation while counselling family regarding poor prognosis
This patient has refractory shock, severe metabolic acidosis (pH 7.08), rising lactate, and arrhythmia — a picture of severe AlP poisoning with multi-organ failure. There is no specific antidote. The correct response is: (1) IV sodium bicarbonate to correct severe acidosis (pH < 7.1) and reduce arrhythmia risk; (2) vasopressor support (noradrenaline) for refractory cardiogenic/distributive shock; (3) mechanical ventilation for respiratory failure and to reduce the work of breathing; (4) immediate honest family counselling about the extremely poor prognosis (lactate 12 mmol/L + pH 7.08 + three tablets = very high mortality). Gastric lavage at 4 hours is dangerous (tablet has largely dissolved) and exposes staff to phosphine. NAC and pralidoxime have no efficacy in phosphine poisoning.
Self-Assessment: Phosphide Poisoning in Context
The following self-assessment exercises integrate your knowledge of the clinical course, pathophysiology, investigation, and management of aluminium phosphide poisoning — all tested at the KH level required by NMC competency IM22.7. For each question, reason through the clinical logic before reading the analysis.
Provided image
Scenario A: A 28-year-old man is brought in 1 hour after ingesting 1 AlP tablet. He is vomiting and complaining of chest tightness. BP 100/70 mmHg (borderline), HR 105 bpm, SpO₂ 96%, ABG: pH 7.31, lactate 3.8 mmol/L. ECG shows sinus tachycardia with no ST changes. What is the risk stratification and management plan?
Analysis: Relatively early presentation (1 hour), single tablet, pH 7.31 (mild acidosis), lactate 3.8 mmol/L (mildly elevated), no haemodynamic collapse yet. Risk is substantial but not immediately critical — this patient can survive with aggressive supportive care if managed correctly. Management: (1) ICU admission immediately — do not put on a general ward. (2) Continuous ECG monitoring. (3) Repeat ABG, lactate, ECG every 2 hours — clinical course can deteriorate rapidly. (4) IV access, high-flow oxygen. (5) Do NOT attempt gastric lavage (1 hour — tablet is likely partially dissolved; risk to staff). (6) Consider oral coconut oil 30 mL (harm-reduction, limited evidence but safe). (7) Vasopressors on standby. (8) Honest counselling: even with single tablet, mortality can be 20–40% — family should be present.
Scenario B: A 19-year-old woman's ECG shows sinus tachycardia at 120 bpm at 2 hours, progressing to ST depression in leads V4–V6 at 4 hours, and now at 6 hours there is sustained monomorphic VT at 180 bpm. BP has fallen to 50/30 mmHg despite noradrenaline infusion. What does this ECG progression indicate, and what additional intervention should be considered?
Analysis: This ECG progression — sinus tachycardia → myocardial ischaemia (ST depression) → ventricular tachycardia — represents sequential deterioration of myocardial energy metabolism from phosphine toxicity. It is a direct marker of advancing cardiomyocyte death. The sustained VT with haemodynamic collapse requires: (1) immediate defibrillation if patient becomes pulseless (VF or pulseless VT); (2) synchronised cardioversion for haemodynamically compromising VT; (3) amiodarone 150 mg IV for recurrent VT if cardioversion achieves temporary termination; (4) correction of hypokalaemia and hypomagnesaemia (which worsen QTc and arrhythmia threshold); (5) consideration of mechanical circulatory support (IABP or VA-ECMO if available) — this is refractory cardiogenic shock from mitochondrial failure; vasopressors alone are insufficient. Family counselling urgently — this is a terminal trajectory.
SELF-CHECK
Which of the following BEST explains why aluminium phosphide poisoning has no specific antidote, unlike organophosphate poisoning which can be treated with pralidoxime?
A. Phosphine has a longer half-life than organophosphates and accumulates irreversibly in fat tissue
B. Phosphine causes direct oxidative damage to mitochondrial electron transport chain complexes that is not enzymatically reversible, unlike the enzymatic AChE inhibition of organophosphates which can be partially reversed by pralidoxime before ageing
C. The aluminium in AlP competitively inhibits all antidote binding sites in the body
D. Phosphine is rapidly excreted by the kidney before any antidote can be administered
Reveal Answer
Answer: B. Phosphine causes direct oxidative damage to mitochondrial electron transport chain complexes that is not enzymatically reversible, unlike the enzymatic AChE inhibition of organophosphates which can be partially reversed by pralidoxime before ageing
Organophosphates cause toxicity by phosphorylating the active site serine of AChE — an enzymatic modification that pralidoxime can reverse before ageing by displacing the phosphate group, regenerating active enzyme. Phosphine, by contrast, causes direct oxidative damage to mitochondrial membrane components and electron transport chain complexes (I, II, IV — principally cytochrome c oxidase). This is not an enzyme active site modification — it is oxidative destruction of protein structure and mitochondrial lipid membranes. No drug can restore the phosphorylation capacity of mitochondria damaged by oxidative stress. The mechanism is fundamentally different and inherently non-reversible by any currently available pharmacological approach.
CLINICAL PEARL
Aluminium phosphide poisoning is the one emergency where the most important clinical skill is not knowing what to DO but knowing what NOT to do, combined with knowing how to have an honest conversation with a family within the first 2 hours of presentation. The three things NOT to do: (1) do NOT perform gastric lavage routinely — it exposes staff to phosphine; (2) do NOT give false hope about an antidote that does not exist; (3) do NOT delay ICU-level monitoring in a patient who appears 'stable' at 2 hours — the peak cardiovascular toxicity phase is 4–12 hours and can be explosive in its onset. The family counselling conversation is not optional — begin it when you admit the patient, not when the arrest has started.