Page 4 of 27
IM22.2-3 | Plant and Corrosive Poisoning — SDL Guide
Learning Objectives
- Enumerate common plant poisons encountered in India and describe their toxicology, clinical features, prognosis, and approach to detoxification
- Describe the toxicology, clinical features, prognosis, and management of common corrosive poisoning in India
- Distinguish acid from alkali corrosive injury and apply the principles of emergency management
- Identify the role of endoscopy in corrosive ingestion and describe the criteria for surgical referral
INSTRUCTIONS
Plant and corrosive poisoning account for significant morbidity in India. This module covers the major plant toxins with an emphasis on Datura, Cleistanthus, and oleander — all prevalent in the Indian subcontinent — and the two major corrosive categories (acid and alkali), with their distinct pathology and management principles.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 454 — Poisoning and Drug Overdose (textbook)
- API Textbook of Medicine, 10th ed., Ch. 26 — Poisoning (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 9 — Poisoning (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old woman is brought in confused and agitated. Her husband reports that she consumed a herbal preparation from a local healer for depression three hours ago. On examination: heart rate 140 bpm, temperature 39.2°C, pupils 8 mm and fixed, dry flushed skin, urinary retention, and she is pulling at her clothing, muttering incoherently. Meanwhile, in the adjacent cubicle, a 22-year-old man has been brought in by his colleagues after drinking from an unlabelled bottle at a construction site. He is in severe pain, drooling, unable to swallow, and his lips and anterior tongue are covered in white-grey sloughing mucosa. His voice is hoarse and his oxygen saturation is 88%. Two presentations, both potentially fatal, requiring entirely different emergency responses: one an anticholinergic plant toxin demanding supportive care and cooling; the other a corrosive airway emergency where the next ten minutes will determine whether he needs emergent intubation or tracheostomy. Plant and corrosive poisoning require you to recognise the pattern instantly and act — before waiting for any investigation.
WHY THIS MATTERS
India's rural and peri-urban populations use plants extensively in traditional medicine, agriculture, and — unfortunately — for intentional self-harm. Datura stramonium (jimsonweed/dhatura) poisoning is endemic across the subcontinent and a common cause of anticholinergic toxidrome presentations. Oleander (Nerium oleander, Thevetia peruviana/yellow oleander) is one of the most common causes of plant-related cardiac glycoside poisoning in South India and Sri Lanka; aconitite poisoning from Aconitum species is prevalent in the Himalayan foothills and as an adulterant in Ayurvedic preparations. Corrosive ingestion — acid (hydrochloric, sulphuric) and alkali (sodium hydroxide, bleach) — remains prevalent, particularly as a method of self-harm and in accidental domestic and industrial exposures. As a final-year student, you will encounter these cases in emergency medicine, general medicine, and surgical rotations. The NMC competencies IM22.2 and IM22.3 require KH-level application of this knowledge to patient care.
RECALL
From your earlier pharmacology and toxicology studies, recall the autonomic receptor framework: muscarinic blockade produces the anticholinergic toxidrome (dry, hot, mydriasis, tachycardia, delirium); muscarinic stimulation via inhibition of acetylcholinesterase produces the cholinergic toxidrome (SLUDGE, miosis, bradycardia). Cardiac glycosides (digoxin, oleandrin) inhibit the Na/K-ATPase pump, increasing intracellular calcium and causing positive inotropy at low doses but bradycardia, heart block, and ventricular arrhythmias at toxic concentrations. From surgery, recall the principle that alkali injury produces liquefactive necrosis (penetrates deeper) while acid injury produces coagulative necrosis (self-limiting eschar). From your earlier toxicology SDL, recall that atropine blocks muscarinic receptors and pralidoxime reactivates acetylcholinesterase. These foundations underpin everything in this module.
Clinical Presentation of Common Plant Poisonings
Plant poisonings in India present across a spectrum from mild anticholinergic delirium to fatal cardiac arrhythmias and respiratory paralysis. The clinical presentation is driven by the class of toxin contained in the plant. For each plant discussed below, the clinical picture is entirely predictable once the mechanism is understood — making the identification of plant type from clinical features alone a core bedside skill.
Provided image
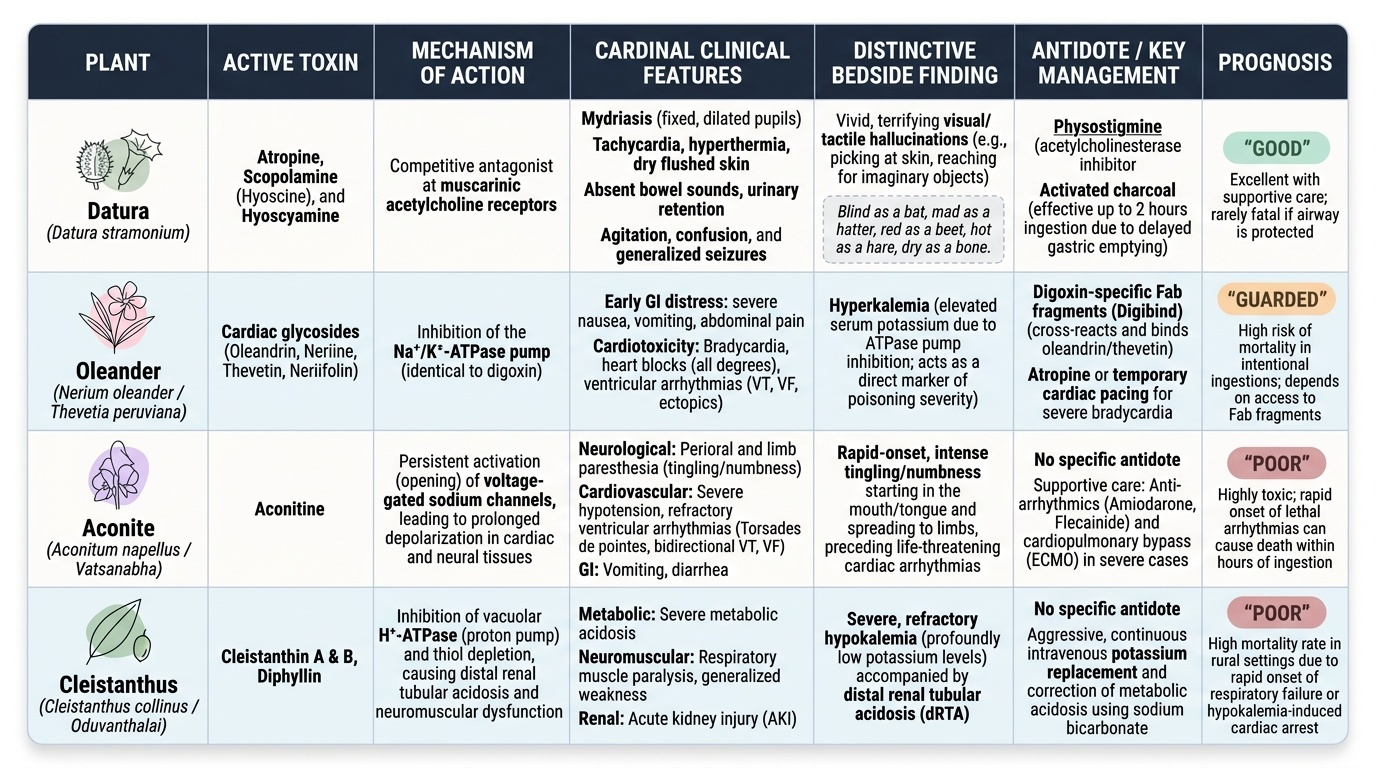
Datura stramonium (Jimsonweed / Dhatura / Angel's trumpet) contains atropine, scopolamine (hyoscine), and hyoscyamine — all potent competitive antagonists at muscarinic acetylcholine receptors. This is the most common plant anticholinergic poisoning in India, occurring both accidentally (in children eating seeds or berries) and as deliberate poisoning (seeds added to food or beverages). Presentation is the classic anticholinergic toxidrome: tachycardia, hyperthermia, mydriasis (maximally dilated, fixed pupils), dry flushed skin, absent bowel sounds, urinary retention, agitation, confusion, hallucinations (often visual and tactile — picking at skin, reaching for imaginary objects), and in severe cases, generalised seizures and coma. The hallucinations are characteristically vivid and terrifying, differentiating Datura delirium from delirium tremens or psychosis. The onset is 30–60 minutes after ingestion. Duration can be prolonged (12–48 hours) due to delayed gastric emptying caused by the anticholinergic drug itself — hence activated charcoal may be useful even at 2 hours post-ingestion if the airway is protected.
Oleander (Nerium oleander — common oleander; Thevetia peruviana — yellow oleander) contains cardiac glycosides (oleandrin and neriine in Nerium; thevetin and neriifolin in Thevetia). Yellow oleander is particularly prevalent in South India and is one of the most common causes of intentional plant poisoning in the region. The mechanism is inhibition of the Na/K-ATPase pump — identical to digoxin toxicity. Clinical features: nausea, vomiting, and abdominal pain are early and prominent (and help distinguish oleander from pure cardiac toxicity); followed by bradycardia, heart block (all degrees), and ventricular arrhythmias (particularly ventricular ectopics, VT, VF). Hyperkalaemia develops from Na/K-ATPase inhibition and is a marker of severity. The ECG may show any arrhythmia seen in digoxin toxicity — bradyarrhythmias are most common, but bidirectional VT is pathognomonic of cardiac glycoside toxicity. Prognosis correlates with potassium level and the degree of arrhythmia. Digoxin-specific Fab antibody fragments (Digibind/DigiFab) cross-react with plant cardiac glycosides and can reverse toxicity — their use should be considered in life-threatening arrhythmias or severe hyperkalaemia, though high doses may be needed due to the greater quantity of glycoside relative to digoxin.
Aconitum species (Aconite / Monkshood / Vatsanabha) contain aconitine and related alkaloids that activate and then permanently open voltage-gated sodium channels (Nav), preventing membrane repolarisation. Found in the Himalayan region and used in traditional Ayurvedic preparations (as Vatsanabha, supposedly detoxified but often incompletely processed). Clinical features begin within 30–60 minutes of ingestion: paraesthesiae and numbness of the lips, tongue, fingers, and skin (the initial and characteristic symptom); followed by limb weakness and paralysis, severe nausea and vomiting, hypersalivation, hypotension, and bradycardia. Cardiac arrhythmias are the most dangerous feature — ventricular tachycardia (including torsades de pointes) and VF are causes of death. Aconitite poisoning should be suspected in any patient with paraesthesiae followed by cardiac arrhythmia, particularly with a history of ingesting traditional herbal preparations. There is no specific antidote; management is supportive (antiarrhythmics as needed, temporary pacing for bradycardia, ventilatory support). The prognosis is grave once arrhythmia develops.
Cleistanthus collinus (Garari / Oduvan) is a shrub native to peninsular India (particularly Tamil Nadu, Andhra Pradesh, Telangana) whose leaves contain cleistanthin and other toxic diterpenoids that inhibit oxidative phosphorylation in mitochondria, particularly affecting the kidney and neuromuscular system. Clinical features: nausea, vomiting, abdominal pain, followed by hypokalaemia (a hallmark and early marker), hyponatraemia, metabolic acidosis, renal failure, ascending paralysis (flaccid), and respiratory paralysis. Death occurs from respiratory failure, renal failure, or cardiac arrhythmia secondary to electrolyte disturbance. There is no antidote; management is aggressive potassium replacement, ventilatory support, and haemodialysis for renal failure.
Pathophysiology and Diagnosis of Plant Poisoning
Understanding the pathophysiology of plant poisons allows the clinician to predict the clinical course, anticipate complications, and select targeted interventions. Each major Indian plant toxin has a distinct biochemical mechanism that maps directly onto its clinical syndrome. The diagnostic approach to plant poisoning is fundamentally clinical — laboratory tests confirm complications but rarely identify the specific toxin.
Anticholinergic mechanism (Datura): The belladonna alkaloids (atropine, scopolamine) competitively and reversibly block muscarinic acetylcholine receptors at postganglionic parasympathetic nerve endings. The result is unopposed sympathetic tone at every organ that normally receives parasympathetic innervation: the heart (tachycardia), salivary glands (dry mouth), sweat glands (anhidrosis → hyperthermia), bronchial glands (dry secretions), bladder detrusor (urinary retention), GI smooth muscle (ileus), iris sphincter (mydriasis). The CNS effects of scopolamine (delirium, hallucinations) are mediated by blockade of central muscarinic receptors. The diagnosis is clinical; there is no rapid bedside test for belladonna alkaloids. A physostigmine trial (a reversible anticholinesterase that crosses the blood-brain barrier) can be both diagnostic and therapeutic — a response (decreased heart rate, improved cognition, reduced agitation) confirms anticholinergic toxidrome — but it carries risks and is reserved for severe cases.
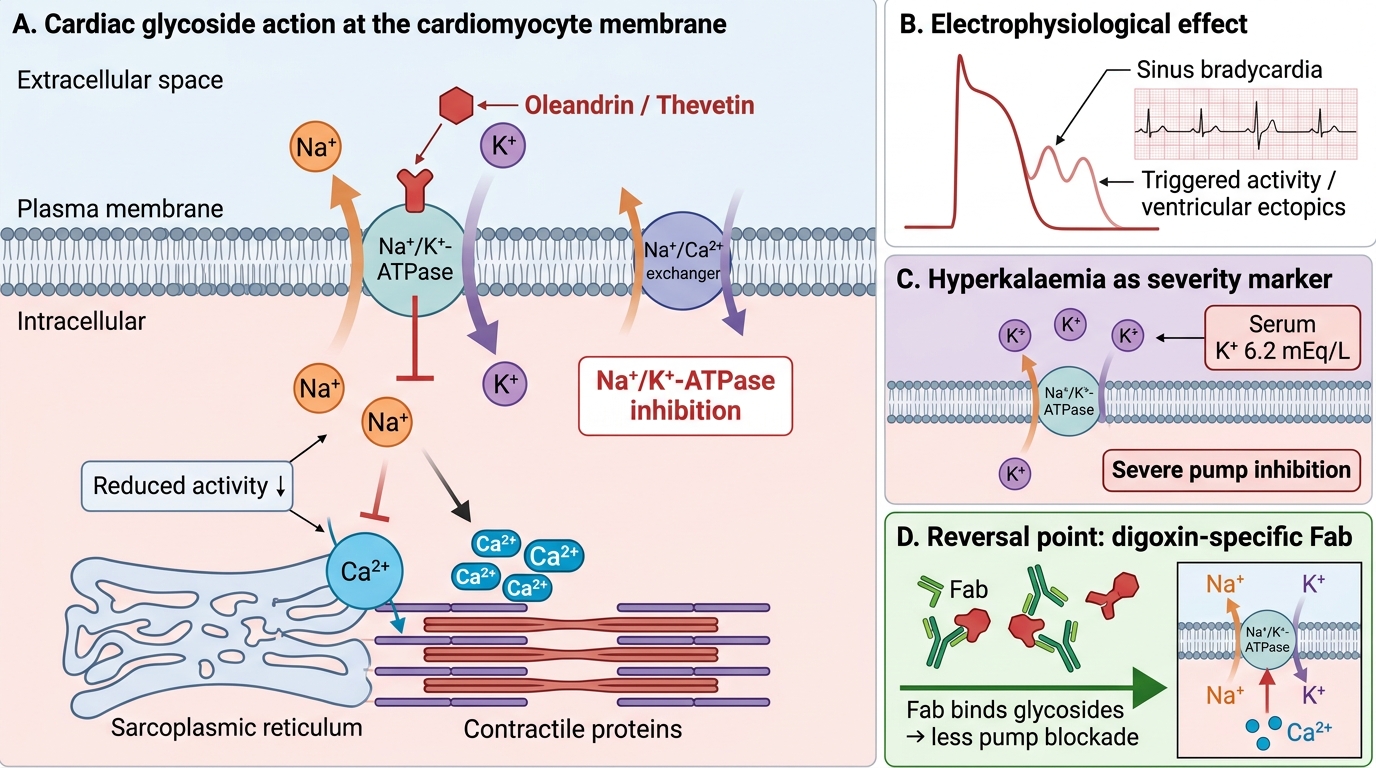
Cardiac glycoside mechanism (Oleander): Oleandrin and thevetin bind to and inhibit the alpha subunit of Na/K-ATPase on myocardial cell membranes. The consequence is: reduced sodium extrusion → increased intracellular sodium → reduced Na-Ca exchanger activity → increased intracellular calcium → increased myocardial contractility (therapeutic effect at low doses) and increased automaticity of ectopic pacemakers (toxic effect at higher doses). The increase in intracellular calcium also sensitises the myocardium to triggered activity (delayed afterdepolarisations) — the mechanism of digoxin-related arrhythmias. Simultaneously, enhanced vagal tone (increased AV nodal refractory period) explains bradycardia and AV block. Serum potassium is a critical prognostic marker: Na/K-ATPase inhibition prevents potassium entry into cells, causing hyperkalaemia; K > 5.5 mEq/L in cardiac glycoside poisoning correlates with high mortality. ECG findings: bradycardia, PR prolongation, AV block (1st, 2nd, 3rd degree), atrial tachycardia with block (a hallmark of digoxin toxicity), frequent ventricular ectopics, and bidirectional VT.
Sodium channel toxicity (Aconite): Aconitine first activates and then permanently opens Nav1.5 (cardiac) and Nav1.4 (skeletal muscle) voltage-gated sodium channels. Persistent sodium entry depolarises membranes, preventing repolarisation and action potential generation. This explains the characteristic paraesthesiae (sensory nerve channels) and subsequent paralysis (motor nerve/muscle channels). Cardiac consequences: persistent membrane depolarisation → triggered arrhythmias (VT, VF), bradycardia (AV nodal effects). ECG: wide complex ventricular tachycardia, polymorphic VT (torsades-like), AV block.
Diagnosis: There are no routine bedside tests for plant toxin identification. The diagnosis is based on: (1) history (plant ingestion, herbal preparation, traditional medicine, or found near plants); (2) clinical syndrome (anticholinergic pattern for Datura; GI + arrhythmia for oleander; paraesthesiae + arrhythmia for aconite; hypokalaemia + paralysis for Cleistanthus); (3) ECG (critical for arrhythmia detection); (4) serum electrolytes, renal function, ABG for complications. In oleander poisoning, serum digoxin level may detect cross-reactive glycosides — a measurable level in a patient who has never taken digoxin confirms cardiac glycoside poisoning.
Cardiac Glycoside Poisoning: Pump Blockade to Fab Reversal
SELF-CHECK
A 28-year-old woman from a rural area in South India presents with nausea, vomiting, and palpitations 2 hours after eating seeds from a garden plant. ECG shows sinus bradycardia at 36 bpm with frequent ventricular ectopics. Serum potassium is 6.2 mEq/L. Her serum digoxin level is reported as 3.1 ng/mL despite no history of taking digoxin. What is the most likely diagnosis and most appropriate specific treatment?
A. Datura poisoning — give physostigmine IV
B. Yellow oleander poisoning — give digoxin-specific Fab fragments
C. Aconite poisoning — give sodium bicarbonate IV
D. Cleistanthus poisoning — give aggressive potassium supplementation
Reveal Answer
Answer: B. Yellow oleander poisoning — give digoxin-specific Fab fragments
The clinical picture — nausea/vomiting, bradycardia, ventricular ectopics, hyperkalaemia, and a detectable digoxin level without prior digoxin use — is the classic presentation of yellow oleander (Thevetia peruviana) cardiac glycoside poisoning. Cross-reactive cardiac glycosides (thevetin, neriifolin) are detected by standard digoxin assays. Hyperkalaemia (K 6.2) indicates severe Na/K-ATPase inhibition and high mortality risk. Digoxin-specific Fab fragments cross-react with plant glycosides and are the definitive treatment for life-threatening arrhythmia or hyperkalaemia in this context. Datura causes anticholinergic syndrome (mydriasis, dry, hot). Aconite causes paraesthesiae. Cleistanthus causes hypokalaemia (not hyperkalaemia).
Management and Prognosis of Plant Poisoning
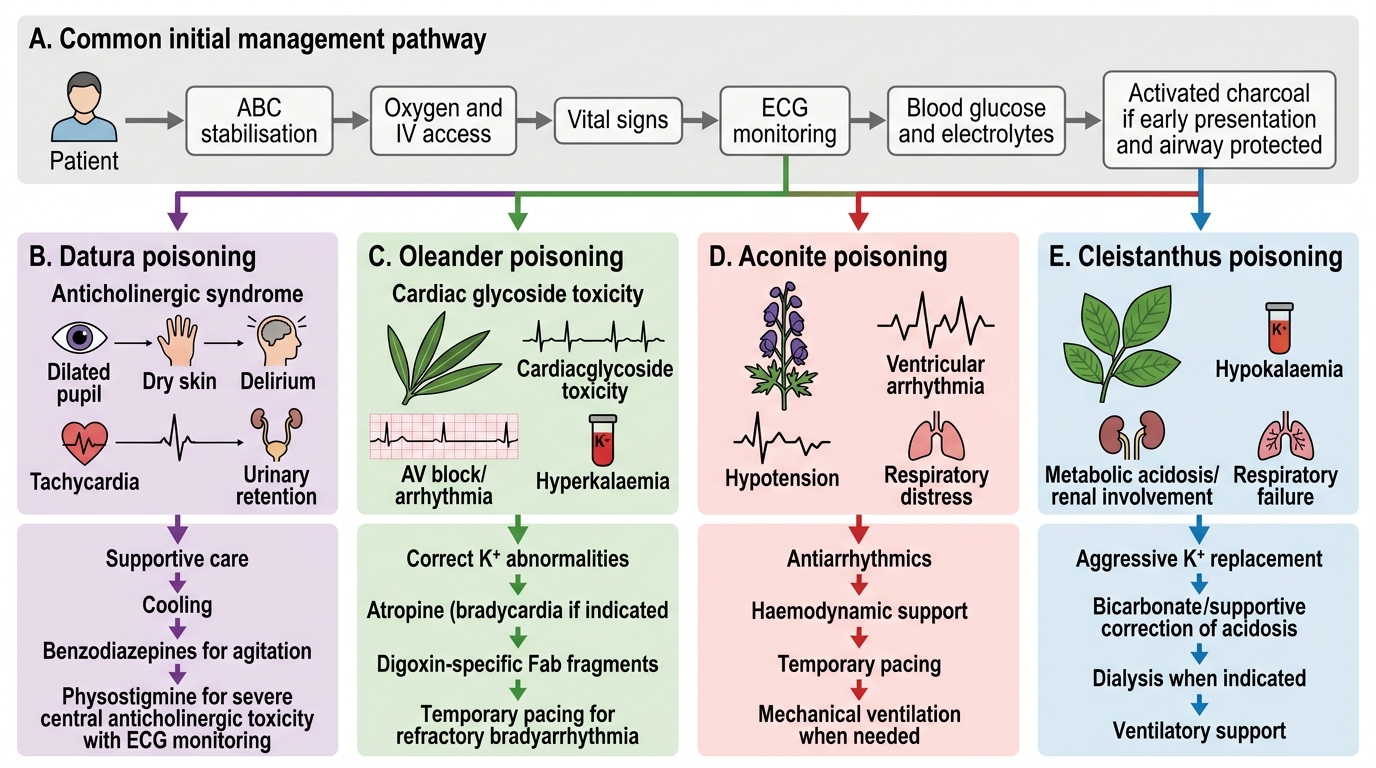
The management of plant poisoning is governed by three overarching principles: first, systematic stabilisation using the ABC framework (because airway, breathing, and haemodynamic compromise are the immediate threats to life regardless of the specific toxin); second, administration of a specific antidote where one exists (Fab fragments for cardiac glycoside poisoning; physostigmine selectively for severe anticholinergic delirium from Datura); and third, active prevention and treatment of the predictable complications based on each toxin's mechanism — arrhythmia monitoring and electrolyte correction for cardiac glycoside and aconite poisonings, aggressive potassium replacement and renal support for Cleistanthus, and temperature management and seizure control for anticholinergic poisoning. The management approach for each toxin follows directly from its pathophysiology, which is why a mechanistic understanding — not a memorised drug list — is what allows you to reason through unfamiliar plant poisonings in practice. The sections below give the toxin-specific management plan for the four major Indian plant poisons covered in this module.
Datura (anticholinergic) poisoning management:
- Stabilisation: ABC; IV access; cardiac monitoring (continuous ECG).
- Decontamination: activated charcoal 50 g if presentation within 2 hours and airway protected (anticholinergics delay gastric emptying, so AC remains beneficial longer than for most toxins).
- Specific treatment: primarily supportive. Benzodiazepines (diazepam 5–10 mg IV) for agitation and seizures. Active cooling measures (tepid sponging, fans) for hyperthermia — do not give antipyretics (not effective for drug-induced hyperthermia). Urinary catheterisation for retention.
- Physostigmine 1–2 mg slow IV (over 5 minutes) can rapidly reverse delirium and reduce agitation — consider for severe delirium or life-threatening tachyarrhythmia; requires cardiac monitoring (contraindicated in TCA co-ingestion and cardiac conduction defects).
- Prognosis: excellent with supportive care; fatal outcome rare but possible from hyperthermia, seizures, or cardiac arrhythmia; full recovery usual within 24–48 hours.
Oleander/Yellow oleander (cardiac glycoside) poisoning management:
- Stabilisation: cardiac monitoring is mandatory — continuous ECG; IV access; correct hyperkalaemia (calcium gluconate IV for membrane stabilisation, dextrose-insulin to drive K into cells; do NOT use sodium bicarbonate which has variable efficacy and may precipitate calcium precipitation in co-administered calcium).
- Decontamination: activated charcoal 50 g within 1 hour if airway protected. MDAC (multiple-dose activated charcoal) may help for thevetin (some enterohepatic recirculation).
- Specific treatment: Digoxin-specific Fab antibody fragments (Digibind/DigiFab) — the definitive antidote. Each vial (38 mg) binds approximately 0.5 mg of digoxin; for plant glycoside poisoning, empirical dosing of 10–20 vials may be required given the much higher quantity of toxin. Indications: bradycardia causing haemodynamic compromise, second/third degree AV block, any ventricular arrhythmia, serum K > 5 mEq/L.
- Temporary cardiac pacing may be required for complete AV block not responding to atropine.
- Prognosis: mortality is significant (10–30% in series from South India/Sri Lanka) and correlates with initial potassium level and degree of arrhythmia.
Aconite poisoning management:
- Stabilisation: cardiac monitoring; IV access; airway protection (risk of respiratory paralysis).
- Decontamination: activated charcoal if within 1 hour.
- No specific antidote. Cardiac arrhythmias are managed with standard antiarrhythmics: amiodarone or flecainide for ventricular tachycardia; temporary pacing for bradyarrhythmias. Ventilatory support for respiratory paralysis.
- Prognosis: guarded; fatal arrhythmias occur even in hospital; mortality 10–20% in symptomatic cases.
Cleistanthus collinus poisoning management:
- Aggressive potassium replacement (IV KCl infusion with continuous ECG monitoring) — hypokalaemia is the life-threatening electrolyte disturbance.
- Ventilatory support (non-invasive or invasive) for respiratory paralysis — may be prolonged.
- Haemodialysis for acute kidney injury.
- No antidote; prognosis is poor in symptomatic cases.
Management Algorithm for Plant Poisoning