Page 19 of 27
IM22.9-13 | Poison Centre and Medico Legal Workflow — SDL Guide
Learning Objectives
- Describe the functions of a poison centre and recognise when to contact one for toxicological advice
- Enumerate the medico-legal aspects of poisoning cases including mandatory documentation and police intimation
- Write a structured medico-legal report for a poisoning case at the supervised house officer (SH) level
- Counsel the family of a poisoning patient regarding prognosis, sequelae, and mental health follow-up
- Identify the indications for psychiatric consultation in poisoning cases, particularly deliberate self-harm and substance abuse
INSTRUCTIONS
Poisoning cases carry significant medico-legal implications in India. Most cases of deliberate self-harm (DSH), homicide by poison, and suspicious deaths require formal medico-legal documentation, police intimation, and coordinated care between medicine and psychiatry. This module covers the clinical skills required for managing the medico-legal and psychosocial dimensions of poisoning — from contacting a poison information centre to writing a medico-legal report to counselling the family and referring to psychiatry.
References
- API Textbook of Medicine, 10th ed., Ch. 26 — Poisoning (textbook)
- Modi's Medical Jurisprudence and Toxicology, 24th ed. (textbook)
- Karmakar's Forensic Medicine and Toxicology, 4th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the on-call house officer at 2 AM when a 22-year-old woman is brought in unconscious after consuming an unknown substance. The family says she ingested something from the kitchen cupboard, but they are vague about what it was — they hand you a container with a faded, partially torn label. You stabilise her and call Poison Control. The toxicologist on duty walks you through the likely toxidrome, suggests specific investigations, and advises that the agent is not charcoal-absorbable — this single phone call changes your management plan. Before you can proceed, a police constable arrives and asks you to prepare a First Information Report (FIR) supporting document. The patient's mother is sobbing in the corridor and asking whether her daughter will survive, whether there will be brain damage, and why this happened — she suspects it was deliberate. Your senior is not available. By the end of this module, you will know exactly what to do in each of these three parallel tracks: clinical toxicology advice from the poison centre, medico-legal documentation, and the family counselling and psychiatric referral pathway.
WHY THIS MATTERS
The medico-legal and psychosocial dimensions of poisoning are as important as the clinical management, yet they are often neglected in medical training. India has one of the world's highest rates of death from poisoning — agricultural pesticides, medications, and household chemicals are the most common agents — and a large proportion involve deliberate self-harm. NMC competencies IM22.9 through IM22.13 address five essential skills: (IM22.9) recognising what a poison information centre does and when to contact one; (IM22.10) managing the medico-legal aspects of poisoning cases; (IM22.11) writing a medico-legal report at the SH level; (IM22.12) counselling the patient's family; and (IM22.13) identifying the indications for psychiatric consultation. These five competencies equip the junior doctor to function independently in the medico-legal, psychosocial, and system-navigation dimensions of poisoning care — dimensions that begin from the moment the patient arrives and continue after clinical stabilisation.
RECALL
From your forensic medicine and ethics teaching, recall the medico-legal case (MLC) framework: any case where injury or disease may have legal consequences is an MLC — this includes poisoning (accidental, suicidal, or homicidal), assault, and road traffic accidents. A registered medical practitioner has a legal obligation under the Code of Medical Ethics and Indian law to treat the patient first, then report to the police. Recall the Indian Penal Code (IPC) provisions: Section 174 CrPC (mandatory post-mortem in unnatural deaths), Section 304A IPC (negligence causing death), and Section 309 IPC (attempt to suicide — now largely decriminalised under MHCA 2017). Recall from your community medicine posting: suicide attempts in India are classified as deliberate self-harm (DSH), and psychiatric evaluation is mandated under MHCA 2017 for all DSH admissions. Also recall that the Mental Healthcare Act 2017 Section 115 specifically provides that a person who attempts suicide shall be presumed to be under severe stress and shall not be tried and punished under Section 309 IPC.
Poison Information Centres: Functions and When to Call
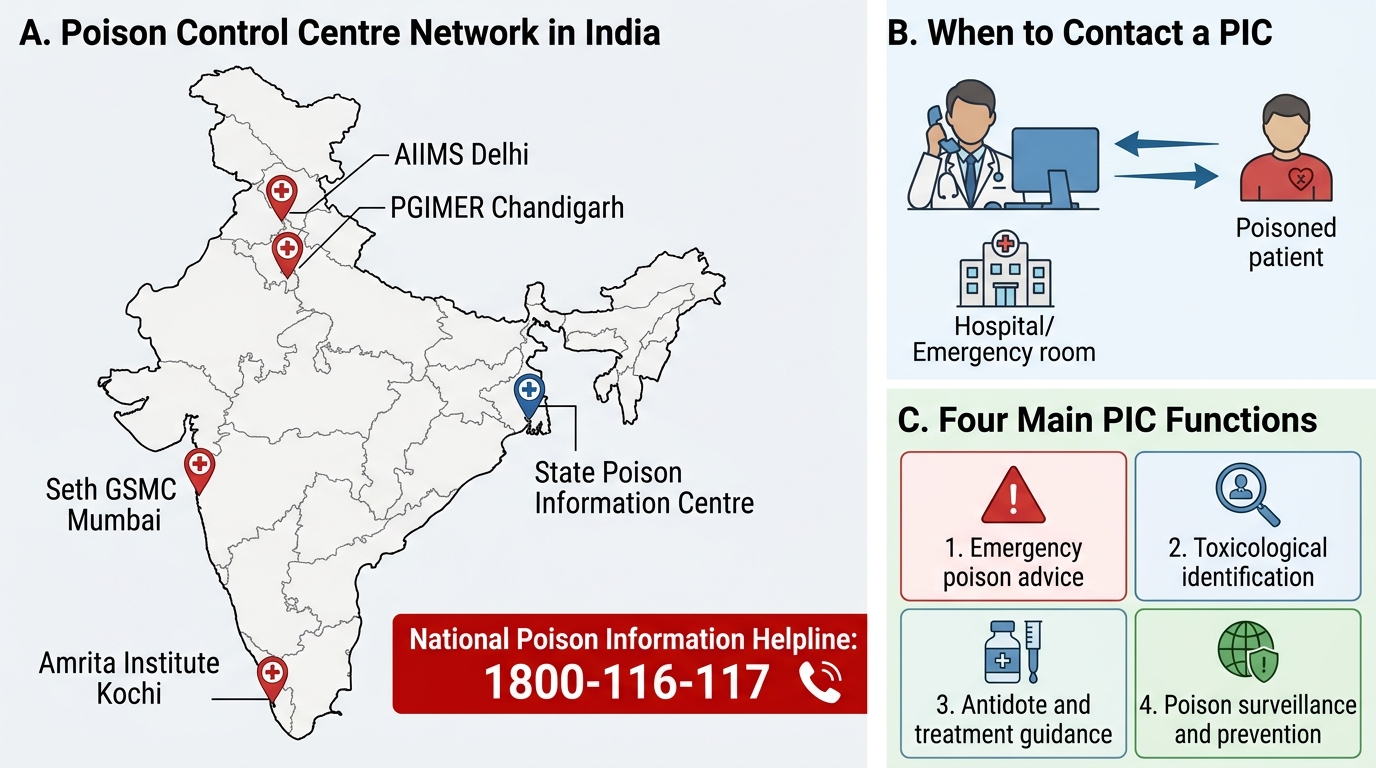
Poison information centres (PICs, also called poison control centres or toxicology advisory services) are specialised 24-hour services staffed by trained toxicologists and pharmacists who provide real-time advice on the management of poisoning cases. In India, a national network of PICs exists under the National Poison Control Centre (NPCC) umbrella, with major centres at AIIMS New Delhi, PGIMER Chandigarh, Amrita Institute of Medical Sciences (Kochi), Seth GSMC Mumbai, and government medical colleges in several states. These centres can be contacted by any treating clinician, including house officers, at any hour of the day or night. The National Poison Control helpline (India): 1800-116-117 (toll-free). Tamil Nadu Poison Control Hotline: 044-28193900 (PGIMER Chennai). Knowing how to access this resource is a clinical skill — knowing when to use it is equally important.
Functions of a poison information centre:
- Toxin identification: When the ingested substance is unknown, poorly labelled, or identified only by brand name, the PIC can help identify the active ingredient, likely toxidrome, and relative toxicity. Brand names of agricultural chemicals, household cleaners, and industrial chemicals are often unfamiliar to treating physicians — the PIC maintains databases of thousands of products.
- Management advice: The PIC provides specific guidance on antidotes, decontamination strategies (whether activated charcoal is appropriate for the specific agent), indications for specific interventions (e.g., dialysis for salicylates or methanol), and dose guidance for uncommon antidotes (e.g., pralidoxime dosing schedules, digoxin Fab dosing).
- Risk stratification: Not all ingestions require hospitalisation or aggressive intervention. The PIC can advise whether a specific dose of a specific agent in an otherwise healthy adult is likely to produce toxicity, or whether home observation is appropriate in a paediatric accidental ingestion (where the agent and amount ingested are known and non-toxic).
- Follow-up advice: Guidance on monitoring parameters, duration of observation, and when specific delayed toxicity is expected (e.g., delayed hepatotoxicity from paracetamol at 24–72 hours, delayed cardiac toxicity from aconitine).
When to call the poison information centre:
- Unknown substance ingested — PIC can help identify the toxin from product description, container, or available information
- Unusual or unfamiliar agent — agricultural chemicals, herbal preparations, mushroom ingestion
- Unusual clinical presentation inconsistent with the stated substance
- Guidance on rare or unfamiliar antidotes
- Paediatric poisoning (dose/weight-based risk stratification)
- Industrial accident or mass casualty involving chemical exposure
- Any case where the managing physician is uncertain about the appropriate treatment strategy
Poison Control Centres and PIC Functions in India
Medico-Legal Obligations in Poisoning Cases
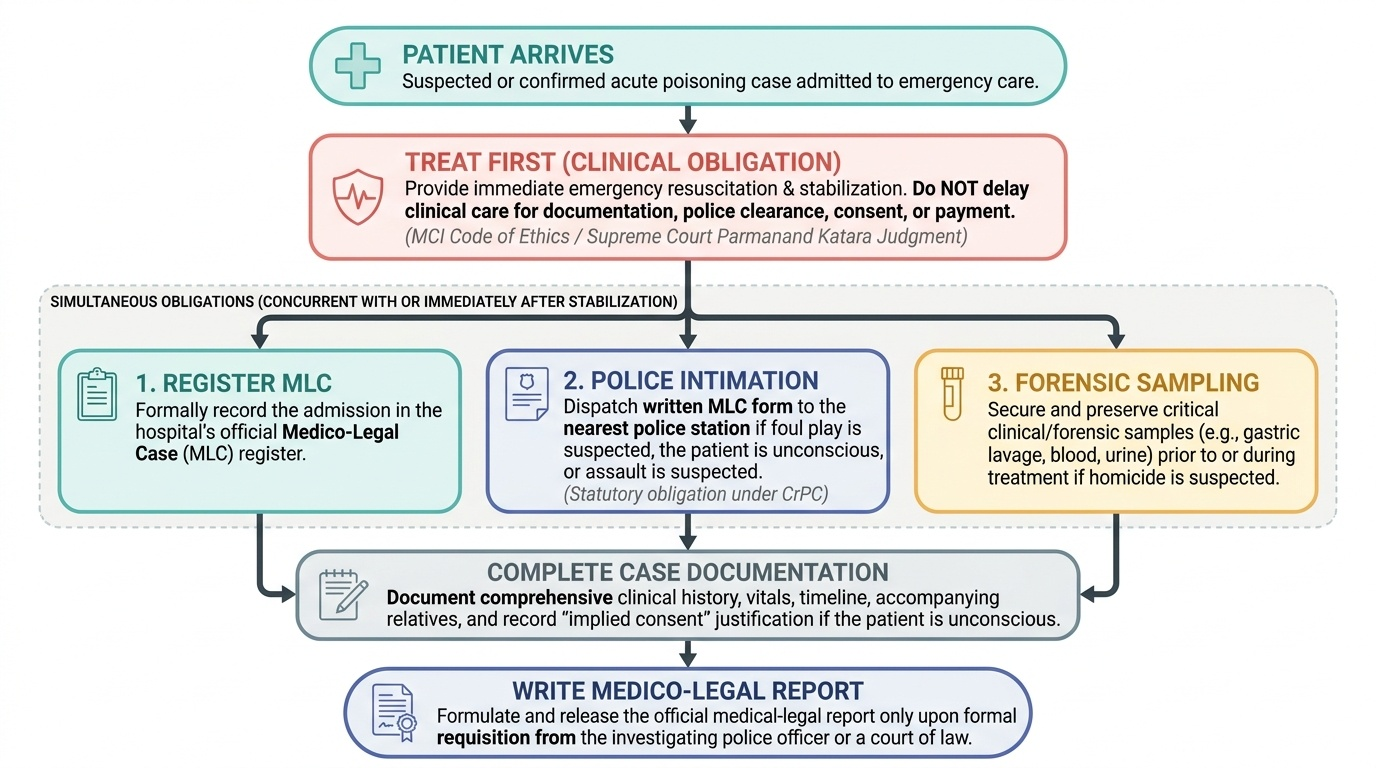
Every poisoning case admitted to a hospital in India is, by definition, a medico-legal case (MLC). The treating physician has both clinical and legal obligations that run in parallel and must not be confused — the clinical obligation (to treat and stabilise) always takes precedence, but the legal obligations must be fulfilled promptly after (or concurrently with) stabilisation. Failure to fulfil medico-legal obligations can have serious professional and legal consequences for the treating doctor, and can compromise the medico-legal investigation that may protect the patient or the public.
Provided image
Principle of treatment first: Under the Clinical Establishments Act, the Medical Council of India's Code of Medical Ethics, and Supreme Court judgments (Parmanand Katara v. Union of India, 1989), a physician MUST treat a medico-legal case patient first, regardless of police presence, consent issues, or availability of payment. No physician may withhold emergency treatment pending documentation, police clearance, or consent from a relative.
Mandatory police intimation:
In all cases of poisoning where foul play is suspected, or where the patient is unconscious and the circumstances of poisoning are unknown, or where the poisoning is the result of assault or administration by another person, the police MUST be informed. The mode is a written intimation (usually a standard MLC form maintained by the hospital) sent to the nearest police station. This is a statutory obligation under CrPC. The physician's role is to inform — not to investigate or to determine whether a crime has occurred. The police will decide whether to register an FIR. Important: police intimation is NOT required for all poisoning cases — it is required when there is a reason to suspect that the poisoning is not a straightforward accidental or self-harm case, or when the patient is incapacitated and circumstances are unclear.
Consent and documentation in unconscious patients:
When the patient is unconscious, consent cannot be obtained from the patient. Emergency consent is implied (implied consent doctrine — life-threatening emergency justifies treatment without explicit consent). Document all relatives present, their relationship to the patient, and any consent obtained for procedures. If no relative is present, document the absence and proceed with emergency treatment.
Preservation of evidence:
In suspected poisoning cases, the physician must take care not to destroy potential forensic evidence:
- Gastric aspirate/lavage fluid: collect a sample and label it clearly (date, time, patient ID, case number)
- Vomitus: collect a sample if available
- Clothing: handle minimally; preserve for police if assault is suspected
- Blood and urine: collect forensic samples at admission before any treatment if assault or homicide is suspected (a second set, clearly labelled 'forensic sample')
- IV fluid bags and drug vials: retain if accidental poisoning in a healthcare setting is suspected
Writing the Medico-Legal Report for Poisoning (SH Level)
A medico-legal report (MLR) for a poisoning case is a formal document that records the clinical findings, the investigation results, the treatment given, and the medical opinion regarding the nature and severity of the poisoning, in a format that is admissible as evidence in a court of law. At the SH (supervised house officer) level, you are expected to be able to write or contribute to an MLR under the supervision of a senior — which means you must understand its structure, the language conventions of medico-legal documentation, and the rules that distinguish a medical opinion from a legal conclusion. The key principle: the MLR states medical facts and medical opinions. The legal conclusion (whether a crime was committed, who did it) is for the court, not the physician.
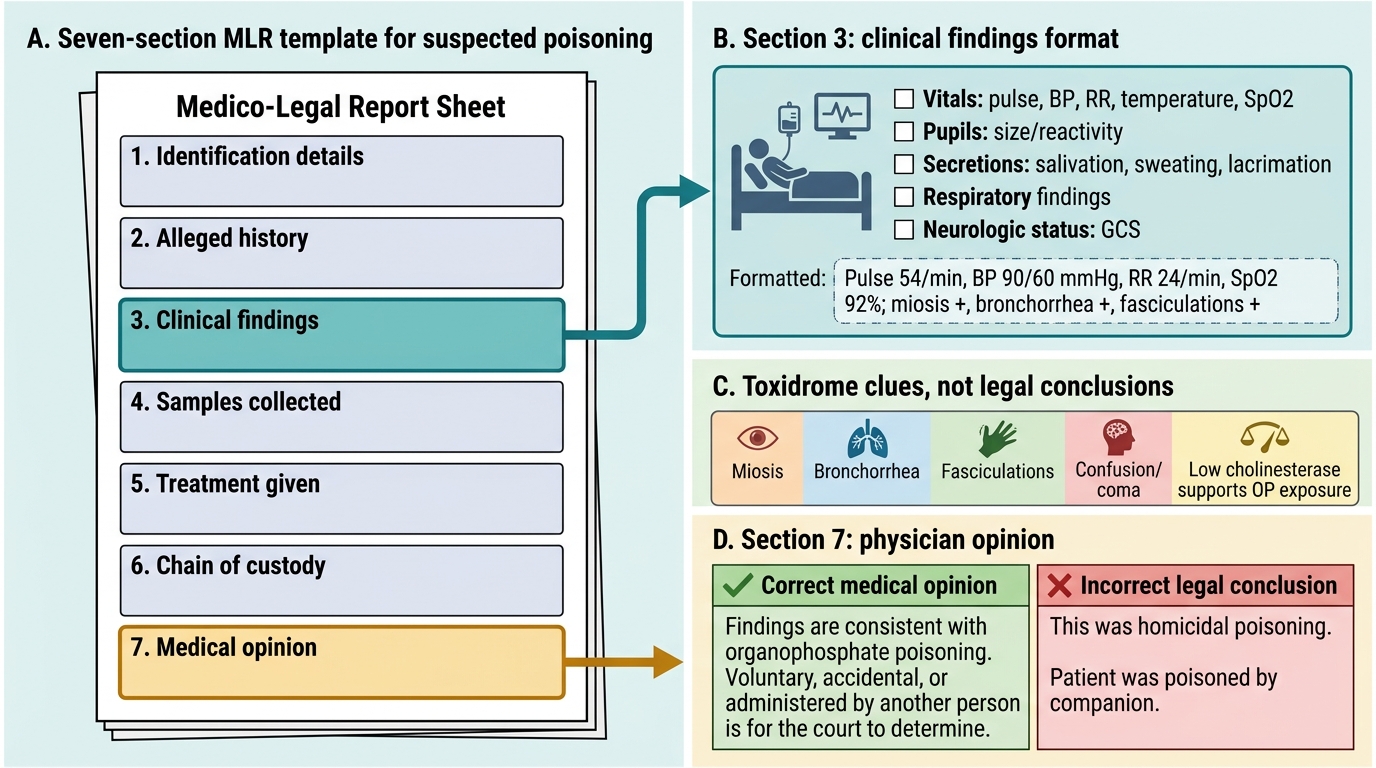
Standard structure of an MLR for poisoning:
Section 1 — Patient identification: Full name, age, sex, address, date and time of admission, hospital ID/MLC number, name of referring physician or police station (if police-referred).
Section 2 — History (as given by informants): The alleged circumstances of poisoning as told by the patient (if conscious) or relatives/police. State the SOURCE of the history — 'as stated by the patient' or 'as given by the attendant (relationship)'. Do NOT state these as facts; use passive voice: 'It was stated that...'
Section 3 — Clinical findings on admission: General condition, GCS score, vital signs (BP, pulse, RR, temperature, SpO₂), signs of poisoning specific to the toxidrome (pupil size and reactivity, skin findings, oral cavity, smell on breath, secretions, muscle fasciculations). Document the time of examination.
Section 4 — Investigations: List all relevant investigations with dates and results (ABG, renal function, LFT, ECG, serum drug levels where available, gastric aspirate sent for analysis, urine toxicology if done).
Section 5 — Treatment given: A clear chronological account of treatment — gastric lavage (time, amount of fluid used, character of return), activated charcoal (dose and time), antidotes administered (name, dose, route, time), supportive care given. This section is important for both clinical and legal purposes — it demonstrates that the standard of care was followed.
Section 6 — Progress and outcome: The patient's clinical course during admission; final diagnosis; prognosis and likely sequelae; whether forensic samples were collected and preserved.
Section 7 — Medical opinion: A clear statement of the physician's medical opinion — the nature of the poisoning (accidental/suicidal/homicidal as far as the medical evidence can suggest), the severity, whether the injuries/toxicity are consistent with the stated history, and any medical factors relevant to the legal investigation. Use precise language: 'In my medical opinion...' or 'The clinical findings are consistent with...' Avoid legal conclusions: do NOT write 'This was a murder' or 'She was forced to consume this substance' — these are legal conclusions, not medical opinions.
Language conventions in MLR writing:
- Use passive voice for history: 'it was alleged that', 'as stated by the patient'
- Use precise measurements, not qualitative estimates: '4 cm × 3 cm bruise on the right forearm' not 'a large bruise'
- Times must be exact: '14:35 hours on 05-06-2026' not 'afternoon'
- State what you observed, not what you inferred: 'pupils were 2 mm, bilaterally equal and reactive' not 'pupils showed organophosphate poisoning'
- Medical opinion section uses 'In my opinion...' or 'Based on my clinical examination and investigations...'
Medico-Legal Report Template for Suspected Poisoning
SELF-CHECK
You are asked to write a medico-legal report for a 30-year-old man admitted after drinking alcohol mixed with an unknown substance that caused him to collapse. The police want to know if a crime was committed. Which statement is CORRECT for the 'Medical Opinion' section of the MLR?
A. Write: 'In my medical opinion, the clinical and biochemical findings are consistent with organophosphate poisoning. Whether the compound was administered voluntarily, accidentally, or by another person is a matter for the court to determine.'
B. Write: 'This was a case of homicidal poisoning as the patient was found unconscious.'
C. Decline to write a medical opinion as you are only a house officer — wait for a consultant to sign the report
D. Write that the patient was poisoned by his companion, as the companion brought him to the hospital and appeared nervous
Reveal Answer
Answer: A. Write: 'In my medical opinion, the clinical and biochemical findings are consistent with organophosphate poisoning. Whether the compound was administered voluntarily, accidentally, or by another person is a matter for the court to determine.'
A medico-legal report from a physician must contain MEDICAL facts and MEDICAL opinion — not legal conclusions. Option A correctly states the clinical findings and the medical assessment of the type of poisoning, while explicitly deferring the legal question (was it homicidal, accidental, or suicidal?) to the court — which is the correct and legally safe approach. Option B commits the fundamental error of a legal conclusion in a medical report — 'homicidal' is a legal determination that only the court makes. Option C is wrong — an SH can write an MLR; the report must be counter-signed by the MO/registrar, but declining to write it is abandonment of a legal duty. Option D is wrong — nervousness of a companion is not a medical finding and cannot appear in an MLR as evidence of guilt.