Page 21 of 27
IM22.9-13 | Poison Centre and Medico Legal Workflow — SDL Guide (Part 3)
Self-Assessment: Medico-Legal Workflow for Poisoning
The following scenarios test your ability to apply all five competency domains covered in this module — poison centre use, medico-legal registration, MLR writing, family counselling, and psychiatric referral. Work through each scenario before reading the analysis.
Scenario 1: A 5-year-old child is brought in by a panicked parent after accidentally swallowing an unknown amount of a household cleaning product from under the sink. The child is alert and crying but not in distress. The parent cannot read the chemical name on the bottle (only the brand name is visible, and the managing team does not recognise it). What is the immediate action?
Analysis: Call the poison information centre immediately (1800-116-117). Give the brand name and the approximate quantity ingested. The PIC will identify the active ingredient, assess the risk for this approximate dose and body weight in a child, and advise whether activated charcoal, gastric lavage, or watchful waiting is appropriate. This is a textbook indication for PIC contact — unknown substance, paediatric patient, dose-risk assessment needed.
Scenario 2: A 55-year-old man is brought unconscious to the emergency department by a friend. The friend states he 'drank something' at a social gathering but does not know what. On examination: miosis, bradycardia, secretions, fasciculations (cholinergic toxidrome). The friend is the only person present. Is this an MLC, and should police be informed?
Analysis: Yes — all poisoning cases are MLCs. Police intimation is indicated in this case because the patient is unconscious, the circumstances of the poisoning are unknown, and a second person (the friend) was involved whose account needs to be verified. Register the MLC, send the police intimation, collect gastric lavage fluid as a forensic sample, and document the friend's account as 'stated by the companion (name and relationship)' in the case notes. The clinical management (atropine, pralidoxime) proceeds in parallel — treatment first.
Scenario 3: A 17-year-old girl is admitted after swallowing 20 tablets of alprazolam. She is now conscious, GCS 15, haemodynamically stable on day 2. The ward sister tells you 'she can go home — she looks fine and her mother is here to collect her.' What is your response?
Analysis: She cannot be discharged without psychiatric assessment. MHCA 2017 mandates psychiatric consultation for all DSH cases before discharge. The ward sister's clinical assessment (looks fine) addresses physical stability only — it does not address suicide risk, underlying psychiatric illness, or the safety of the home environment. Initiate the psychiatric consultation today. Write the referral: DSH (intentional alprazolam ingestion), patient is now alert and conversant, specific questions: suicide risk assessment, is discharge safe, does she require inpatient psychiatric admission? Tell the mother clearly and kindly: 'Your daughter is physically much better. Before she goes home, we need one more evaluation — a psychiatrist will speak with her today. This is a routine part of her medical care and is required by law. It is not a sign that she is 'mad'; it is to make sure she has the right support going forward.'
Medico-Legal Workflow in Poisoning
CLINICAL PEARL
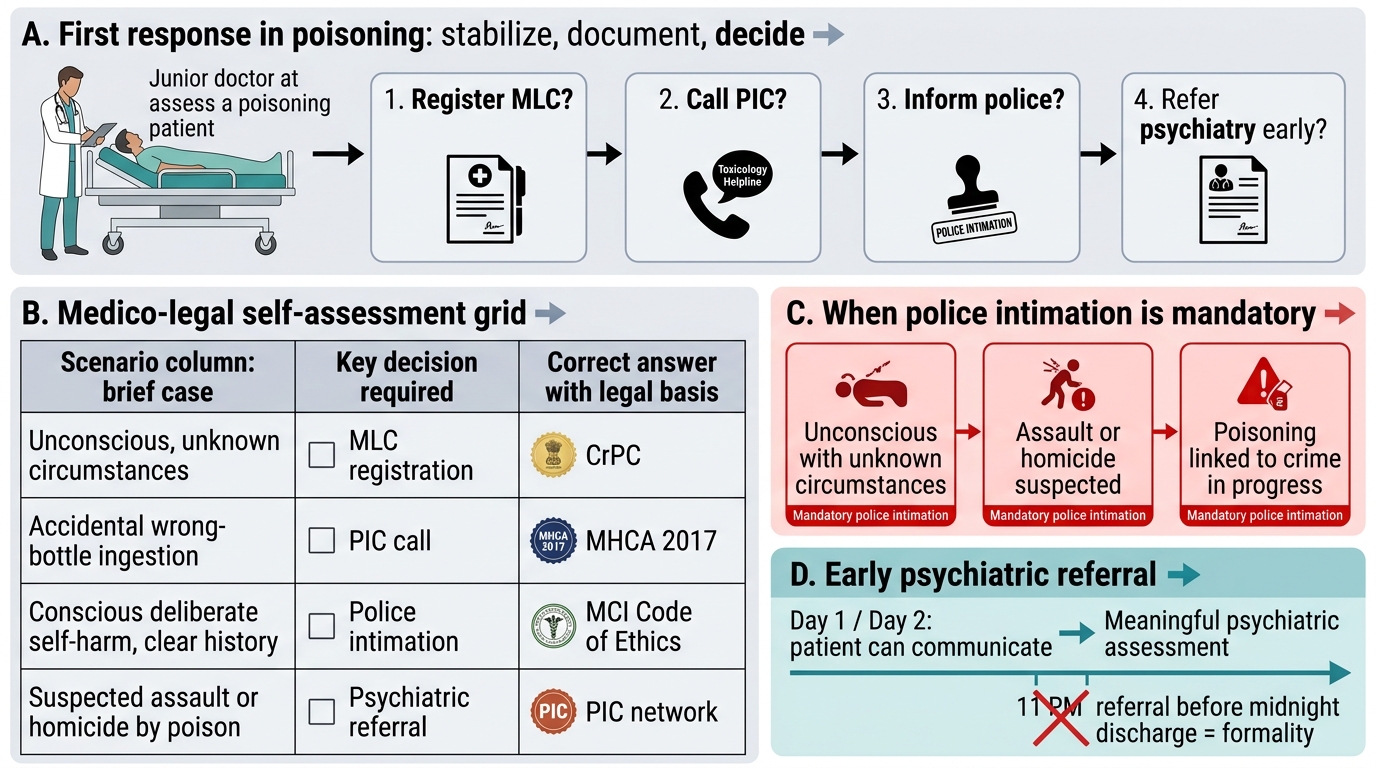
In India, the most common question a junior doctor asks about medico-legal cases is: 'Do I have to call the police?' The answer is context-specific. You MUST inform the police when: the patient is brought in unconscious with unknown circumstances; when assault or homicide by poison is suspected; when the poisoning is connected to a crime in progress. You are NOT required to call the police for: straightforward accidental poisoning (the family member who accidentally drank the wrong bottle); DSH cases where the patient is conscious and circumstances are clear (the patient confirms it was self-harm in a stable setting) — in these cases, police intimation is not mandatory, though it varies by hospital protocol.
For psychiatric referral: initiate it early — do not wait until the patient is being prepared for discharge. A psychiatric referral written at 11 PM when the patient is being discharged at midnight is not a referral; it is a formality. Early referral (day 1 or day 2 when the patient can communicate) gives the psychiatrist enough time for a meaningful assessment.