Page 2 of 27
IM22.{1,5} | Poisoning Stabilisation and Toxidromes — SDL Guide (Part 2)
Decontamination Principles and Enhanced Elimination
Decontamination refers to measures that reduce the amount of toxin available for absorption into the systemic circulation. It is most effective when instituted within the first 1–2 hours of ingestion and must never be attempted at the expense of ABC stabilisation. The decontamination strategy must be matched to the toxin and route of exposure; inappropriate decontamination can cause more harm than the poison itself.
Activated charcoal (AC) is the most widely used gastrointestinal decontaminant and remains the cornerstone of oral poison management. Activated charcoal is a highly porous, adsorptive substance produced by burning carbonaceous material (usually coconut shell) at high temperatures in the absence of oxygen. Its enormous surface area (900–2000 m²/g) adsorbs most organic toxins by Van der Waals forces, preventing their absorption through the gastrointestinal mucosa. The standard adult dose is 50 g (1 g/kg in children) mixed in water and given orally or via nasogastric tube. Indications: oral ingestion of adsorbed toxins within 1 hour of ingestion; consider up to 2 hours for toxins that delay gastric emptying (anticholinergics, modified-release preparations, opioids). Contraindications: unprotected airway (aspiration risk — must intubate first); ingestion of corrosives (acid, alkali — charcoal does not adsorb corrosives and masks endoscopic assessment); hydrocarbons (aspiration pneumonitis risk); and elemental metals (iron, lithium — poorly adsorbed). Activated charcoal does NOT adsorb: iron, lithium, potassium, fluoride, cyanide, alcohols, or mineral acids and alkalis.
Multiple-dose activated charcoal (MDAC) — repeated doses of 25–50 g every 4 hours — is used for toxins that undergo enterohepatic recirculation (carbamazepine, quinine, phenobarbital, dapsone, theophylline) or have prolonged absorption phases. The mechanism is "gut dialysis" — AC in the gut lumen acts as a sink for toxin that has already been absorbed and is secreted back into the GI lumen via enterohepatic cycling.
Gastric lavage — previously widely practised — is now used rarely and selectively. It is considered only when: the patient presents within 1 hour of ingesting a life-threatening amount of a toxin not adsorbed by AC (e.g., iron tablets) and the airway is protected (GCS normal or patient intubated). Contraindications: corrosive ingestion, unprotected airway, hydrocarbon ingestion. Inducing emesis (ipecac syrup) is no longer recommended in any scenario — the risk of aspiration and its delay of AC administration outweigh any benefit.
Dermal decontamination: Remove all contaminated clothing (wear gloves — healthcare worker protection) and wash the skin thoroughly with soap and water for at least 15 minutes. Critical for organophosphate, corrosive, and many industrial chemical exposures. Eye exposure: immediate irrigation with large volumes of normal saline or water for at least 20–30 minutes; slit-lamp examination after irrigation for corrosive injury.
Enhanced elimination refers to measures that accelerate removal of already-absorbed toxin from the body. The main strategies are:
- Urinary alkalinisation (sodium bicarbonate IV to raise urine pH > 7.5): increases renal clearance of weak acids — particularly salicylates (aspirin) and phenobarbital — by ion trapping (ionised drug cannot diffuse back across tubular epithelium). Requires normal renal function and careful monitoring of serum potassium.
- Haemodialysis: removes water-soluble, low-molecular-weight, low-protein-bound toxins. Indications include: methanol and ethylene glycol poisoning with metabolic acidosis (definitive treatment when fomepizole is unavailable), severe salicylate toxicity, severe lithium toxicity, and valproate toxicity with coma. Haemoperfusion (blood passed through activated charcoal column) is used for theophylline and carbamazepine poisoning where dialysis is less effective.
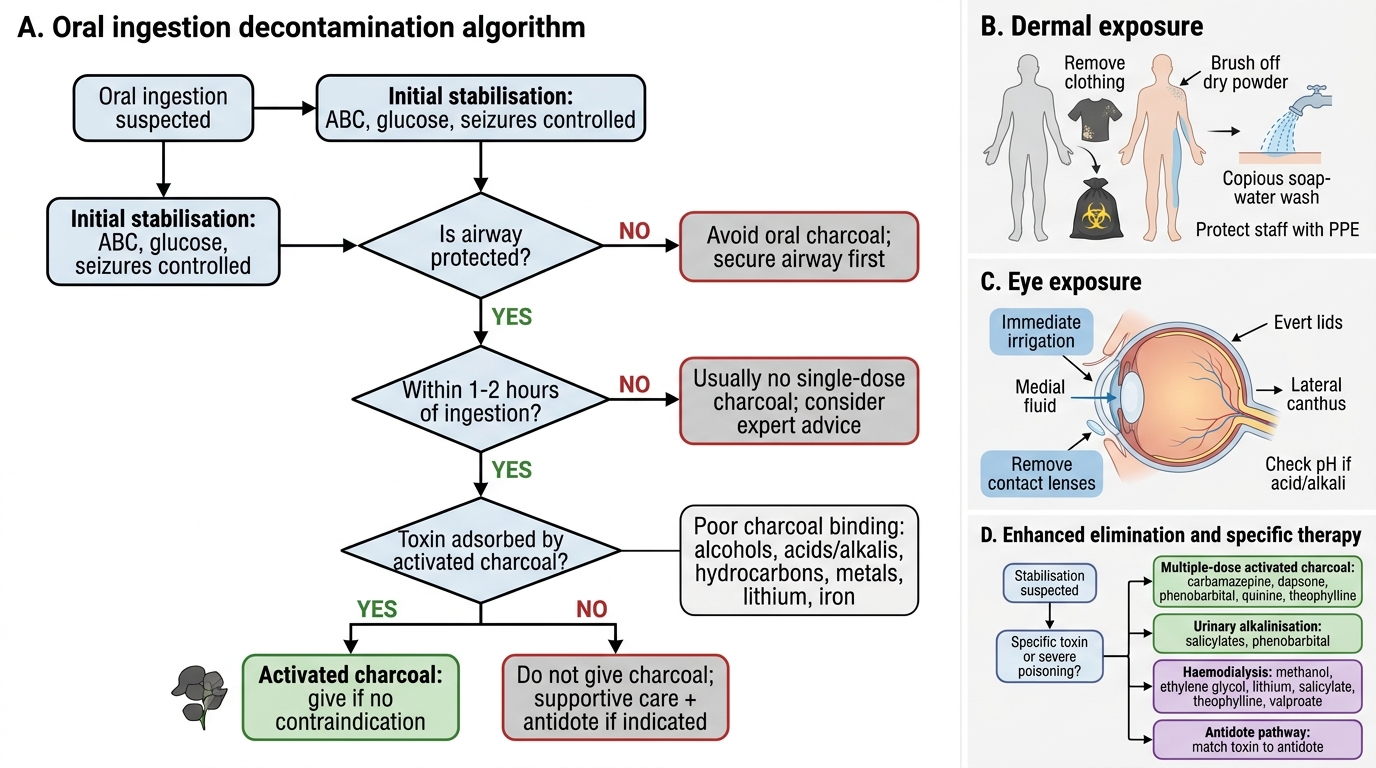
Poisoning Decontamination Decision Algorithm
Management of Specific Toxidromes: Antidote Matching
Beyond initial stabilisation and decontamination, the definitive management of poisoning hinges on two axes: specific antidote administration where an antidote exists, and meticulous supportive care where it does not. Supportive care — airway protection, haemodynamic support, correction of electrolyte and acid-base disturbances, seizure management, thermoregulation, and prevention of complications — remains the backbone of poisoning management for the majority of toxins for which no antidote exists.
Provided image
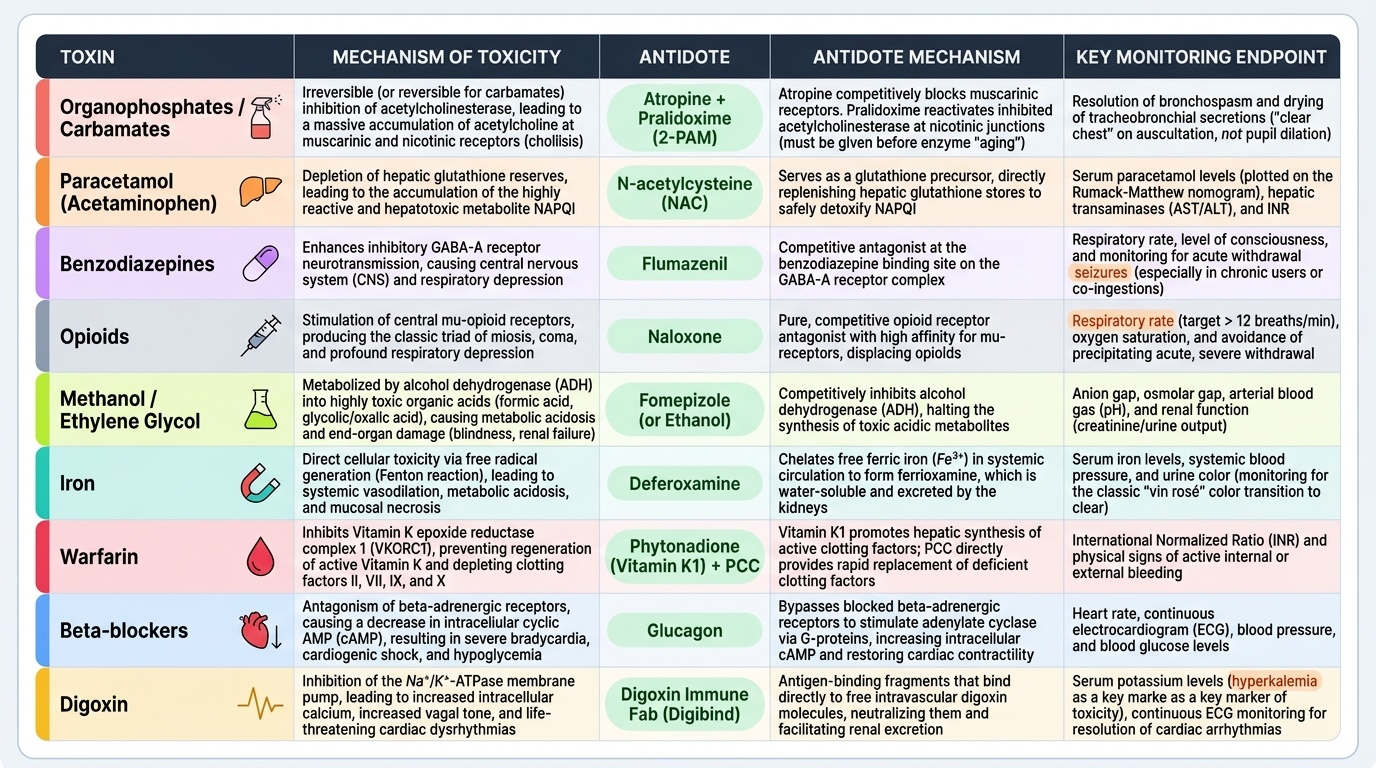
The following antidote-toxin pairings represent the most clinically urgent associations that must be memorised at the level of conditioned reflex. Each delay in antidote administration directly increases morbidity and mortality.
Organophosphate/carbamate → Atropine + Pralidoxime. Atropine blocks muscarinic receptors, drying secretions and reversing bradycardia and bronchospasm. It must be given in large, repeated doses — starting at 2–4 mg IV and doubling every 5 minutes until secretions dry (not pupils dilate — the endpoint is dry secretions and clear chest). Pralidoxime (1–2 g IV over 15–30 minutes) reactivates inhibited cholinesterase at nicotinic junctions if given before the enzyme-inhibitor bond becomes irreversible ("ageing" — occurs within hours for most OPs, within minutes for some compounds like soman).
Paracetamol → N-acetylcysteine (NAC). NAC is a glutathione precursor that replenishes hepatic glutathione, preventing accumulation of the toxic metabolite NAPQI. The Rumack-Matthew nomogram plots serum paracetamol concentration against time post-ingestion to determine whether NAC is required. Start NAC if serum paracetamol level falls above the treatment line (approximately 150 mg/L at 4 hours post-ingestion). Standard regimen: IV NAC 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours. Oral NAC (1330 mg/kg total over 72 hours) is an alternative when IV is unavailable.
Benzodiazepine → Flumazenil. A competitive GABA-A receptor antagonist. Use 0.2 mg IV, repeat every 60 seconds to a maximum of 1 mg. Caution: precipitates acute withdrawal in BZD-dependent patients; dangerous if BZDs were co-ingested with proconvulsants (TCAs) — reversal of sedation may unmask TCA-induced seizures. Its short half-life means re-sedation is common.
Opioid → Naloxone. Pure μ-opioid receptor antagonist. Dose 0.4–2 mg IV/IM/intranasal; repeat every 2–3 minutes; maximum 10 mg. If no response to 10 mg, the diagnosis of opioid toxidrome should be reconsidered. In opioid-dependent patients, titrate to restore ventilation — abrupt reversal precipitates acute withdrawal with vomiting, agitation, and pulmonary oedema.
Methanol/Ethylene glycol → Fomepizole (preferred) or Ethanol. Both agents competitively inhibit alcohol dehydrogenase (ADH), preventing conversion of methanol to formic acid and ethylene glycol to glycolic/oxalic acid — the toxic metabolites responsible for optic toxicity and nephrotoxicity, respectively. Fomepizole 15 mg/kg IV is the preferred antidote. Ethanol (oral or IV to achieve blood ethanol concentration ~100 mg/dL) is the alternative when fomepizole is unavailable (common in India). Haemodialysis is required when metabolic acidosis is present, renal failure ensues, or serum levels are very high.
Iron → Desferrioxamine (deferoxamine). An iron chelator that binds free ferric iron and excretes it in urine (as ferrioxamine — which turns the urine "vin rosé" colour, a useful monitoring sign). Indications: serum iron > 500 mcg/dL or ≥ 350 with systemic symptoms (shock, coma, severe acidosis). Dose: continuous IV infusion up to 15 mg/kg/hour, maximum 80 mg/kg/day.
Warfarin/anticoagulant overdose → Vitamin K + Prothrombin Complex Concentrate (PCC) or Fresh Frozen Plasma (FFP). Vitamin K₁ (phytomenadione) 10 mg IV/oral reverses warfarin's anti-vitamin K effect over 6–24 hours. For immediate reversal in active bleeding, 4-factor PCC (Octaplex) or FFP provides immediate clotting factor replacement while vitamin K takes effect.
Beta-blocker overdose → Glucagon. Glucagon activates adenylyl cyclase via a non-adrenergic receptor pathway, bypassing the blocked beta-receptor and restoring cardiac contractility and rate. Dose: 3–5 mg IV bolus, then 3–5 mg/hour infusion. High-dose insulin-euglycaemia therapy is an emerging alternative for severe CCB and beta-blocker poisoning.
Digoxin toxicity → Digoxin-specific Fab antibody fragments (Digibind/DigiFab). Each vial (38 mg) binds 0.5 mg of digoxin. Calculate dose from serum digoxin level or estimated ingested amount. Indicated for: life-threatening arrhythmias, serum digoxin > 10 ng/mL, hyperkalaemia (> 5.5 mEq/L) in digitalis toxicity.
SELF-CHECK
A 19-year-old student presents 6 hours after ingesting approximately 25 tablets of paracetamol 500 mg. She is fully conscious, pulse 88 bpm, BP 120/80 mmHg, no jaundice. Serum paracetamol level is 180 mg/L at 6 hours post-ingestion. According to the Rumack-Matthew nomogram, she falls ABOVE the treatment line. Which treatment should be started immediately?
A. Activated charcoal 50 g and observation only
B. N-acetylcysteine IV infusion protocol
C. Flumazenil 0.2 mg IV
D. Haemodialysis for paracetamol clearance
Reveal Answer
Answer: B. N-acetylcysteine IV infusion protocol
A serum paracetamol of 180 mg/L at 6 hours post-ingestion falls above the Rumack-Matthew nomogram treatment line (approximately 150 mg/L at 4 hours; lower at later time points). Intravenous N-acetylcysteine must be started immediately — it replenishes glutathione, prevents accumulation of NAPQI, and is effective in preventing hepatic necrosis up to 8–12 hours post-ingestion (and sometimes up to 24 hours). Activated charcoal alone is insufficient at 6 hours. Flumazenil is for benzodiazepine overdose. Haemodialysis is not indicated for paracetamol poisoning unless there is already established acute liver failure with encephalopathy.
Self-Assessment: Applying the Toxidrome Framework
The self-assessment section tests your ability to integrate the stabilisation approach, toxidrome recognition, and antidote knowledge into a clinical decision-making sequence. For each scenario, work through the assessment before reading the analysis. This mirrors the NMC IM22.1 and IM22.5 competencies, which require you to apply both stabilisation logic and toxidrome recognition to a patient encounter.
Scenario A: A 22-year-old man is brought in from a farming community, unconscious. Examination reveals: GCS 6, pulse 36 bpm, BP 60/30 mmHg, respiratory rate 6/min with copious frothy secretions from the mouth, pupils 1 mm bilaterally, visible fasciculations of the deltoids, and he is incontinent of urine and faeces. His accompanying family confirm he was working in the fields spraying pesticide this morning. Describe the toxidrome, immediate stabilisation priorities, and antidote regimen.
Analysis: Cholinergic toxidrome — SLUDGE features + bradycardia + bronchorrhoea + miosis + nicotinic fasciculations. Cause: organophosphate insecticide. Stabilisation: (1) Protect airway — GCS 6 + copious secretions = imminent aspiration, prepare for intubation but give atropine IV first to reduce secretions. (2) Atropine 2–4 mg IV stat; repeat every 5 minutes doubling the dose until secretions dry. Do NOT use 0.6 mg ampules — inadequate dosing is the leading cause of preventable death. (3) Pralidoxime 1–2 g IV over 30 minutes, ideally within 6–8 hours. (4) IV fluids for hypotension. (5) Benzodiazepines for seizures. (6) Dermal decontamination after airway secured. Remove clothing, wash skin.
Scenario B: An 18-year-old woman is brought by her mother, agitated, confused, and saying strange things. Mother reports she found her having eaten some wild berries from the garden before this started. Examination: HR 134 bpm, BP 150/90 mmHg, temperature 38.8°C, pupils 8 mm bilaterally and fixed, skin flushed and completely dry, no bowel sounds, urinary retention. She is pulling at her clothes and hallucinating. Identify the toxidrome and causative agent family.
Analysis: Anticholinergic toxidrome — tachycardia, hyperthermia, MYDRIASIS (not miosis), dry flushed skin (no secretions — key differentiator from cholinergic), agitation, hallucinations, urinary retention, absent bowel sounds. Cause: Datura stramonium (jimsonweed/dhatura berries) containing atropine and scopolamine. Management: supportive cooling, benzodiazepines for agitation, urinary catheter for retention, IV fluids. Physostigmine 1–2 mg slow IV may be considered for severe delirium or life-threatening anticholinergic features but requires cardiac monitoring (contraindicated in TCA co-ingestion).
Scenario C: A 45-year-old man is found unresponsive at home. No history available. On examination: GCS 4, respiratory rate 4/min, oxygen saturation 84%, blood pressure 90/60 mmHg, pupils 2 mm bilaterally and reactive, no excessive secretions, no fasciculations, no diaphoresis. There are track marks (injection sites) on both forearms. Identify toxidrome and immediate priority treatment.
Analysis: Opioid toxidrome — the triad of miosis + respiratory depression + coma. Track marks suggest IV opioid use. Immediate priority: (1) Establish airway — bag-valve-mask ventilation while preparing naloxone. (2) Naloxone 0.4–2 mg IV/IM/intranasal stat. (3) Repeat naloxone every 2–3 minutes, monitoring SpO₂ and level of consciousness. (4) If no response after 10 mg naloxone, reconsider diagnosis — may have mixed ingestion or hypoglycaemia. (5) Arrange naloxone infusion if response achieved (drug half-life of naloxone is shorter than most opioids).
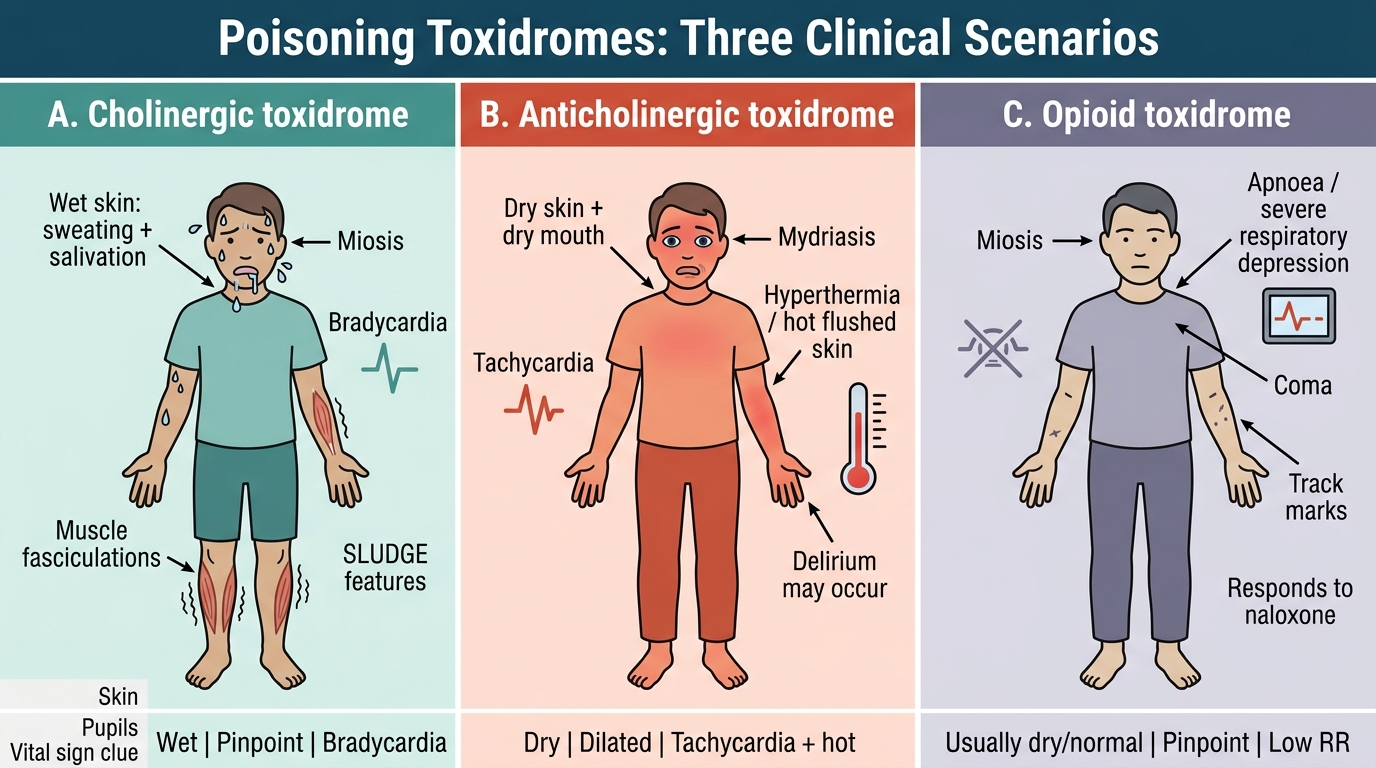
Poisoning Toxidromes: Key Differentiating Features
SELF-CHECK
A 28-year-old woman is brought unconscious after taking an overdose of sleeping tablets and a bottle of cough syrup. Her pupils are 2.5 mm, responsive to light; BP 90/60 mmHg; RR 8/min; temperature 36.1°C; no muscle fasciculations; skin is neither wet nor excessively dry. After giving naloxone 2 mg IV with no response, which toxidrome is MOST likely and what is the specific antidote?
A. Cholinergic — give atropine
B. Sympathomimetic — give benzodiazepines
C. Sedative-hypnotic — give flumazenil
D. Anticholinergic — give physostigmine
Reveal Answer
Answer: C. Sedative-hypnotic — give flumazenil
The sedative-hypnotic toxidrome is characterised by CNS depression (coma), respiratory depression, near-normal pupils (2.5 mm — not pinpoint as in opioid toxidrome), hypotension, and hypothermia/normothermia, with NO fasciculations and NEITHER dry nor diaphoretic skin. The sleeping tablets suggest benzodiazepine ingestion. No response to naloxone excludes opioid toxidrome. The specific antidote for benzodiazepine toxidrome is flumazenil (0.2 mg IV, repeatable). Caution: do not give flumazenil if tricyclics were co-ingested. Cholinergic toxidrome has wet SLUDGE features. Sympathomimetic causes agitation, tachycardia, hypertension, diaphoresis. Anticholinergic has dry flushed skin and mydriasis.
CLINICAL PEARL
The greatest single danger in managing the poisoned patient is under-dosing atropine in organophosphate poisoning. Students — and even house officers — often give 0.6 mg and wait for improvement. The correct endpoint for atropine titration is drying of secretions and clearance of pulmonary wheeze — NOT pupil dilation (pupils may not dilate even with adequate atropinisation) and NOT heart rate (tachycardia is not the goal). Patients with severe organophosphate poisoning may require hundreds of milligrams of atropine over 24–48 hours. There is no upper dose limit in cholinergic crisis — you stop when the endpoint (dry secretions) is achieved and restart when secretions return.
A second pearl: the toxidrome framework assumes pure poisoning. Organophosphate is the classic example of a toxin that causes BOTH muscarinic (SLUDGE + bradycardia) AND nicotinic (fasciculations + paralysis) features — atropine covers the muscarinic side but does nothing for the neuromuscular paralysis. This is why atropine alone is insufficient and pralidoxime must be added to address the nicotinic (NMJ) component.