Page 17 of 27
IM22.8 | Toxic Alcohol Poisoning — SDL Guide (Part 2)
Management: ADH Inhibition, Folate, and Haemodialysis
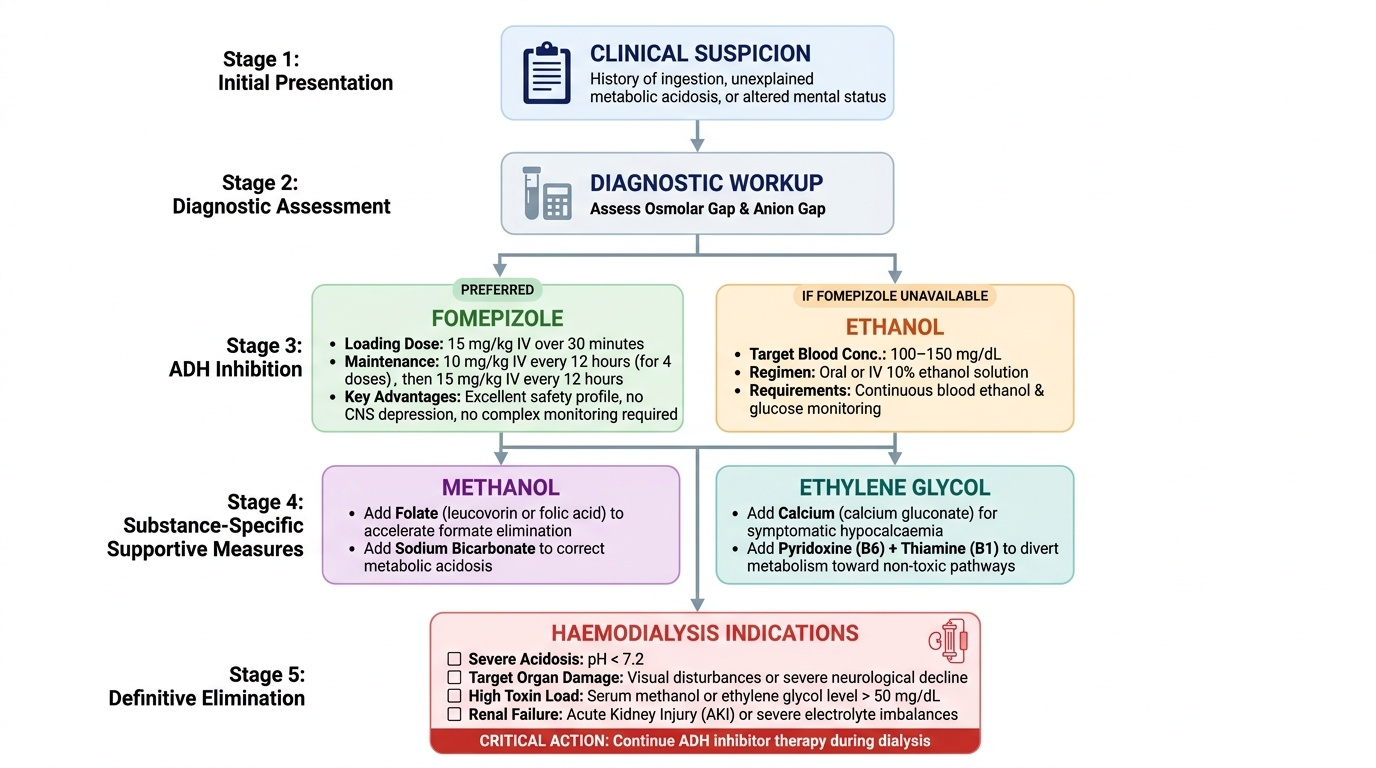
The management of methanol and ethylene glycol poisoning rests on a logical three-part strategy derived directly from the metabolic pathways: (1) block ADH to prevent further generation of toxic metabolites; (2) accelerate excretion of the parent alcohol and its metabolites by haemodialysis; and (3) provide specific supportive measures for the complications that have already developed (metabolic acidosis, optic nerve toxicity, renal failure, hypocalcaemia). Every component of this strategy is pharmacologically rational — the clinician who understands the pathway can derive the treatment without memorisation. The urgency of treatment is directly proportional to the metabolic severity: early treatment (before significant metabolite accumulation) can prevent organ damage entirely; late treatment (after formate or oxalate has caused irreversible injury) can only limit further damage.
Provided image
1. Inhibit alcohol dehydrogenase (ADH) — the primary antidote strategy:
Fomepizole (4-methylpyrazole): A potent, competitive inhibitor of ADH. It prevents conversion of methanol to formaldehyde/formate and ethylene glycol to glycolaldehyde/glycolate. Fomepizole is the preferred antidote: dose 15 mg/kg IV over 30 minutes (loading), then 10 mg/kg every 12 hours for four doses, then 15 mg/kg every 12 hours thereafter. Advantages over ethanol: does not cause CNS depression, does not require complex monitoring, no hypoglycaemia risk, can be used in children. Disadvantage: expensive and not available in most Indian hospitals outside major academic centres.
Ethanol: When fomepizole is unavailable (the common situation in Indian district hospitals), ethanol competes with methanol and ethylene glycol for ADH (ethanol has much higher ADH affinity — about 10–20× higher than methanol; and 100× higher than ethylene glycol). By saturating ADH with ethanol, the toxic alcohols are not metabolised and are excreted unchanged by the kidney and exhaled via the lungs. Target blood ethanol concentration: 100–150 mg/dL (approximately equivalent to moderate intoxication). Regimen: oral or IV 10% ethanol solution, adjusted to maintain the target concentration. Requires continuous blood ethanol monitoring and glucose monitoring (ethanol causes hypoglycaemia, especially in children and malnourished adults). Ethanol antidote must be continued until the methanol or ethylene glycol has been eliminated — this means continuous administration for 24–72 hours, often including during haemodialysis (dialysis removes ethanol rapidly, requiring dose adjustment).
Indications for ADH inhibitor therapy: suspected methanol or ethylene glycol poisoning with elevated osmolar gap, high anion gap metabolic acidosis, or consistent clinical features — do not wait for serum levels if not available; treat on clinical grounds.
2. Adjunctive measures:
For methanol poisoning specifically:
- Folate (leucovorin/folinic acid or folic acid): The endogenous formate detoxification pathway is folate-dependent. Administer folic acid 50 mg IV every 4–6 hours (or folinic acid/leucovorin 1 mg/kg, maximum 50 mg, IV every 4–6 hours) — this enhances the conversion of formate to CO₂ + H₂O and accelerates clearance of the toxic metabolite. Folic acid is inexpensive, safe, and available everywhere. It should be given to all methanol-poisoned patients.
- Sodium bicarbonate: For severe metabolic acidosis (pH < 7.1 or HCO₃ < 5 mEq/L) — maintain pH > 7.2 to limit the non-ionic form of formic acid that crosses into the optic nerve (un-ionised formic acid at low pH crosses the blood-brain and blood-retinal barriers more readily than ionised formate at normal pH).
For ethylene glycol poisoning specifically:
- Calcium gluconate or calcium chloride for severe symptomatic hypocalcaemia (tetany, seizures, QTc > 500 ms). Caution: do not give calcium to prevent oxalate formation — it does not reduce oxalate production and may worsen systemic calcium oxalate deposition.
- Pyridoxine (vitamin B6) and thiamine (vitamin B1): May enhance alternative metabolic pathways for ethylene glycol that bypass the toxic oxalate pathway. Given as adjuncts (pyridoxine 100 mg IV, thiamine 100 mg IV every 6 hours) with little harm and possibly some benefit.
3. Haemodialysis:
Haemodialysis is the definitive means of removing the toxic alcohol and its metabolites from the body, and correcting severe metabolic acidosis. It is far faster than renal excretion alone. The decision to dialyse is driven by clinical and metabolic severity, not only by serum level (which may not be available).
Indications for haemodialysis in methanol poisoning:
- Serum methanol > 50 mg/dL (if available)
- Severe metabolic acidosis (pH < 7.2 despite bicarbonate) or HCO₃ < 5 mEq/L
- Visual disturbance (any degree) — optic nerve toxicity is an emergency indication; dialysis removes formate and may prevent progression to blindness
- Renal failure
- Any deteriorating clinical status despite ADH inhibitor therapy
Indications for haemodialysis in ethylene glycol poisoning:
- Serum ethylene glycol > 50 mg/dL (if available)
- Metabolic acidosis (pH < 7.25)
- AKI (rising creatinine or oliguria)
- Refractory hypocalcaemia
During haemodialysis, ADH inhibitor (ethanol or fomepizole) must be continued at increased dosing rate because dialysis removes both the ethanol (requiring dose adjustment to maintain the target 100–150 mg/dL blood level) and the toxic alcohol.
SELF-CHECK
A 35-year-old man is diagnosed with methanol poisoning at a district hospital. Serum methanol level is unavailable. ABG: pH 7.12, HCO₃ 5 mEq/L. He complains of blurred vision and can count fingers at 2 metres (markedly reduced visual acuity). Fomepizole is not available. Which management plan is CORRECT?
A. Give ethanol (oral or IV) to achieve blood ethanol 100-150 mg/dL, folate IV, sodium bicarbonate IV, and arrange urgent haemodialysis — visual disturbance and pH < 7.2 are both absolute indications for dialysis
B. Give activated charcoal 50 g and observe — methanol is well absorbed by charcoal
C. Give NAC IV as formate causes oxidative damage similar to NAPQI in paracetamol poisoning
D. Wait for serum methanol level before starting treatment — treatment must be guided by the level
Reveal Answer
Answer: A. Give ethanol (oral or IV) to achieve blood ethanol 100-150 mg/dL, folate IV, sodium bicarbonate IV, and arrange urgent haemodialysis — visual disturbance and pH < 7.2 are both absolute indications for dialysis
This patient has severe methanol poisoning: pH 7.12 (severe acidosis), HCO₃ 5 mEq/L, and visual disturbance (optic nerve formate toxicity — an absolute indication for haemodialysis). Fomepizole is unavailable; therefore ethanol is the ADH inhibitor of choice — target blood ethanol 100-150 mg/dL. Add folic acid IV (enhances formate detoxification). IV sodium bicarbonate for severe acidosis. Arrange urgent haemodialysis immediately — visual disturbance and pH < 7.2 both independently mandate dialysis; dialysis removes formate and methanol rapidly and is the only intervention that can prevent further optic nerve damage. Activated charcoal does not adsorb alcohols. NAC has no mechanism of action in methanol poisoning. Treatment must not wait for serum levels when clinical indications are clear.
Prognosis and Self-Assessment
The prognosis of toxic alcohol poisoning is directly related to the speed and completeness of ADH inhibition and the availability of haemodialysis — two variables that differ dramatically between a well-equipped tertiary centre and a rural district hospital in India. In methanol poisoning, the extent of optic nerve damage at the time of presentation is largely irreversible — permanent visual loss occurs in patients who have accumulated significant formate before treatment is initiated. Recovery of vision after methanol poisoning is possible when formate levels are intercepted early; the outcome worsens with every hour of delay. In ethylene glycol poisoning, renal failure can be reversed if haemodialysis is instituted before irreversible tubular necrosis occurs. The overall survival rate from methanol and ethylene glycol poisoning in well-resourced centres with prompt treatment is greater than 90%; in district hospital settings without fomepizole and with limited dialysis access, mortality and permanent visual impairment are substantially higher.
Key prognostic factors in methanol poisoning:
- Severity of metabolic acidosis at presentation (pH < 7.1 = very high mortality/morbidity)
- Degree of visual disturbance at presentation (any visual loss = high risk of permanent impairment without urgent dialysis)
- Serum formate level (> 20 mg/dL = severe toxicity; not routinely available)
- Time from ingestion to ADH inhibition (every hour without treatment = more formate accumulated)
The following cases test your application of toxic alcohol management:
Scenario A: A 45-year-old man from a hooch-affected village arrives alert, 4 hours after drinking home-brew. No visual symptoms yet. Osmolar gap = 22 mOsm/kg (elevated). ABG: pH 7.35, HCO₃ 20 mEq/L (mild metabolic component). He is relatively well. Should treatment be started immediately or observed?
Analysis: The elevated osmolar gap is the diagnostic key — this man has significant methanol in his blood (osmolar gap of 22 suggests approximately 35–40 mg/dL methanol). He is in the pre-metabolite phase (pH near-normal, no visual symptoms yet) because formate accumulation has not yet begun. This is the OPTIMAL window for ADH inhibitor therapy — starting fomepizole (or ethanol) NOW prevents formate from ever accumulating. Do not observe and wait for clinical deterioration. Start ethanol (or fomepizole if available) immediately to maintain blood ethanol > 100 mg/dL. Monitor serial ABGs and clinical status. Arrange dialysis preparation. The absence of acidosis and visual symptoms does NOT mean the danger has passed — it means the window for prevention is still open.
Scenario B: A 28-year-old woman is admitted 18 hours after ingesting antifreeze (ethylene glycol). She has flank pain, oliguria with output of 20 mL/hour, serum creatinine 3.8 mg/dL, calcium 1.6 mmol/L, urine dipstick positive for blood. Urine microscopy shows abundant calcium oxalate crystals. ABG: pH 7.20, HCO₃ 10 mEq/L. Outline the management.
Analysis: Stage 3 ethylene glycol poisoning — AKI (creatinine 3.8, oliguria, oxalate crystals in urine), hypocalcaemia (1.6 mmol/L), metabolic acidosis (pH 7.20). Management: (1) ADH inhibitor — start ethanol or fomepizole (even at 18 hours, any residual ethylene glycol is being metabolised; stopping ADH prevents further oxalate generation). (2) Calcium gluconate IV for symptomatic hypocalcaemia (tetany, QTc prolongation) — calcium 10 mL of 10% calcium gluconate IV slowly. (3) Pyridoxine and thiamine IV. (4) Sodium bicarbonate for pH 7.20. (5) Urgent haemodialysis — AKI + pH 7.20 are both indications; dialysis removes ethylene glycol, glycolate, and oxalate; also corrects acidosis and hypocalcaemia.
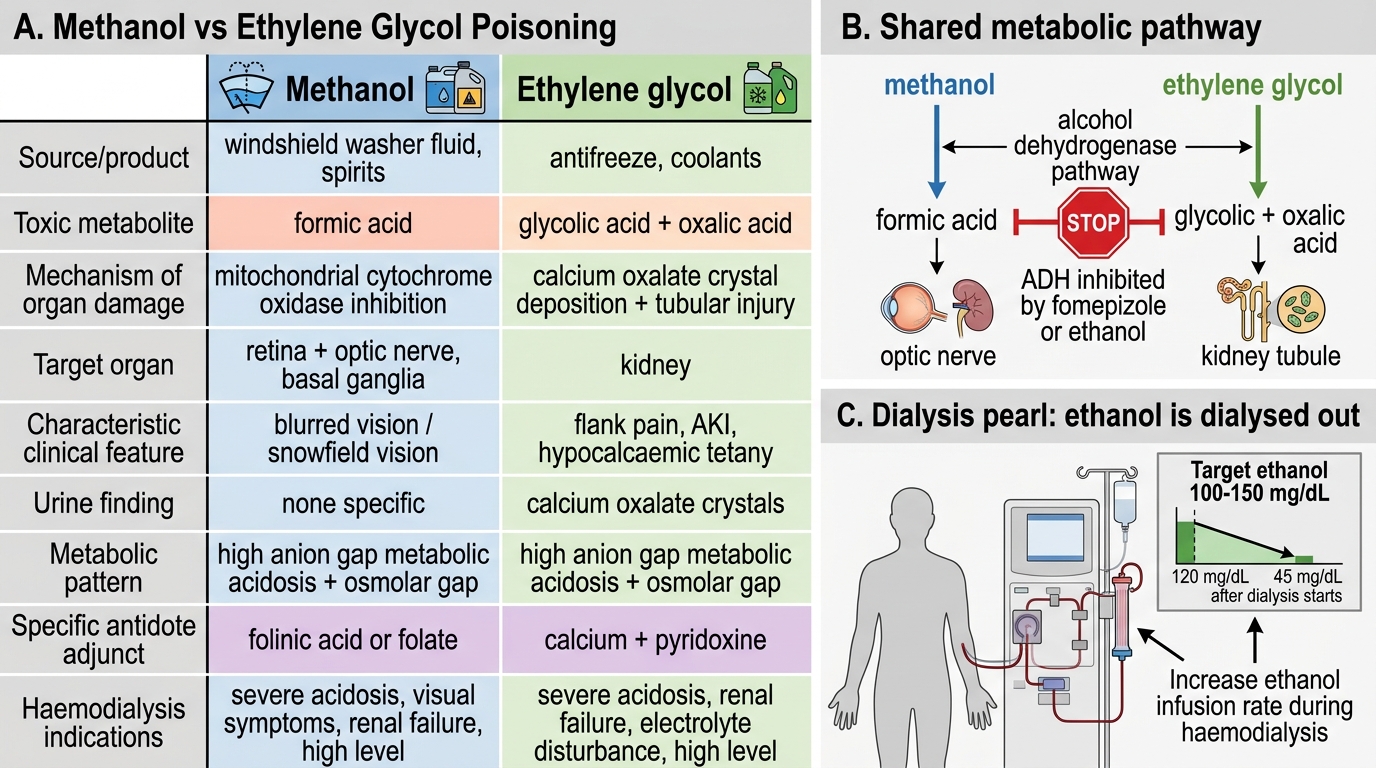
Methanol vs Ethylene Glycol Poisoning
SELF-CHECK
During haemodialysis for methanol poisoning, the patient has been receiving an IV ethanol infusion to maintain blood ethanol at 120 mg/dL. Forty minutes after dialysis starts, his blood ethanol level falls to 45 mg/dL (below the target). What is the explanation and corrective action?
A. Ethanol is removed by haemodialysis and the infusion rate must be increased during dialysis to compensate
B. The patient is metabolising ethanol faster due to ADH induction during methanol poisoning
C. Ethanol binds to the dialysis membrane and is inactivated; switch to fomepizole
D. Blood ethanol falling during dialysis is expected and no action is needed
Reveal Answer
Answer: A. Ethanol is removed by haemodialysis and the infusion rate must be increased during dialysis to compensate
Ethanol is a small, water-soluble molecule that is efficiently removed by haemodialysis — the dialysis membrane is highly permeable to ethanol. This is a critical practical point: when using ethanol as the ADH inhibitor in a patient undergoing haemodialysis, the ethanol infusion rate must be increased significantly (typically by 50-100%) during the dialysis session to compensate for dialytic removal, in order to maintain the target blood ethanol concentration of 100-150 mg/dL. This is one advantage of fomepizole over ethanol in dialysis patients — fomepizole is protein-bound and removed less efficiently by dialysis, simplifying dosing. Failure to increase ethanol during dialysis means ADH remains uninhibited during the session, allowing continued methanol metabolism to formate.
CLINICAL PEARL
The most dangerous time in methanol poisoning is the latent phase — when the patient feels well, the family thinks the danger has passed, and the emergency department staff are focused on more obviously sick patients. The elevated osmolar gap in the setting of alcohol ingestion is the single most important early clue: it confirms significant methanol or ethylene glycol in the blood, BEFORE the metabolites have accumulated. Treat based on the osmolar gap, not based on whether the patient looks sick yet. By the time vision fails or the pH falls to 7.1, the optimal treatment window has closed.
For ethanol as an antidote: the target is 100–150 mg/dL blood ethanol (moderate intoxication) — not just a few drinks or trace levels. Monitor blood glucose every 2–4 hours in all patients receiving ethanol antidote, and in children especially, because ethanol inhibits gluconeogenesis.