Page 1 of 17
IM23.1-3 | Calcium and Parathyroid Disorders — SDL Guide
Learning Objectives
- Enumerate the causes of hypercalcaemia and distinguish PTH-mediated from non-PTH-mediated mechanisms
- Describe the aetiology, clinical manifestations, diagnosis, and management of primary hyperparathyroidism
- Outline a stepwise approach to the acute and chronic management of hypercalcaemia
INSTRUCTIONS
Calcium is the most abundant mineral in the body and participates in nearly every physiological process — from nerve conduction to cardiac contraction to bone mineralisation. Disorders of calcium homeostasis therefore produce strikingly diverse and often non-specific symptoms that span multiple organ systems. This module uses the IM-foundation arc to build from normal physiology to the mechanisms of disordered calcium balance, and then applies that understanding directly to the clinical problems of hypercalcaemia and hyperparathyroidism.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 403 — Hypercalcaemia and Hyperparathyroidism (textbook)
- API Textbook of Medicine, 10th ed. — Calcium and Parathyroid Disorders (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 20 — Calcium Metabolism (textbook)
- Fourth International Workshop on Asymptomatic Primary Hyperparathyroidism Guidelines, J Clin Endocrinol Metab 2014 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old woman is referred to you after a routine biochemistry panel showed a serum calcium of 2.98 mmol/L (11.9 mg/dL). She reports vague fatigue, constipation for several months, and says she has been 'foggy in the head'. Her family doctor thought she was simply anxious and prescribed antidepressants three months ago. Now a second calcium measurement confirms the elevation. Intact PTH comes back at 92 pg/mL — elevated. Phosphate is low. Ultrasound of the neck reveals a 12 mm hypoechoic nodule posterior to the lower right thyroid lobe. The diagnosis is almost certain. Now consider a contrasting scenario: a 62-year-old man with known squamous cell carcinoma of the lung presents with nausea, confusion, and polyuria. His calcium is 3.30 mmol/L (13.2 mg/dL). PTH is undetectable at <5 pg/mL. This is not hyperparathyroidism — this is humoral hypercalcaemia of malignancy driven by PTH-related protein. Both men are hypercalcaemic, but the mechanism, implications, and urgency of treatment are entirely different. Learning to separate PTH-mediated from non-PTH-mediated hypercalcaemia is the central skill of this module.
WHY THIS MATTERS
Hypercalcaemia is encountered across virtually every medical subspecialty. It is the most common metabolic complication of malignancy, affecting up to 30% of cancer patients at some point in their illness. It is also the presenting finding in the majority of primary hyperparathyroidism cases, a condition whose incidence has risen dramatically since routine biochemistry panels became standard — the disease now presents most often asymptomatically rather than with the classic 'bones, stones, groans, and psychic moans' of textbook tradition. For NMC competencies IM23.1 through IM23.3, you are expected to work at the KH (Knowledge and Understanding applied to clinical scenarios) level — meaning you must not only classify hypercalcaemia but also interpret PTH and phosphate results, identify primary hyperparathyroidism from a case vignette, and select appropriate management for both acute severe hypercalcaemia and the chronic ambulatory form.
RECALL
Before proceeding, activate your knowledge of calcium physiology from your pre-clinical years. The body contains approximately 1000 g of calcium, of which 99% is in bone as hydroxyapatite. The remaining 1% is in extracellular fluid and cells, but this tiny fraction governs cellular excitability. Serum calcium is maintained within a narrow range of 2.1–2.6 mmol/L (8.5–10.5 mg/dL) by three hormones acting on three organs. Parathyroid hormone (PTH) is released by the four parathyroid glands in response to a fall in ionised calcium sensed by the calcium-sensing receptor (CaSR). PTH raises calcium in three ways: it increases osteoclast activity (releasing calcium from bone), increases renal tubular calcium reabsorption (while promoting phosphate excretion in the proximal tubule), and stimulates renal 1-alpha-hydroxylase to convert 25-hydroxyvitamin D to the active form 1,25-dihydroxyvitamin D (calcitriol), which in turn increases intestinal calcium absorption. Calcitonin from parafollicular C-cells of the thyroid opposes PTH by inhibiting osteoclasts, but its physiological role in adults is minor. Recall also that roughly 40% of serum calcium is protein-bound (mainly to albumin), 50% is ionised (physiologically active), and 10% is complexed to anions. When checking calcium in a hypoalbuminaemic patient, a corrected calcium must be calculated: corrected Ca = measured Ca + 0.8 × (4 − serum albumin in g/dL).
Orientation: Why Calcium Disorders Matter Clinically
Calcium homeostasis sits at the intersection of bone health, renal function, gastrointestinal physiology, neuromuscular excitability, and cardiovascular integrity. When calcium rises above the normal range, symptoms emerge from each of these systems — and the clinician who understands the physiology can predict and recognise each symptom rather than memorising a disconnected list. Conversely, hypocalcaemia (which is not the focus of this SDL but merits mention for orientation) produces the opposite pattern: increased neuromuscular excitability manifesting as tetany, paraesthesiae, Chvostek's and Trousseau's signs, and potentially fatal cardiac arrhythmias. The two poles of calcium derangement thus exemplify how a single ion, maintained in exquisite balance by a three-hormone system across bone, kidney, and gut, governs fundamental aspects of human physiology.
The clinical significance of hypercalcaemia is determined by both the absolute level and the rate of rise. Mild hypercalcaemia (serum calcium 2.6–3.0 mmol/L or 10.5–12 mg/dL) may be entirely asymptomatic and discovered incidentally on a biochemistry panel. Moderate hypercalcaemia (3.0–3.5 mmol/L or 12–14 mg/dL) typically produces constitutional symptoms. Severe hypercalcaemia (>3.5 mmol/L or >14 mg/dL) is a medical emergency associated with renal failure, cardiac arrhythmias, coma, and death if not treated promptly. The rate of rise matters: a patient whose calcium has risen gradually over months may tolerate levels that would be acutely dangerous if reached rapidly.
Primary hyperparathyroidism (PHPT) is the most common cause of asymptomatic hypercalcaemia in the outpatient setting, and malignancy is the most common cause of symptomatic hypercalcaemia in hospitalised patients. These two diagnoses account for over 90% of all hypercalcaemia encountered in clinical practice. The key discriminator — the PTH level interpreted alongside the calcium — separates them immediately and directs the subsequent workup.
Hypercalcaemia: Classification by PTH Status
Normal Calcium Homeostasis: Magnitudes and Mechanisms
The normal serum calcium range in adults is 2.1–2.6 mmol/L (8.5–10.5 mg/dL). This is maintained by a tightly regulated interplay between PTH, calcitriol, and calcitonin acting on the intestine, kidney, and bone. Understanding the quantitative relationships between these players — not just the directional arrows — is essential for interpreting clinical abnormalities.
Parathyroid hormone is an 84-amino acid peptide secreted by the chief cells of the four parathyroid glands. Its secretion is regulated by the CaSR on the cell surface: a fall in ionised calcium (below approximately 1.1 mmol/L) triggers rapid PTH release; a rise above 1.3 mmol/L suppresses it. The half-life of intact PTH is approximately 2–4 minutes. Normal serum PTH ranges from 10 to 65 pg/mL (10–65 ng/L) by most assays. PTH acts via the PTH-1 receptor on osteoblasts, renal proximal and distal tubular cells, and (indirectly, through calcitriol) intestinal cells.
The three target-organ effects of PTH are: (1) in bone, PTH stimulates osteoblasts to release RANKL, which activates osteoclasts — the net effect is calcium and phosphate mobilisation; (2) in the kidney, PTH increases distal tubular calcium reabsorption (conserving calcium) while simultaneously inhibiting proximal tubular phosphate reabsorption (causing phosphaturia and lowering serum phosphate — this inverse relationship of calcium and phosphate is a key diagnostic signal); (3) PTH activates renal 1α-hydroxylase, producing calcitriol (1,25-dihydroxyvitamin D), which increases intestinal calcium and phosphate absorption.
Calcitriol (1,25(OH)₂D₃) is synthesised from 25-hydroxyvitamin D in the kidney (proximal tubule, 1α-hydroxylation). Normal serum 25-hydroxyvitamin D (the storage form) is 50–150 nmol/L (20–60 ng/mL); frank deficiency is <30 nmol/L. Calcitriol increases intestinal calcium absorption (primarily in the duodenum and jejunum via TRPV6 channels and calbindin). In granulomatous diseases and lymphomas, macrophages express 1α-hydroxylase autonomously — this is PTH-independent calcitriol production that causes non-PTH-mediated hypercalcaemia.
Phosphate is the inverse counterpart of calcium in PTH regulation: elevated PTH → phosphaturia → low serum phosphate. In malignancy-associated hypercalcaemia from PTHrP, the same phosphaturic effect occurs (since PTHrP signals via the PTH-1 receptor). In hypercalcaemia from vitamin D toxicity or granulomas, phosphate may be normal or elevated because there is no PTH-driven phosphaturia.
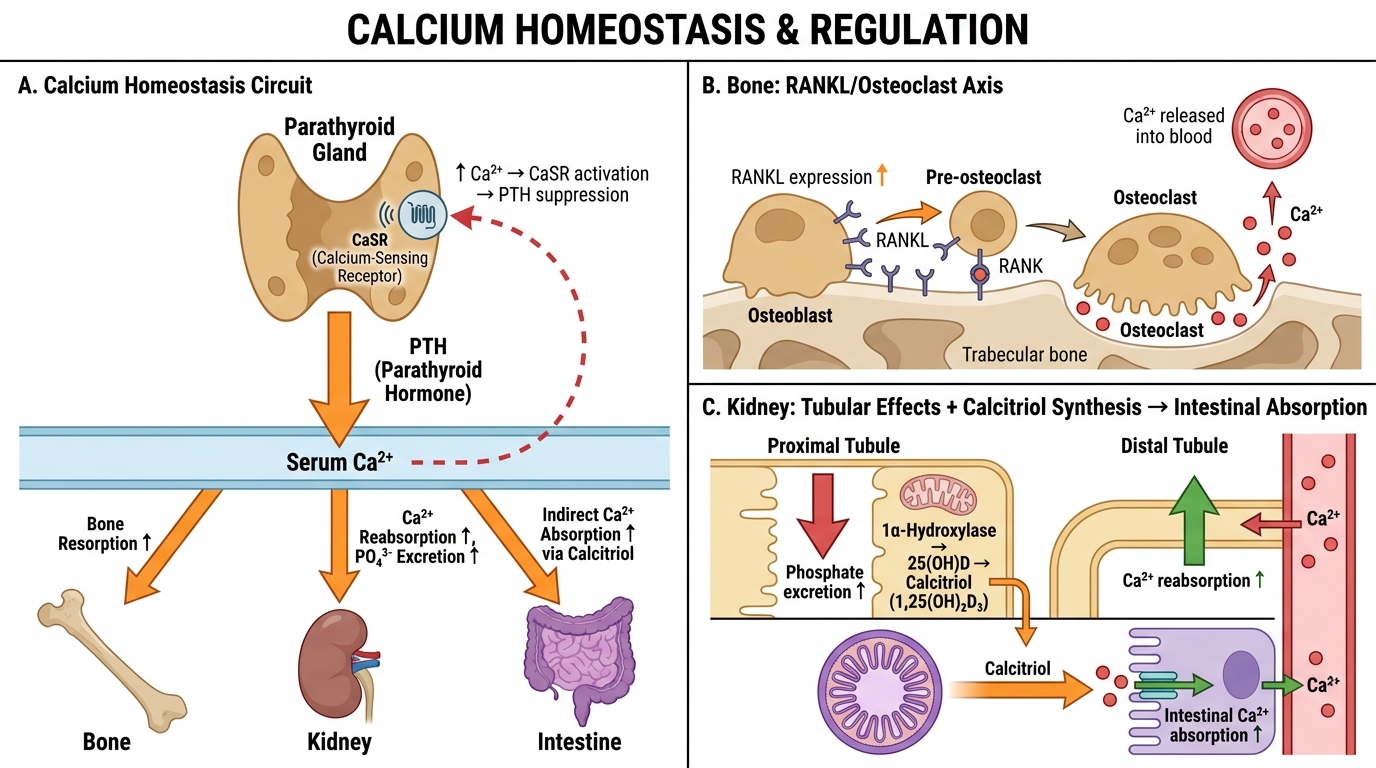
Calcium Homeostasis: PTH Synthesis, Target Organ Effects, and CaSR Feedback
Mechanisms and Causes of Hypercalcaemia: PTH vs Non-PTH Mediated
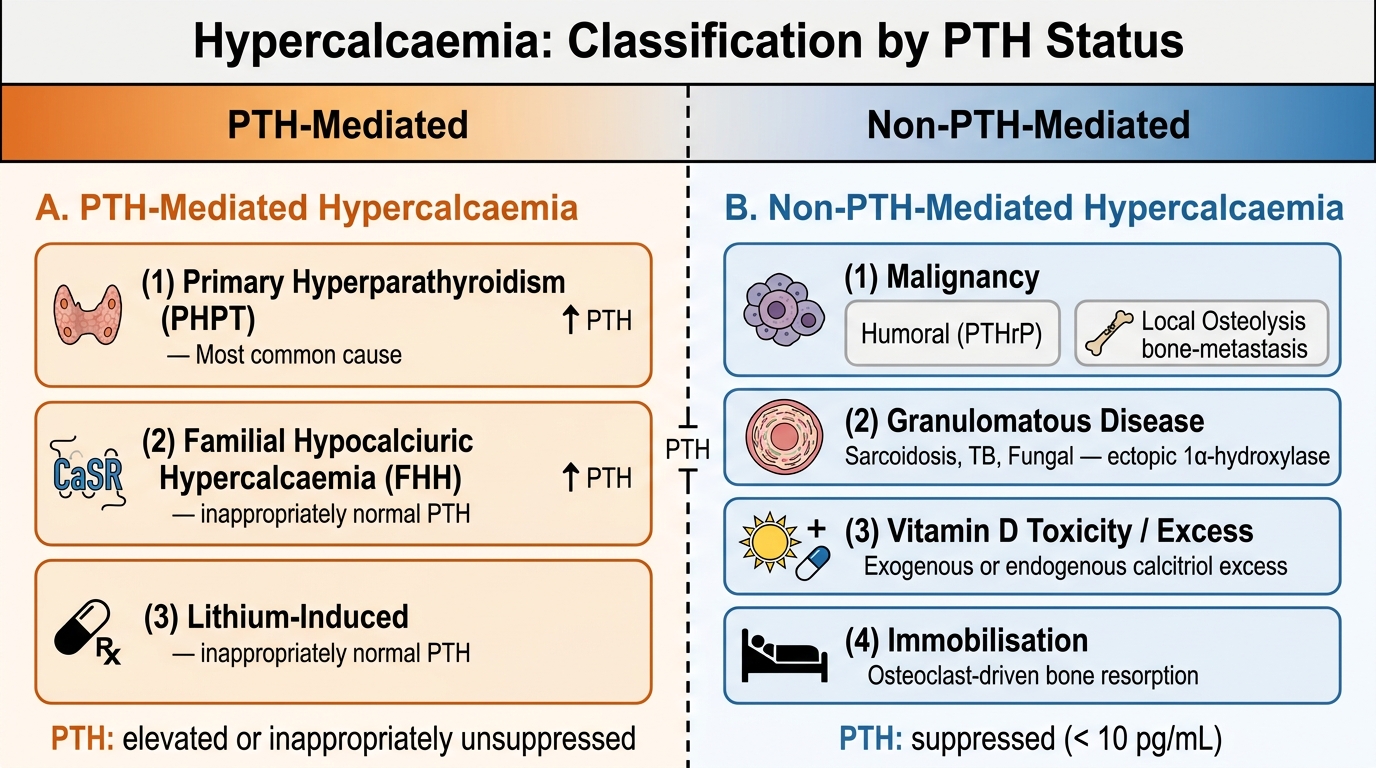
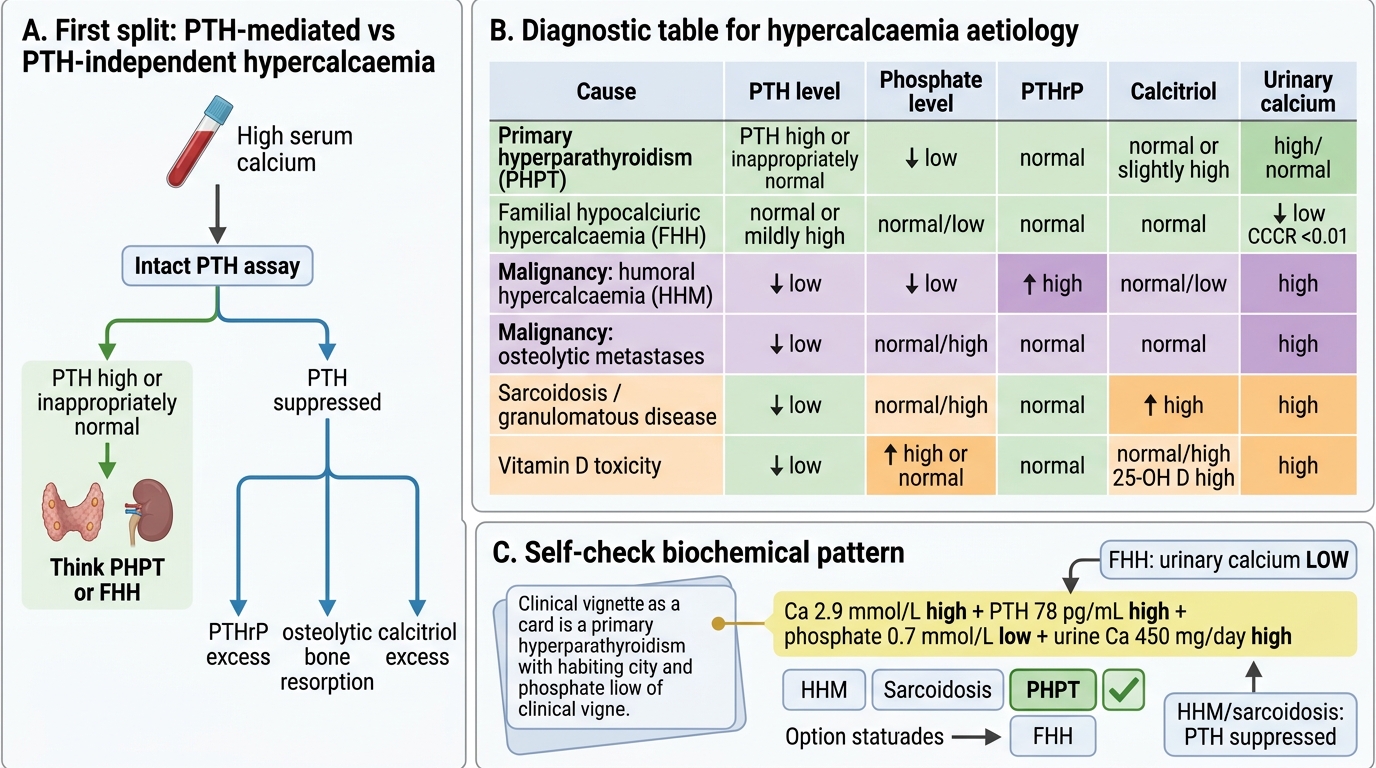
The most clinically important classification of hypercalcaemia divides causes into those where PTH is the primary driver versus those where PTH is suppressed by an independent mechanism. This distinction is made by simultaneously measuring serum calcium and intact PTH: when calcium is elevated and PTH is also elevated or even 'inappropriately normal' (i.e., not suppressed to undetectable levels), PTH is driving the hypercalcaemia. When calcium is elevated and PTH is suppressed (<20 pg/mL or undetectable), a non-PTH mechanism is responsible. Understanding the mechanism for each cause allows you to predict the full biochemical picture — not just the calcium level — and to choose targeted treatment rather than empirical calcium-lowering. Importantly, the same strategy that corrects calcium without addressing the root cause (for example, saline-only for malignancy) will lead to recurrence, whereas treating the underlying driver — whether by parathyroid surgery, chemotherapy, or glucocorticoids for granulomatous disease — produces durable improvement. The classification into PTH-mediated versus non-PTH-mediated therefore has direct therapeutic implications, not just nosological ones.
PTH-mediated hypercalcaemia arises when PTH is secreted in excess or in an unregulated fashion:
- Primary hyperparathyroidism (PHPT): the most common cause of outpatient hypercalcaemia. Occurs due to autonomous PTH secretion, most often from a single parathyroid adenoma (80–85%), less often from four-gland hyperplasia (15%), and rarely from parathyroid carcinoma (<1%). The biochemical signature is hypercalcaemia with elevated PTH, low serum phosphate (PTH-driven phosphaturia), elevated 24-hour urinary calcium (hypercalciuria), and elevated or high-normal calcitriol. Osteitis fibrosa cystica — the classic severe bone disease of untreated PHPT — is now rare because most patients are diagnosed early by routine screening.
- Familial hypocalciuric hypercalcaemia (FHH): an autosomal dominant disorder caused by a loss-of-function mutation in the CaSR gene. Because the CaSR is less sensitive to calcium, the glands behave as if calcium is always 'low' and secrete excess PTH. The critical distinguishing feature from PHPT is the low 24-hour urinary calcium (calcium-creatinine clearance ratio <0.01 in FHH vs >0.02 in PHPT). FHH is benign; parathyroidectomy is contraindicated. It must be excluded before any neck surgery for suspected PHPT.
- Lithium-induced hypercalcaemia: lithium raises the set-point of the CaSR, mimicking a mild FHH-like state. PTH is mildly elevated; the hypercalcaemia is usually mild and resolves if lithium is discontinued.
- Tertiary hyperparathyroidism: occurs after prolonged secondary hyperparathyroidism (e.g., in chronic renal failure), where one or more glands undergo autonomous adenomatous transformation and continue secreting PTH even after the original stimulus is corrected (e.g., post-renal transplantation).
Non-PTH-mediated hypercalcaemia — PTH is appropriately suppressed by the hypercalcaemia, but calcium is elevated by an independent mechanism:
- Malignancy (most common cause in hospitalised patients): three mechanisms: (1) Humoral hypercalcaemia of malignancy (HHM): PTH-related protein (PTHrP) secreted by the tumour (most often squamous cell carcinoma of lung, head/neck, oesophagus; also renal cell and breast carcinoma) binds PTH-1 receptor producing a PTH-like effect (hypercalcaemia + hypophosphataemia + elevated urinary calcium); PTH is suppressed but PTHrP is elevated. (2) Osteolytic bone metastases: direct bone destruction by metastases (breast, myeloma, lymphoma) releases calcium; PTH is suppressed, calcitriol is not elevated. (3) Calcitriol excess: lymphoma produces autonomous 1α-hydroxylase activity → elevated calcitriol.
- Granulomatous diseases: sarcoidosis, tuberculosis, histoplasmosis, berylliosis — macrophages in granulomas constitutively produce 1α-hydroxylase, generating excess calcitriol, which increases intestinal calcium absorption; PTH is suppressed; calcitriol is elevated.
- Vitamin D toxicity: exogenous overdose or excessive sun exposure in vitamin D-supplemented patients; elevated 25-hydroxyvitamin D (>500 nmol/L in overt toxicity); PTH suppressed.
- Immobilisation: in conditions with high bone turnover (Paget's, malignancy), prolonged immobilisation increases osteoclast activity and releases calcium; PTH is suppressed.
- Milk-alkali syndrome: excess calcium ingestion (antacids containing CaCO₃, often used by elderly for heartburn); PTH is suppressed; phosphate is usually elevated or normal.
- Thyrotoxicosis: excess thyroid hormone increases osteoclast activity mildly; mild hypercalcaemia; PTH suppressed; TSH undetectable.
- Addison disease / adrenal insufficiency: cortisol normally inhibits intestinal calcium absorption; in deficiency, absorption increases; mild hypercalcaemia.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Diagnostic Patterns in Hypercalcaemia
SELF-CHECK
A 52-year-old woman has asymptomatic hypercalcaemia discovered on a routine panel: calcium 2.9 mmol/L (11.6 mg/dL). Intact PTH is 78 pg/mL (normal 10–65). Serum phosphate is 0.7 mmol/L (normal 0.85–1.45). 24-hour urinary calcium is elevated at 450 mg/day. Which diagnosis best explains this biochemical pattern?
A. Humoral hypercalcaemia of malignancy
B. Sarcoidosis with calcitriol excess
C. Primary hyperparathyroidism
D. Familial hypocalciuric hypercalcaemia
Reveal Answer
Answer: C. Primary hyperparathyroidism
Elevated calcium + elevated (not suppressed) PTH = PTH-mediated hypercalcaemia. Low phosphate (PTH-driven phosphaturia) + elevated urinary calcium confirms primary hyperparathyroidism (PHPT). In malignancy-HHM, PTH would be suppressed despite a PTH-like effect (because PTHrP is not detected by the intact PTH assay). Sarcoidosis has suppressed PTH with elevated calcitriol. FHH also has elevated PTH but critically has LOW 24-hour urinary calcium (calcium-creatinine clearance ratio <0.01), which distinguishes it from PHPT.