Page 8 of 17
IM24.1-5 | Nutrition Assessment and Support — SDL Guide (Part 2)
Refeeding Syndrome: The Critical Nutritional Emergency
Refeeding syndrome is the metabolic derangement that occurs when nutrition is reintroduced after a period of prolonged starvation or severe malnutrition. It is one of the most important — and most underappreciated — complications in nutritional medicine, because it is preventable, can be fatal, and occurs specifically when treatment is initiated. The mechanism turns on phosphate.
During starvation, cells rely on fat and protein catabolism for energy. Intracellular stores of phosphate, potassium, and magnesium are depleted by the catabolic process and excreted in urine, but serum levels may remain normal (because the cells are not actively importing these anions). When carbohydrate is reintroduced, insulin secretion surges. Insulin drives glucose, phosphate, potassium, and magnesium into cells via the Na⁺/K⁺-ATPase and related transporters. Serum levels of all three crash simultaneously, but the hallmark and most dangerous drop is in phosphate — causing hypophosphataemia, which is the biochemical signature of refeeding syndrome.
Hypophosphataemia impairs ATP synthesis (phosphate is the substrate for ATP via oxidative phosphorylation) and reduces red cell 2,3-diphosphoglycerate (2,3-DPG), causing tissue hypoxia despite normal haemoglobin. The clinical consequences are: respiratory failure (diaphragmatic and respiratory muscle weakness — the most acutely dangerous), cardiac failure and arrhythmias (myocardial dysfunction), neuromuscular weakness (proximal myopathy, paraesthesiae, seizures in severe cases), haemolytic anaemia (membrane fragility), and generalised encephalopathy. Concurrent hypokalaemia and hypomagnesaemia amplify the cardiac arrhythmia risk.
Thiamine deficiency is often precipitated simultaneously — the reintroduction of carbohydrate rapidly depletes the already-low thiamine stores, triggering Wernicke encephalopathy in malnourished patients.
Risk factors for refeeding syndrome (NICE 2006 criteria): one or more of — BMI <16, unintentional weight loss >15% in the past 3–6 months, little or no nutritional intake for >10 days, or low serum levels of potassium, phosphate, or magnesium pre-feeding; OR two or more of — BMI 16–18.5, weight loss 10–15%, little or no intake for >5 days, or history of alcohol abuse or insulin, chemotherapy, antacid, or diuretic use.
Prevention and management: identify high-risk patients before feeding begins; start nutritional support at no more than 5–10 kcal/kg/day (50% of estimated requirements), increasing slowly over 4–7 days to full requirements. Supplement phosphate (PO₄), potassium, and magnesium prophylactically and correct any deficiency before and during feeding. Give thiamine 200–300 mg oral three times daily (or IV if unable to take orally) for the first 10 days. Monitor serum electrolytes daily in the first week of refeeding. Do NOT restrict fluid unless specifically indicated.
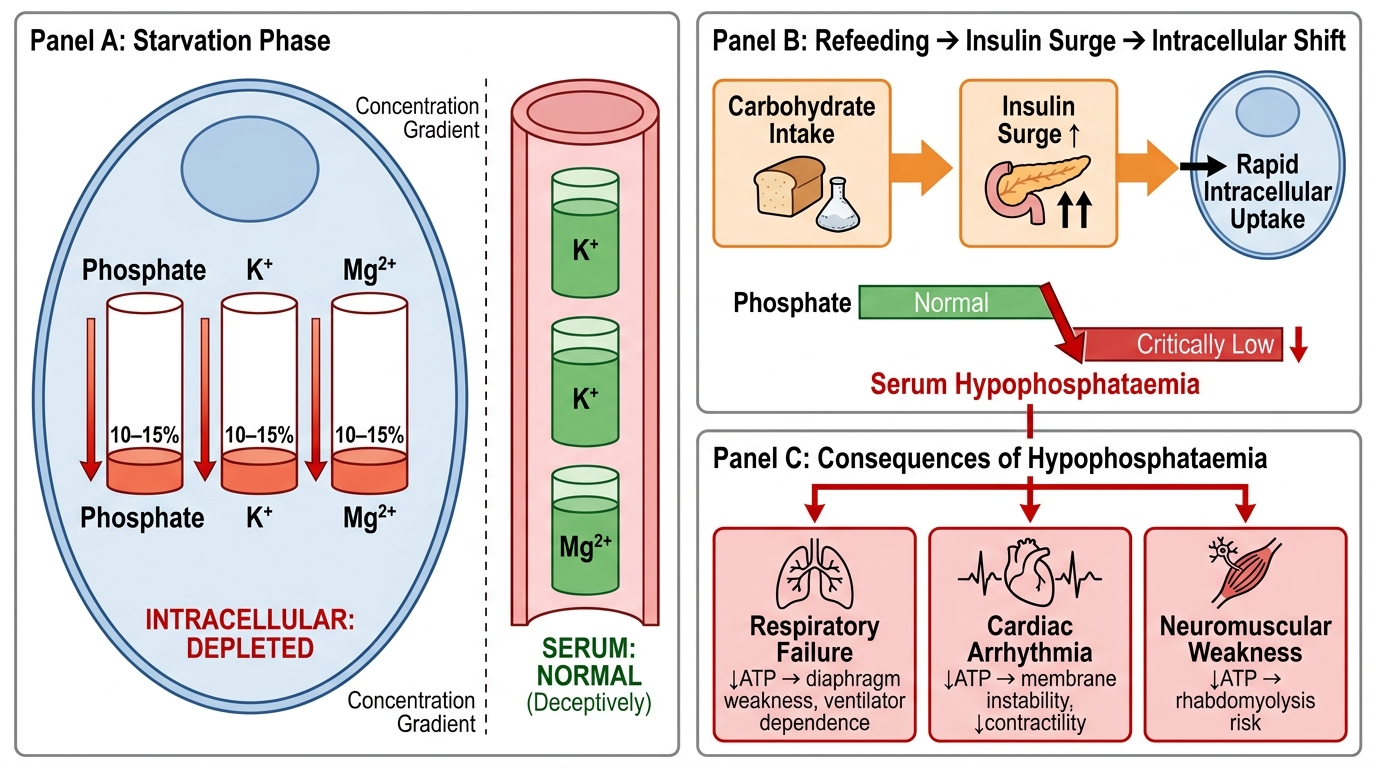
Refeeding Syndrome: Pathophysiological Mechanism and Clinical Consequences
Enteral and Parenteral Nutrition: Indications and Principles
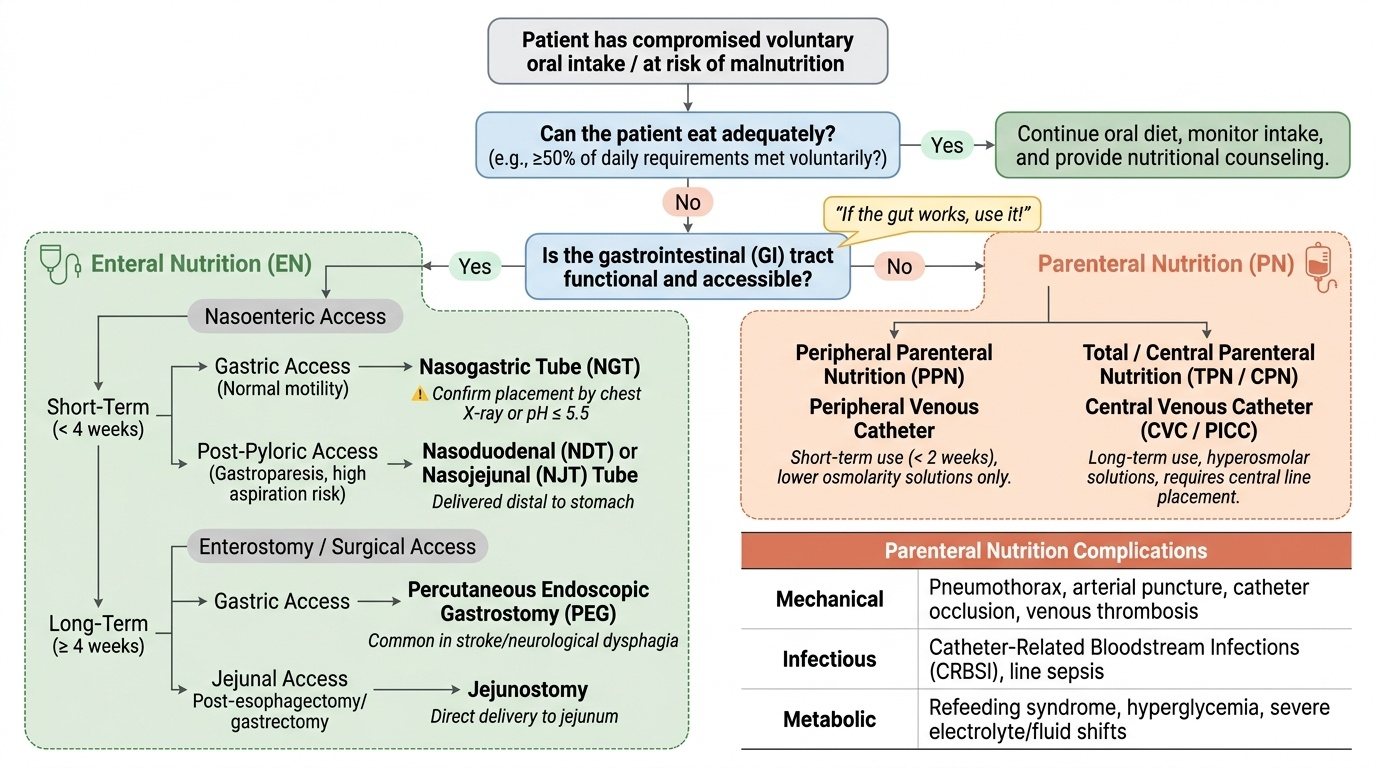
When a patient cannot meet their nutritional requirements through voluntary oral intake, artificial nutritional support is required. The two modalities are enteral nutrition (EN) — delivery of nutrients into the gastrointestinal tract via a tube — and parenteral nutrition (PN) — delivery of nutrients directly into the bloodstream via a central or peripheral venous catheter. The fundamental principle governing the choice between them is captured in the aphorism: 'If the gut works, use it.' This is not merely tradition — the evidence strongly supports enteral over parenteral nutrition in nearly every clinical setting, because enteral feeding maintains gut mucosal integrity, stimulates intestinal immune function, reduces bacterial translocation, and is associated with fewer infectious complications, lower cost, and lower mortality compared to parenteral nutrition.
Provided image
Calculating nutritional requirements: The total daily energy requirement is estimated by the Harris-Benedict equation (caloric requirement = BMR × activity factor × stress factor) or by indirect calorimetry (the gold standard). In practice, the rule of thumb for critically ill patients is 25–30 kcal/kg/day for total energy and 1.2–2.0 g/kg/day of protein. Requirements increase with fever (10% per degree Celsius above 37°C), sepsis, burns, and major surgery; they decrease in sedated, ventilated patients.
Enteral nutrition — indications and route:
EN is indicated when: (1) the patient cannot eat or is eating less than 50% of estimated requirements for more than 3 days; (2) there is anticipated prolonged impairment of oral intake (e.g., major head and neck surgery, oesophageal cancer, coma, severe stroke); (3) the gut is functional and accessible. Routes: nasogastric tube (NGT) — first line; confirm placement radiologically before use (chest X-ray or pH ≤5.5 on aspirate). Nasoduodenal or nasojejunal tube — for patients with gastroparesis, high aspiration risk, or pancreatitis (feeds are delivered distal to the stomach). Percutaneous endoscopic gastrostomy (PEG) — for long-term (>4 weeks) EN; most commonly used in dysphagia from stroke or neurological disease. Jejunostomy — used after oesophagectomy or gastrectomy; delivers feeds directly to the jejunum.
Contraindications to EN: complete mechanical small bowel obstruction, ischaemic bowel, high-output proximal small bowel fistula (>500 mL/day), severe haemodynamic instability where gut perfusion is compromised. Short-term ileus after surgery is NOT a contraindication — early post-operative EN (within 24–48 hours) is now standard of care in most surgical specialties.
Parenteral nutrition — indications and route:
PN is reserved for situations where the gut cannot be used or where EN alone is insufficient. Key indications: short bowel syndrome (less than 60–100 cm of functional small bowel remaining after resection), severe acute pancreatitis where enteral access beyond the ligament of Treitz is not possible, high-output enterocutaneous fistula (>500 mL/day) where enteral absorption is impossible, prolonged paralytic ileus, bowel obstruction not amenable to immediate surgery, severe mucositis after chemotherapy/radiotherapy preventing any enteral intake.
PN access: central venous access is standard for full PN formulations because the high osmolality damages peripheral veins (thrombophlebitis). Central venous catheters (subclavian or internal jugular — placed with Seldinger technique and confirmed by chest X-ray before use) or PICC lines (peripherally inserted central catheters — lower infection risk for long-term use). Peripheral parenteral nutrition (PPN) uses lower-osmolality formulations tolerable in peripheral veins; limited to short-term use (<2 weeks) and lower caloric density.
Complications of PN: The most important are: catheter-related bloodstream infections (CRBSI — Staphylococcus aureus and CoNS most common; strict aseptic technique and dedicated single-lumen access are the primary prevention strategies); hyperglycaemia (insulin resistance in critical illness + glucose in PN solutions — monitor glucose 4-hourly; target 6–10 mmol/L; use insulin infusion if above target); metabolic complications — hypophosphataemia (especially in refeeding), cholestatic liver disease (TPN-associated cholestasis from lack of gut stimulation), trace element deficiency with long-term use.
The ESPEN 2019 guidelines on ICU nutrition recommend: EN within 24–48 hours of ICU admission if haemodynamically stable; PN is added only if EN is contraindicated or if EN meets less than 60% of requirements after 3–5 days. Do NOT overfeed — excess caloric intake (especially glucose) increases CO₂ production (respiratory quotient of glucose = 1.0 vs fat = 0.7), worsens hyperglycaemia, and increases infection risk.
SELF-CHECK
A 35-year-old woman with Crohn's disease involving the terminal ileum underwent a 120 cm ileal resection 2 years ago. She now has persistent diarrhoea and weight loss. Her B12 is 85 pg/mL (low). The MOST appropriate route of B12 supplementation is:
A. Oral cyanocobalamin 1000 mcg daily
B. Intramuscular hydroxocobalamin 1000 mcg every 3 months
C. Sublingual methylcobalamin 500 mcg daily
D. Increasing dietary red meat and dairy intake alone
Reveal Answer
Answer: B. Intramuscular hydroxocobalamin 1000 mcg every 3 months
B12 absorption in the terminal ileum requires binding to intrinsic factor (IF) secreted by gastric parietal cells. After terminal ileal resection, this absorption pathway is absent — oral B12 (even at high doses) relies on the terminal ileum for IF-mediated absorption. While massive pharmacological doses of oral B12 (>1000 mcg/day) can achieve some passive absorption (approximately 1% of dose) in the proximal small bowel without IF, this is unreliable after extensive ileal resection with ongoing malabsorption. Intramuscular hydroxocobalamin bypasses the gut entirely and is the definitive route. Monthly or every-3-month IM injections maintain B12 stores reliably. Dietary modification alone is insufficient given the absent absorption pathway.
SELF-CHECK
A 62-year-old woman has been on total parenteral nutrition for 10 days after an ileostomy for bowel obstruction. She is now ready to start enteral feeds. Serum phosphate is 0.45 mmol/L (normal 0.85–1.45). She develops respiratory distress requiring non-invasive ventilation on day 2 of enteral re-feeding. What syndrome best explains the acute respiratory decompensation?
A. Aspiration pneumonia from nasogastric tube misplacement
B. Refeeding syndrome with hypophosphataemia causing respiratory muscle failure
C. Catheter-related bloodstream infection from the central venous catheter
D. Volume overload from the high-osmolality enteral feed solution
Reveal Answer
Answer: B. Refeeding syndrome with hypophosphataemia causing respiratory muscle failure
This is a classic refeeding syndrome presentation. The patient is high-risk: prolonged (10-day) TPN with minimal oral intake, pre-existing low phosphate before re-feeding. When enteral carbohydrate was introduced, insulin surged, driving phosphate into cells and causing a further fall in serum phosphate. Hypophosphataemia depletes ATP (phosphate is the substrate for oxidative phosphorylation) and impairs diaphragm and respiratory muscle function, causing acute respiratory failure. The serum phosphate of 0.45 mmol/L before feeds began was already below normal — this patient should have had prophylactic phosphate supplementation and feeds started at 5–10 kcal/kg/day only. Thiamine should also have been given before re-feeding.
CLINICAL PEARL
Two nutritional pearls that directly prevent harm:
First: in any malnourished or alcoholic patient with an altered level of consciousness, thiamine MUST be given before glucose. Administering glucose to a thiamine-depleted patient precipitates Wernicke encephalopathy by consuming the last of the available thiamine reserves. In an emergency, if you are unsure whether glucose or thiamine is needed first, give thiamine immediately before the dextrose bolus — you cannot cause harm with thiamine, but you can precipitate irreversible Korsakoff psychosis with dextrose alone.
Second: the 'if the gut works, use it' principle has a practical corollary: post-operative ileus is NOT a contraindication to early enteral feeding. The small bowel recovers peristaltic function within hours of abdominal surgery (well before the large bowel). Feeding through a nasojejunal tube or jejunostomy within 24–48 hours of major upper GI surgery is standard practice and reduces infectious complications compared to waiting for return of bowel sounds.
Self-Assessment: Nutritional Medicine in Clinical Context
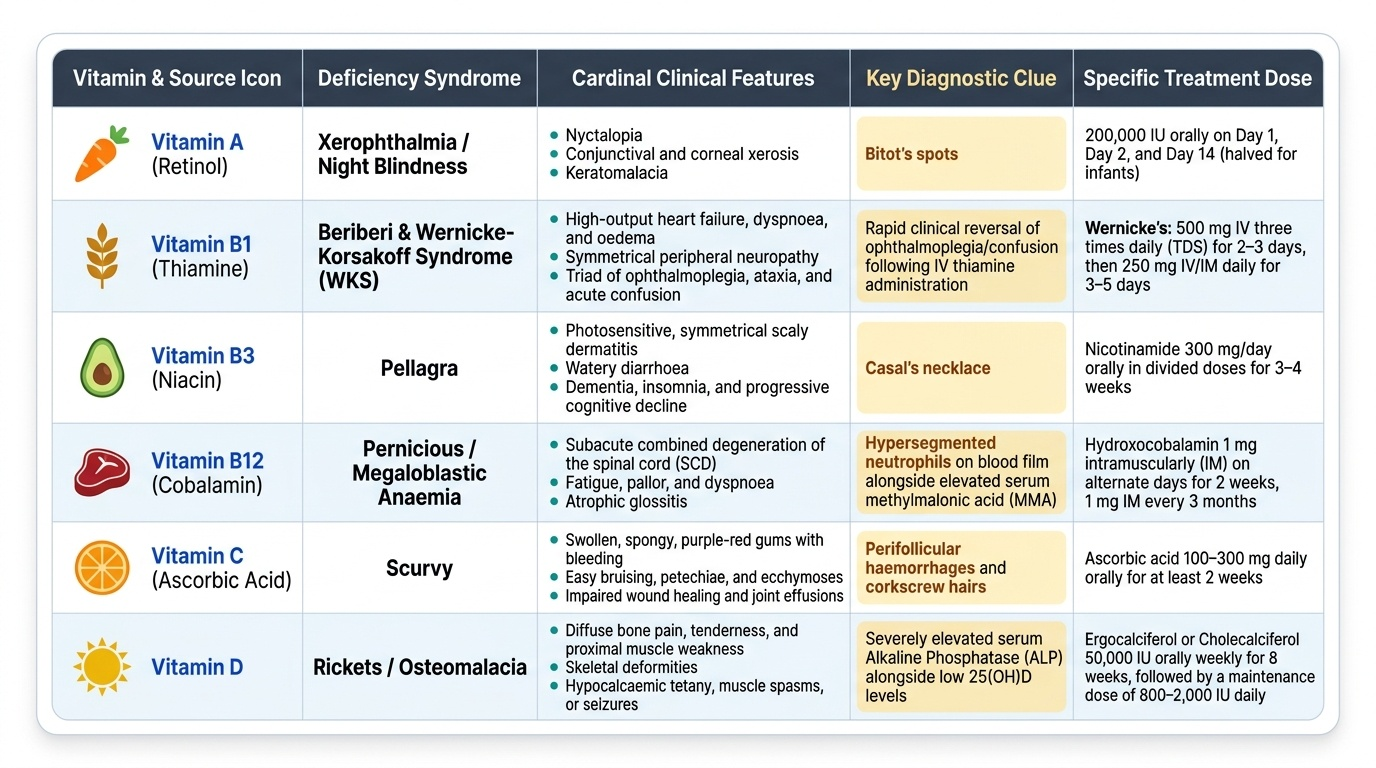
The following scenarios consolidate nutritional assessment, specific deficiency recognition, and artificial nutrition decision-making. Work through each case before reading the analysis — the objective is to integrate the ABCD assessment framework, recognise the classic deficiency syndromes from their clinical clues, and apply the EN-versus-PN decision algorithm correctly. Nutritional medicine requires pattern recognition at two levels: identifying a specific deficiency syndrome from its clinical hallmarks (Casal necklace = pellagra; Bitot spots = vitamin A; gum bleeding + perifollicular haemorrhage = scurvy) and making systematic decisions about support modality based on gut function, duration, and risk. These are the skills tested in the IM24.1–24.5 competencies at the KH and SH level — including the ability to counsel a patient, which requires translating the principles of a balanced diet into practical, culturally appropriate language.
Provided image
Scenario A: A 55-year-old woman with dysphagia from oesophageal cancer is to begin chemotherapy. She is currently unable to swallow solids and has lost 8 kg (12% of body weight) in 3 months. BMI is 17.8. She is clinically euvolaemic and haemodynamically stable. What is the appropriate nutritional support strategy?
Analysis: NRS-2002 score is high (weight loss >10% + BMI <18.5 + serious disease = ≥3 → nutritional risk confirmed). The gut is functional (dysphagia is oesophageal, small bowel is intact). Indication: enteral nutrition. Route: nasojejunal tube or PEG-J (PEG with jejunal extension), placed before chemotherapy starts to ensure access for the duration of treatment. PN is not indicated — the gut works. Nutritional targets: 25–30 kcal/kg/day, 1.5 g/kg/day protein. Monitor for refeeding syndrome (13% weight loss in 3 months + low BMI = risk).
Scenario B: A 22-year-old student living in a hostel presents with fatigue, sore tongue, and tingling in both hands and feet for 3 months. He is a strict vegetarian who avoids all dairy products. Haemoglobin 8.2 g/dL; MCV 112 fL; peripheral smear shows macrocytosis and hypersegmented neutrophils. Neurological exam: absent ankle jerks bilaterally, impaired vibration sense in both feet. Serum B12: 92 pg/mL (normal 200–900). Folate: normal. What is the diagnosis and treatment?
Analysis: Megaloblastic anaemia (macrocytosis + hypersegmented neutrophils) from B12 deficiency (dietary — strict vegan, no B12 source). The neurological features (absent ankle jerks + reduced vibration = posterior column) confirm subacute combined degeneration of the cord (SACD) — this occurs in B12 deficiency, NOT in folate deficiency. This is the distinguishing diagnostic point. Treatment: IM hydroxocobalamin 1000 mcg daily for 5 days, then weekly for 4 weeks, then monthly for life (or oral high-dose B12 1000 mcg/day if no malabsorption — dietary deficiency without absorption impairment can be treated orally in reliable patients). Neurological recovery is variable but best with early treatment; haematological recovery precedes neurological improvement.
Scenario C: You are seeing a 70-year-old man in outpatient clinic for his annual review. He is diabetic, has moderate CKD (eGFR 38), and is a pure vegetarian. He mentions fatigue and occasional muscle cramps. Investigations: serum 25-OH vitamin D = 18 nmol/L (deficient), serum B12 = 185 pg/mL (borderline low), HbA1c 7.8%. He wants advice on diet. How do you counsel him?
Analysis: Competency IM24.5 — counselling. Key points: (1) Vitamin D — supplement cholecalciferol (D3) 1000–2000 IU/day; advise 15–20 minutes of sun exposure to arms and legs daily when possible; note that dark skin requires longer exposure; food sources limited (fatty fish, fortified foods). (2) B12 — strict vegetarian, elderly, borderline B12 → start oral cyanocobalamin 1000 mcg/day or consider IM injections if concerned about absorption; dairy products and eggs are acceptable vegetarian B12 sources if culturally acceptable. (3) CKD diet: moderate protein restriction (0.8 g/kg/day — not <0.6 in elderly to prevent sarcopenia); phosphate restriction (avoid dairy excess, processed foods); potassium caution (bananas, potatoes, tomatoes if K elevated). (4) Diabetes: low glycaemic index foods, whole grains over refined; distribute carbohydrate throughout the day; avoid sugary beverages. (5) Calcium: vegetarian sources — sesame seeds, ragi, green leafy vegetables; supplement if dietary intake inadequate.