Page 2 of 32
IM25.{1-2,18} | Geriatric Foundations and Assessment — SDL Guide (Part 2)
Investigation Approach in the Elderly
The investigation of an elderly patient requires a framework that is both systematic and targeted, recognising that the yield and the harm of investigations are both influenced by age-related factors. Over-investigation is hazardous — the elderly are more vulnerable to contrast nephropathy, sedation for procedures, bleeding from anticoagulation needed for procedures, and the stress of transport to testing facilities. Under-investigation is equally hazardous because of atypical presentation (absent fever in pneumonia, normal WBC in serious infection, absence of classic angina in MI). The guiding principle is goal-concordant investigation — test for what you can treat, and weight the test burden against the patient's overall goals of care.
The basic geriatric investigative panel on initial assessment includes: full blood count (anaemia is common in the elderly and often multifactorial: iron deficiency, B12/folate deficiency, chronic disease, myelodysplasia); metabolic profile (renal function — note GFR not creatinine as discussed; electrolytes — hyponatraemia is the commonest electrolyte disorder in elderly, often SIADH or thiazide-related; blood glucose); liver function tests; thyroid function (hypothyroidism and hyperthyroidism are more common in elderly and both present atypically — exclude before attributing fatigue, cognitive change, or weight loss to 'ageing'); serum vitamin B12 and folate (deficiency is common and reversible cause of cognitive impairment, neuropathy, and megaloblastic anaemia); serum albumin (marker of nutritional status and inflammation; below 3.5 g/dL predicts adverse outcomes); calcium (hypercalcaemia of malignancy; hypocalcaemia from vitamin D deficiency).
Urinalysis must be interpreted cautiously: asymptomatic bacteriuria is present in 20–50% of elderly women and 5–20% of elderly men and does NOT require antibiotic treatment (treating it does not improve outcomes and promotes resistance). Treat only when there are symptoms of UTI, or before genitourinary procedures. Attributing delirium to 'UTI' in an elderly patient with a positive dipstick but no urinary symptoms is a common and potentially dangerous diagnostic error — the delirium often has another cause.
Imaging: plain chest X-ray (CXR) to detect pneumonia, cardiac size, pleural effusion, lung mass); ECG (atrial fibrillation — the most common cardiac arrhythmia in the elderly, present in 5–15% of those over 75; conduction disease; silent ischaemia); echocardiography where indicated (diastolic dysfunction, valvular disease — aortic stenosis is the most common valvular disease in the elderly). CT brain (to exclude subdural haematoma, stroke, or tumour before labelling cognitive decline as dementia). DEXA scan for bone mineral density in all patients with fragility fracture or high fracture risk.
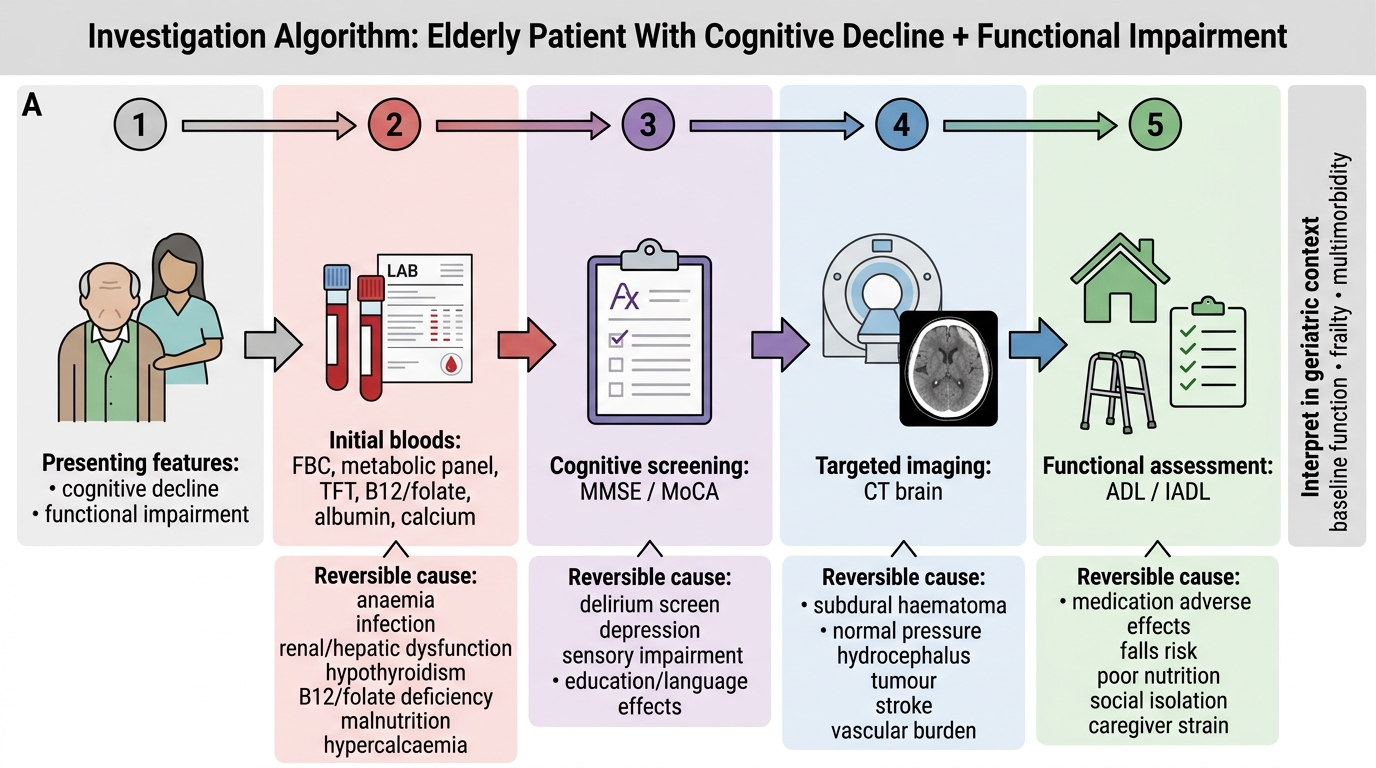
Investigation Algorithm for Cognitive Decline in Older Adults
Management Principles in Geriatric Medicine
Management of the elderly patient in internal medicine requires adapting evidence-based guidelines — most of which were derived from trials that excluded elderly patients and those with multimorbidity — to the complex reality of the frail, polymorbid older adult. Five overarching principles guide geriatric management and distinguish it from standard adult medicine.
Provided image
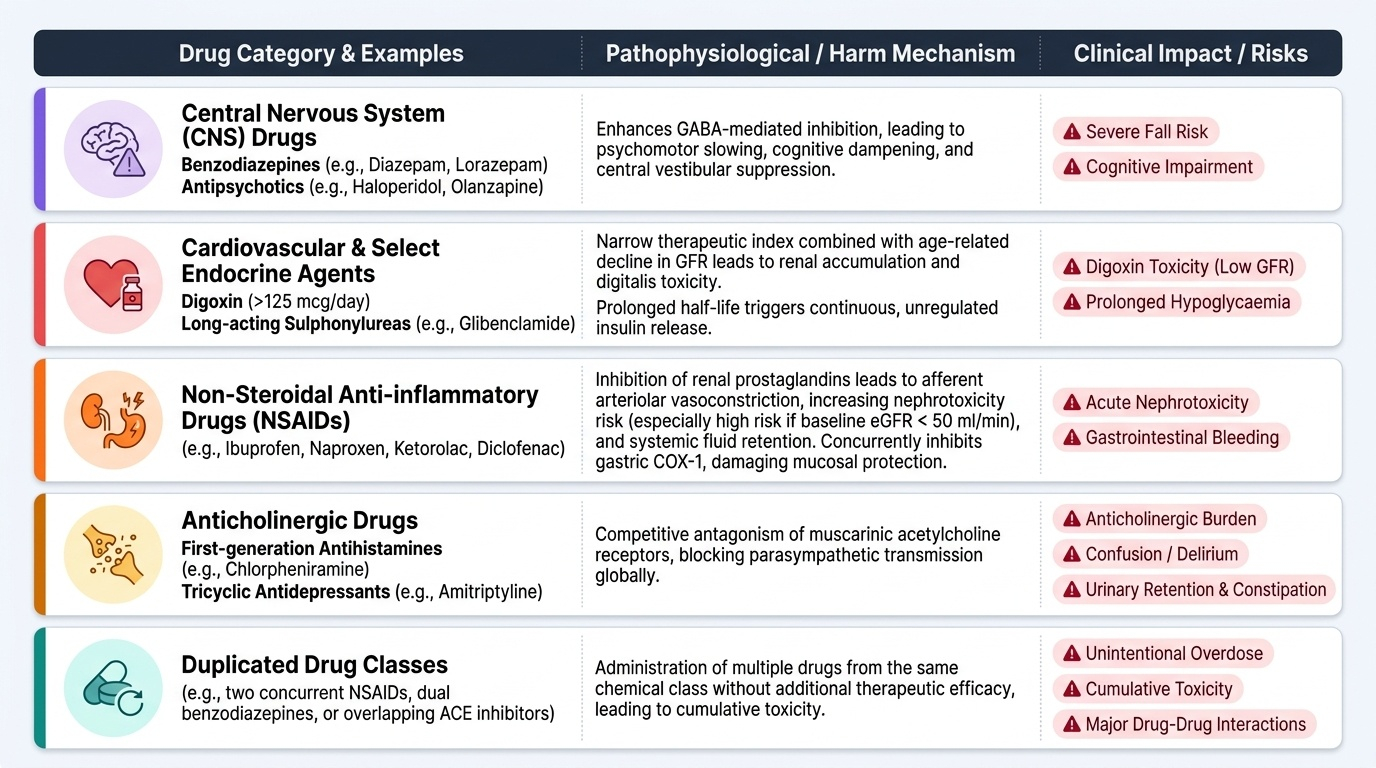
Principle 1 — Polypharmacy management and medication safety. The Beers Criteria (American Geriatrics Society, updated 2023) and the STOPP/START criteria (Screening Tool of Older People's Prescriptions / Screening Tool to Alert doctors to the Right Treatment, O'Mahony 2015, version 2) are the two principal validated tools for identifying potentially inappropriate medications (PIMs) in the elderly. The STOPP criteria list medications that are potentially inappropriate in older patients based on risk-benefit assessment (e.g., first-generation antihistamines — anticholinergic burden; long-acting sulphonylureas — prolonged hypoglycaemia risk; NSAID in eGFR <50 — nephrotoxicity and GI bleeding risk; benzodiazepines — fall and cognitive impairment risk; digoxin >125 mcg/day — toxicity risk at low GFR). The START criteria identify medications that are potentially omitted inappropriately (e.g., statins in known atherosclerotic disease, ACE inhibitors in systolic heart failure, vitamin D and calcium supplementation in osteoporosis). Medication reconciliation — compiling a complete and accurate medication list — is a patient safety imperative. The goal is to achieve the simplest effective regimen (deprescribing where benefit is marginal), not necessarily to treat every guideline target.
Principle 2 — Fall prevention. Falls are the most common and consequential geriatric syndrome, with approximately 30% of community-dwelling elderly over 65 falling at least once a year, and 10% of falls resulting in serious injury (hip fracture, head injury). The FRAT (Falls Risk Assessment Tool) and TUG test (Timed Up and Go — normal <12 seconds; >14 seconds = significant fall risk) are validated screening instruments. Fall prevention is multifactorial: review and reduce fall-risk medications (antihypertensives, sedatives, anticholinergics), physiotherapy for balance and strength (Tai Chi is evidence-based), vision correction, home hazard modification, treatment of orthostatic hypotension, and vitamin D supplementation (deficiency impairs muscle function and contributes to fall risk).
Principle 3 — Rehabilitation and functional restoration. The goal of care is not merely to treat disease but to restore or maintain function. Rehabilitation begins as soon as the patient is medically stable. Physiotherapy addresses mobility, strength, balance, and gait. Occupational therapy assesses home environment and adapts activities of daily living (assistive devices, adaptations). Early mobilisation in hospital reduces delirium, venous thromboembolism, pressure ulcer development, and pneumonia — the risks of immobility compound rapidly in the elderly. The Hospital Elder Life Program (HELP) is an evidence-based multi-component intervention reducing delirium in hospitalised elderly.
Principle 4 — Goals of care and advance care planning. For many elderly patients — particularly those with advanced dementia, severe heart failure, or terminal malignancy — the goal of care is not cure or disease modification but quality of life, comfort, and maintaining the ability to live as the patient values. Advance care planning (ACP) involves a structured conversation between the patient (with decision-making capacity) and their family and healthcare team about values, preferences, and care goals. ACP supports the completion of advance directives or living wills specifying preferences for resuscitation, artificial nutrition, and hospitalisation. In India, the Supreme Court judgment in Common Cause v. Union of India (2018) legally recognised the validity of advance directives ('living wills'), providing constitutional backing for passive euthanasia in patients with terminal illness in a permanent vegetative state.
Principle 5 — Caregiver support. The family caregiver is an essential partner in geriatric care, but caring for a frail elderly person — particularly one with dementia — creates substantial psychological, physical, and financial burden (the '36-hour day' in Alzheimer caregiving). Caregiver burnout is a recognised clinical entity and a cause of elder neglect and abuse. Geriatric management must include caregiver assessment and support: providing information about the diagnosis, prognosis, and care techniques; connecting caregivers with respite services and support groups; and screening for depression and burnout in the caregiver.
SELF-CHECK
An 83-year-old woman with type 2 diabetes (HbA1c 7.4%), hypertension, and moderate Alzheimer dementia is on glibenclamide (a long-acting sulphonylurea), amlodipine, a bedtime benzodiazepine, and a first-generation antihistamine for allergic rhinitis. Using STOPP criteria, which TWO medications are most likely to be flagged as potentially inappropriate?
A. Glibenclamide and amlodipine
B. Amlodipine and the antihistamine
C. Glibenclamide and benzodiazepine
D. Benzodiazepine and amlodipine
Reveal Answer
Answer: C. Glibenclamide and benzodiazepine
STOPP criteria flag: (1) long-acting sulphonylureas (glibenclamide, glimepiride) in elderly because of prolonged severe hypoglycaemia risk — especially dangerous in a demented patient who cannot report symptoms; shorter-acting sulphonylureas or SGLT-2 inhibitors are preferred. (2) Benzodiazepines — increase fall risk, cause cognitive impairment, worsen existing dementia, and can cause paradoxical agitation in demented patients. First-generation antihistamines are also flagged (anticholinergic burden — worsen cognition in dementia), but the question asks for the TWO most likely. Amlodipine is generally acceptable in the elderly for hypertension control and is not a primary STOPP concern.
Self-Assessment: Applying Geriatric Principles to Clinical Scenarios
You have now covered the epidemiology and demography of ageing in India, the pathophysiology of age-related change, the structure and domains of the Comprehensive Geriatric Assessment, and the five management principles that distinguish geriatric medicine. The following scenarios test your ability to integrate these into clinical reasoning at the NMC KH level. For each, identify the key geriatric principle being applied before reading the analysis.
Scenario A: A 78-year-old woman with hypertension, type 2 diabetes, and severe osteoarthritis is admitted with acute confusion and a positive urine dipstick for leucocytes and nitrites. The medical resident diagnoses 'UTI causing delirium' and prescribes ciprofloxacin. Her daughter reports the confusion began suddenly after the woman was found on the floor that morning. What is the most important diagnostic step the resident has omitted?
Analysis: The resident has committed the classic geriatric error of treating asymptomatic bacteriuria (positive dipstick without urinary symptoms) and attributing the delirium to UTI without considering other causes. The sudden onset of confusion following a fall should prompt CT brain to exclude subdural haematoma. Additionally, metabolic causes of acute confusional state (hyponatraemia, hypoglycaemia, renal failure) should be excluded. A fall + acute confusion = always image the brain. The geriatric principle: atypical presentation + geriatric giant (delirium) requires systematic exclusion of multiple causes, not pattern-matching on the first positive test.
Scenario B: Mr Raghavan, 82 years old, is seen in the geriatrics outpatient clinic. He lives alone, takes 11 medications (prescribed by cardiologist, nephrologist, endocrinologist, and GP), has fallen twice in three months, reports poor appetite and weight loss, and scores 22/30 on MMSE. His IADL score is 3/8. Which two CGA domains are most critically impaired and what is the priority intervention?
Analysis: Most critically impaired domains: (1) Functional — IADL score 3/8 (severely impaired instrumental function; cannot manage medications, finances, or transport independently; ADL assessment needed but likely partially impaired given the falls); (2) Medical — polypharmacy (11 medications, uncoordinated multi-specialist prescribing, high risk of STOPP violations and drug-drug interactions). Priority intervention: medication reconciliation and deprescribing review (using STOPP criteria) — because polypharmacy is likely the proximate cause of the falls and may be contributing to cognitive impairment (anticholinergic burden). Cognitive assessment (MMSE 22 = mild impairment) needs follow-up with MoCA and investigation for reversible causes. Social assessment for safety of living alone is urgent.
Scenario C: A 70-year-old man with COPD attends for annual review. He scores 0/5 on the Fried frailty phenotype (robust). His spirometry shows FEV1 61% predicted (GOLD Grade 2). He is moderately active, eats well, and has no functional limitations. How does his frailty status modify his COPD management?
Analysis: A robust (non-frail) 70-year-old with Grade 2 COPD should receive standard GOLD guideline-based management without the modifications required for frail patients: full-dose inhaled therapy (LABA/LAMA), pulmonary rehabilitation, and influenza/pneumococcal vaccination. Frailty would modify management by: reducing targets (avoid aggressive titration that risks hypotension or hypoglycaemia); simplifying regimens for cognitive and dexterity limitations; and prioritising function and symptom relief over spirometric targets. The absence of frailty indicates this patient can tolerate standard treatment targets and benefit from rehabilitation. Frailty assessment is not once-only — it should be repeated annually or after any acute illness.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
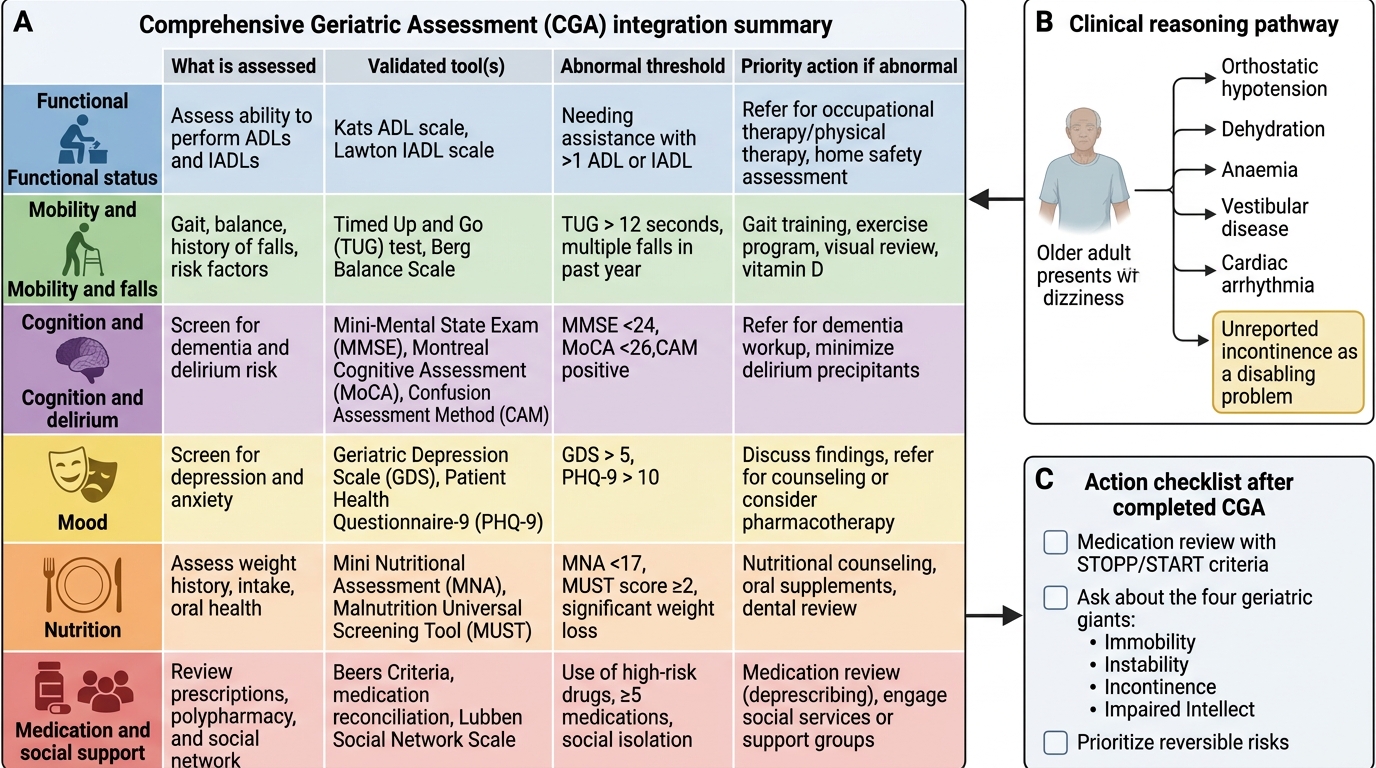
Comprehensive Geriatric Assessment Integration Summary
CLINICAL PEARL
The most important single principle in geriatric medicine is this: the presenting complaint is often not the diagnosis, and the most disabling problem is often not the chief complaint. An elderly patient who presents with 'dizziness' may have orthostatic hypotension from antihypertensives, dehydration, anaemia, vestibular disease, or cardiac arrhythmia — and their most disabling problem (which they did not mention) may be incontinence that prevents them from leaving the house. Always complete the CGA; always review the medication list with STOPP/START criteria; and always ask about the four geriatric giants (immobility, instability/falls, incontinence, intellectual impairment) regardless of the presenting complaint. A focused single-diagnosis approach is the most dangerous approach in geriatric medicine.