Page 10 of 32
IM25.{8,12-14} | Geriatric Musculoskeletal Disorders — SDL Guide
Learning Objectives
- Define osteoporosis using WHO DEXA criteria and identify the fragility fractures that constitute the clinical presentation
- Classify osteoporosis as primary or secondary and identify the most common secondary causes including glucocorticoid use
- Prescribe evidence-based pharmacological treatment for osteoporosis including bisphosphonates, denosumab, and teriparatide with correct administration instructions
- Describe the pathophysiology and clinical features of osteoarthritis and apply the ACR diagnostic criteria
- Implement a stepwise management plan for OA including non-pharmacological, pharmacological, and surgical options
- Conduct a multifactorial falls risk assessment and prescribe an evidence-based multidomain falls prevention programme
INSTRUCTIONS
This module covers the four most consequential musculoskeletal conditions in elderly medicine: osteoporosis, osteoarthritis, falls, and fragility fractures. These conditions are interconnected — osteoporosis determines fracture severity when a fall occurs, OA and muscle weakness contribute to falls risk, and falls trigger the fractures that osteoporosis makes catastrophic. Mastering the prevention and management framework for this group protects elderly patients from the most common and preventable sources of disability and death.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chs 406–408 — Osteoporosis and Bone Disorders (textbook)
- API Textbook of Medicine, 11th ed., Chapters on Osteoporosis and Degenerative Joint Disease (textbook)
- National Osteoporosis Foundation NOF 2022 Clinician's Guide to Prevention and Treatment of Osteoporosis (guideline)
- NICE Clinical Guideline: Osteoporosis — Assessing the Risk of Fragility Fracture (CG146), 2012 (updated 2017) (guideline)
- AGS/BGS 2019 Updated Clinical Practice Guidelines for Prevention of Falls in Older Persons (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Meenakshi is 78 years old when her daughter-in-law brings her to the orthopaedic emergency after she slipped on a wet bathroom floor. Plain X-ray shows a subcapital fracture of the right neck of femur. The surgeon says she needs a hemiarthroplasty, but the anaesthetist is concerned: Meenakshi has hypertension, mild chronic kidney disease (eGFR 48), and a 10-year history of 'arthritis in both knees' that is now limiting her stair-climbing. She has been taking ibuprofen for the knee pain for years. The story of this hip fracture did not begin today in the bathroom — it began decades ago, with accelerating bone loss after menopause, progressive erosion of knee cartilage, and the gradual functional decline that led her to grip the bathroom wall for support. The hip fracture is the event; osteoporosis, degenerative joint disease, and falls are the long-building process. Understanding that process — and how to interrupt it — is the subject of this module.
WHY THIS MATTERS
Musculoskeletal disease is the leading cause of disability in the elderly worldwide. Hip fracture carries a one-year mortality of 20–25% in the elderly and leaves 50% of survivors permanently disabled; it is the paradigm complication of osteoporosis and falls, and entirely preventable with appropriate screening and treatment. Degenerative joint disease (osteoarthritis) affects approximately 40–60% of elderly Indians and is the leading cause of pain and mobility impairment in this age group. NMC competencies IM25.8 (osteoporosis), IM25.12 (degenerative joint disease), IM25.13 (falls), and IM25.14 (common fractures in the elderly) cover this essential quartet — together representing the dominant source of disability, hospitalisation, and death from preventable musculoskeletal disease in the elderly.
RECALL
Activate your musculoskeletal foundations. Bone remodelling is a continuous process: osteoclasts (bone resorption) and osteoblasts (bone formation) act in coordinated remodelling units. Peak bone mass is achieved at age 25–30 years and is the most important determinant of lifetime osteoporosis risk. After 40, bone mass declines at approximately 0.5–1% per year in both sexes; in women, the accelerated phase following menopause (oestrogen withdrawal) causes a further 2–3% per year loss for 5–10 years. The RANK/RANKL/osteoprotegerin pathway: RANKL (produced by osteoblasts) binds RANK on osteoclast precursors to stimulate osteoclastogenesis; osteoprotegerin (OPG) is a decoy receptor that blocks RANKL; the ratio determines osteoclast activity. Denosumab targets RANKL. Articular cartilage consists primarily of type II collagen and aggrecan proteoglycans, maintained by chondrocytes; it has no blood supply (nutrition by diffusion from synovial fluid) and extremely limited regenerative capacity — once lost, it does not regrow. These foundations underpin the disease mechanisms in this module.
Osteoporosis: Pathophysiology, Clinical Presentation and Diagnosis
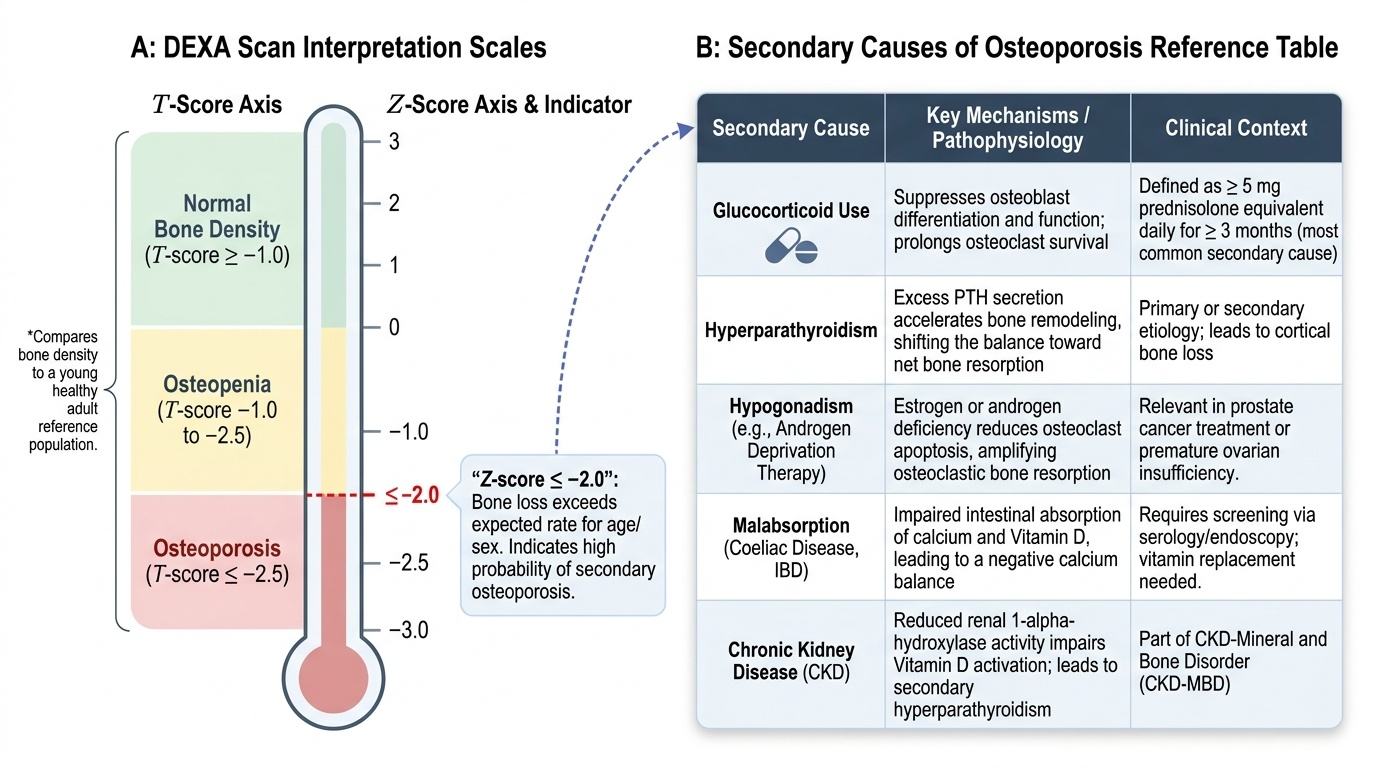
Osteoporosis is defined by the World Health Organization as a systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue, leading to bone fragility and increased susceptibility to fracture. The diagnostic threshold on dual-energy X-ray absorptiometry (DEXA) scan is a T-score ≤ −2.5 standard deviations (SD) below the mean peak bone mass of a young healthy adult reference population. Osteopenia is defined as T-score between −1.0 and −2.5. The Z-score compares bone density with an age-matched reference and is used to identify individuals whose bone loss exceeds that expected for their age and sex — a Z-score ≤ −2.0 prompts investigation for secondary causes.
Provided image
The pathophysiology of osteoporosis involves an imbalance in the remodelling cycle favouring net bone resorption. The primary aetiological distinction is: primary osteoporosis (Type I — postmenopausal, driven by oestrogen deficiency amplifying osteoclast activity and reducing osteoclast apoptosis; Type II — senile, affecting both sexes over 70 years, driven by age-related reduction in osteoblast function, calcium and vitamin D insufficiency, secondary hyperparathyroidism, and reduced physical activity) and secondary osteoporosis (caused by identifiable conditions or medications: glucocorticoid use (the most common secondary cause — suppresses osteoblast function and promotes osteoclast survival; defined as ≥5 mg prednisolone equivalent daily for ≥3 months), hyperparathyroidism, hypogonadism (including androgen deprivation therapy for prostate cancer), hyperthyroidism, malabsorption (coeliac disease, inflammatory bowel disease — calcium/vitamin D malabsorption), chronic kidney disease, multiple myeloma, and anticonvulsants (increase vitamin D metabolism).
Clinical presentation of osteoporosis is characterised by the insidious nature of bone loss — osteoporosis is clinically silent until a fracture occurs. The three characteristic osteoporotic fractures are: vertebral compression fracture (most common, often occurring without significant trauma — 'minimal trauma fracture'; presents with acute back pain or is asymptomatic and found incidentally on imaging; loss of vertebral height causing progressive kyphosis — 'dowager's hump' — and height loss); hip fracture (the most severe — high mortality and disability; typically involves the neck of femur or intertrochanteric region; falls are the precipitating event); Colles fracture (distal radius — the fall-on-outstretched-hand fracture; often the first fragility fracture and the warning sign that should prompt DEXA scanning). The fragility fracture concept: any fracture caused by a fall from standing height or less — i.e., a force that would not fracture normal bone — constitutes a fragility fracture and is diagnostic of osteoporosis until proven otherwise, even before DEXA.
DEXA scanning is the gold standard for bone mineral density (BMD) measurement. Indications: postmenopausal women with risk factors (age ≥65 without risk factors; <65 with risk factors); men ≥70 years or younger men with risk factors; any age if fragility fracture; prior to or during prolonged glucocorticoid therapy; secondary causes of bone loss. The FRAX® tool (WHO Fracture Risk Assessment Tool) estimates the 10-year probability of hip fracture and major osteoporotic fracture based on clinical risk factors (with or without BMD); it is used to guide treatment decisions — particularly in patients with osteopenia (T-score −1.0 to −2.5) where absolute fracture risk determines treatment threshold.
Falls in the Elderly: Assessment and Prevention
Falls are defined as coming to rest inadvertently on the ground or lower level, not as a result of a major intrinsic event (stroke, syncope) or overwhelming hazard. Falls are the most common and consequential geriatric syndrome: approximately 30% of community-dwelling elderly over 65 fall at least once per year, rising to 50% in those over 80. Ten percent of falls result in serious injury — hip fracture, head injury (subdural haematoma), soft tissue injury, and loss of confidence. The morbidity from falls extends beyond physical injury: fear of falling (post-fall syndrome) leads to self-imposed restriction of activity, social withdrawal, progressive deconditioning, further functional decline, and depression — creating a negative spiral.
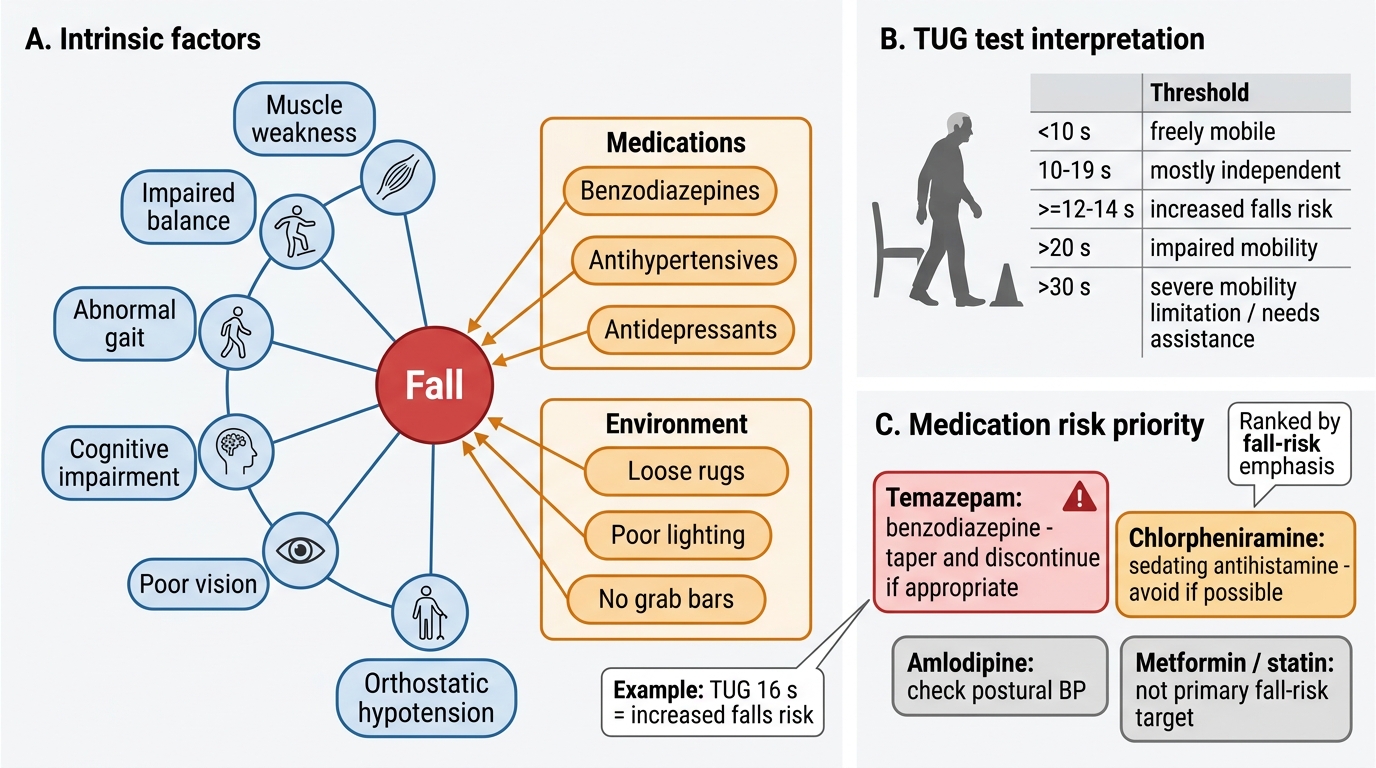
Falls in the elderly are multifactorial — the result of accumulated risk factors across multiple domains, not a single cause. The framework divides risk factors into intrinsic (patient-related) and extrinsic (environment/medication-related). Key intrinsic factors: muscle weakness (reduced quadriceps and hip extensor strength — the single most consistent predictor of falls); balance impairment (proprioceptive loss, vestibular dysfunction, cerebellar ataxia — assess with the Romberg test and tandem stance); gait abnormality (parkinsonian gait — shuffling, festinating; ataxic gait; antalgic gait from OA or foot pain; hemiparetic gait); cognitive impairment (dementia doubles falls risk — attention and executive function are needed for safe gait); visual impairment (reduced acuity, contrast sensitivity, depth perception); orthostatic hypotension (fall in systolic BP ≥20 mmHg or diastolic ≥10 mmHg within 3 minutes of standing — caused by antihypertensives, volume depletion, autonomic neuropathy, Parkinson's disease; measure lying and standing BP at every geriatric assessment). Key extrinsic/medication factors: polypharmacy (≥4 medications doubles falls risk); high-risk medications — benzodiazepines (the single highest-risk medication class for falls; odds ratio approximately 1.5–1.8), sedative-hypnotics, antidepressants (TCAs > SSRIs), antipsychotics, opioids, antiepileptics, antihypertensives (orthostatic hypotension), and diabetic medications (hypoglycaemia); environmental hazards — loose rugs, poor lighting, lack of grab bars in bathroom and toilet, slippery floors, low toilet seats, clutter.
Fall assessment tools: The Timed Up and Go (TUG) test — rise from a standard arm chair, walk 3 metres at comfortable pace, turn, walk back, sit. Normal: <12 seconds; borderline: 12–14 seconds; significant fall risk: >14 seconds. The Berg Balance Scale — 14 tasks scored 0–4 each (total 56); <45 indicates fall risk. The Physiological Profile Assessment (PPA) measures five physiological domains (vision, peripheral sensation, reaction time, quadriceps strength, balance). For routine clinical screening, the 'Get Up and Go' test (qualitative observation of rising, walking, turning) provides rapid clinical information. Standard falls history questions: How many falls in the past year? What were the circumstances? Were there any warning symptoms? Loss of consciousness? Any injury?
Falls Risk Factors and TUG Interpretation
SELF-CHECK
A 74-year-old woman has fallen twice in the past 3 months. Her TUG test time is 16 seconds. Her current medications include amlodipine 10 mg, atorvastatin 40 mg, temazepam (a benzodiazepine) 10 mg at night, metformin 500 mg twice daily, and chlorpheniramine (a first-generation antihistamine) for rhinitis. Which medication change is MOST likely to reduce her falls risk?
A. Switch atorvastatin to a lower-intensity statin to reduce myalgia risk
B. Reduce metformin dose to minimise hypoglycaemia risk
C. Taper and discontinue temazepam — benzodiazepines are the highest-risk medication class for falls in the elderly
D. Reduce amlodipine dose to minimise orthostatic hypotension
Reveal Answer
Answer: C. Taper and discontinue temazepam — benzodiazepines are the highest-risk medication class for falls in the elderly
Benzodiazepines are the single highest-risk medication class for falls in the elderly (odds ratio approximately 1.5–1.8); temazepam at night causes next-morning sedation, impairs balance, and blunts protective reflexes. Chlorpheniramine (first-generation antihistamine) also carries high falls risk (sedative and anticholinergic burden) and should also be changed to a non-sedating antihistamine. While amlodipine can cause orthostatic hypotension and should be reviewed, the primary target is the benzodiazepine. Atorvastatin and metformin are not major falls-risk medications in this context.
Degenerative Joint Disease (Osteoarthritis): Pathophysiology and Management
Osteoarthritis (OA) is the most common joint disease worldwide and the most prevalent musculoskeletal disorder in elderly Indians. It is a disease of the whole joint — not merely 'wear and tear' of cartilage — characterised by progressive loss of articular cartilage, subchondral bone remodelling (sclerosis and cyst formation), osteophyte formation, synovial inflammation, and periarticular muscle weakness. The joints most commonly affected in the elderly are: knees (most prevalent and most disabling), hips, hands (distal interphalangeal joints — Heberden's nodes; proximal interphalangeal joints — Bouchard's nodes), and lumbar/cervical spine (spondylosis). Hip and knee OA are the leading causes of pain and functional impairment requiring joint replacement surgery.
Pathophysiology: The chondrocyte (the sole resident cell of cartilage) becomes metabolically dysregulated with ageing and mechanical stress. Pro-inflammatory cytokines — particularly IL-1β and TNF-α — produced by activated chondrocytes and synoviocytes stimulate matrix metalloproteinases (collagenase, stromelysin) that degrade the cartilage extracellular matrix faster than it can be synthesised. Simultaneously, nitric oxide produced by chondrocytes inhibits proteoglycan synthesis and promotes apoptosis. The subchondral bone remodels in response to altered load distribution — sclerosis in load-bearing areas and cyst formation in areas of stress concentration. Osteophytes form at joint margins as an attempt at stabilisation. Synovial inflammation (synovitis) — driven by cartilage breakdown products released into the joint space — contributes to pain and further damage. Unlike rheumatoid arthritis, the inflammation in OA is non-specific and non-autoimmune — it is secondary to mechanical and degradation-product stimuli.
Risk factors for OA: age (the most powerful risk factor — prevalence 10% at age 60, rising to 60% by age 75); female sex (especially knee OA); obesity (the most modifiable risk factor — for every 1 kg weight loss, approximately 4 kg reduction in knee-joint reaction force with each step; obese individuals have 6-fold higher knee OA risk); prior joint injury (ACL tears, meniscal injury); occupational and recreational loading (farmers, labourers, athletes — repetitive knee bending); malalignment (varus/valgus deformity amplifies focal cartilage stress); and genetic factors (polygenically heritable — twins concordance approximately 50%).
Clinical features: OA presents with use-related joint pain (worsened by activity, relieved by rest — early disease; in late disease, rest and night pain occurs), morning stiffness <30 minutes (important distinguishing feature from rheumatoid arthritis, where morning stiffness >60 minutes), bony enlargement (osteophytes + thickened capsule), crepitus (grating sensation), and reduced range of motion. Knee OA may show varus (bow-leg) or valgus (knock-knee) deformity. Hip OA produces groin pain with loss of internal rotation. The American College of Rheumatology (ACR) clinical criteria for knee OA: age >50 + morning stiffness <30 min + crepitus + bony tenderness + bony enlargement (any 3 of 5) — in the appropriate clinical context, these criteria have 89% sensitivity and 88% specificity without requiring X-ray.
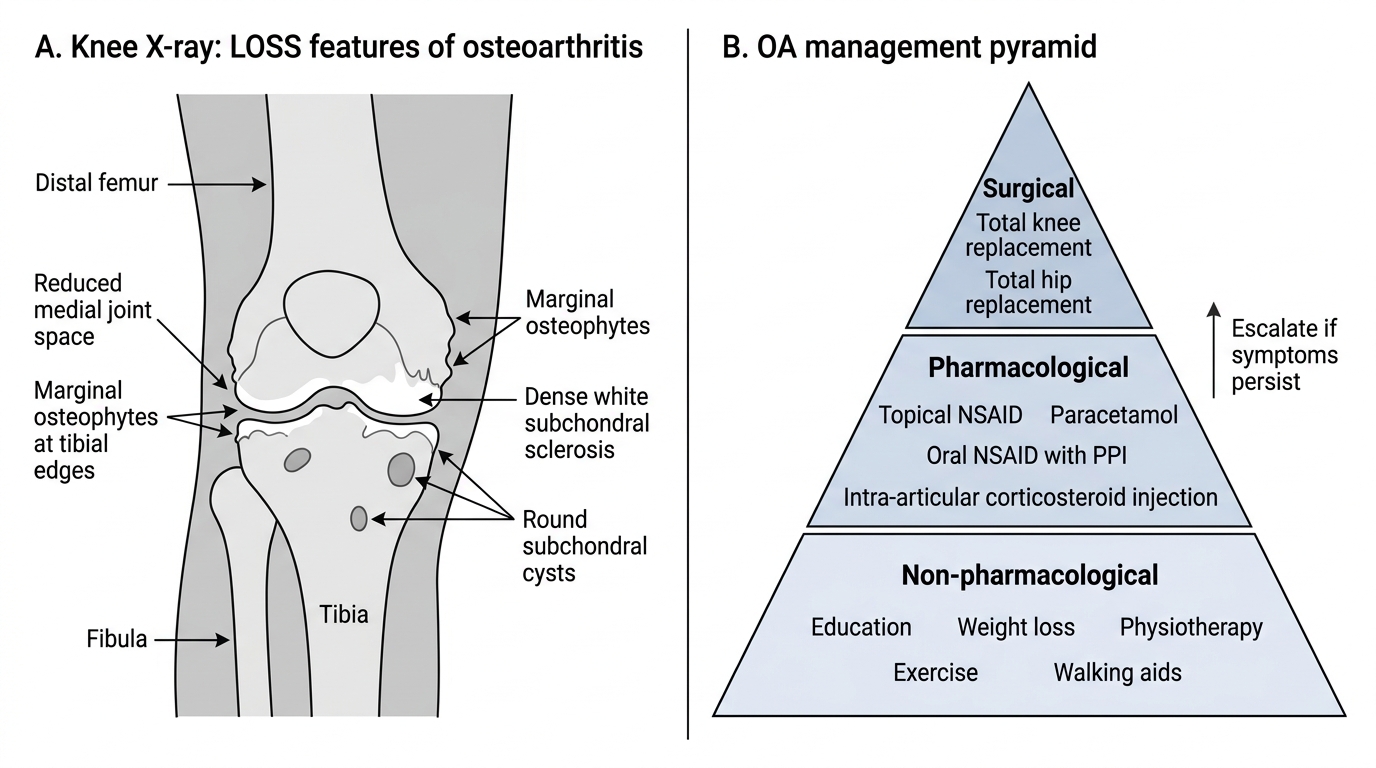
Investigation: X-ray features of OA (the 'LOSS' mnemonic): Loss of joint space (reduced cartilage); Osteophyte formation; Subchondral sclerosis (bone hardening); Subchondral cysts. MRI is more sensitive for early cartilage loss, meniscal tears, and bone marrow oedema but is not routinely needed for diagnosis. Inflammatory markers (CRP, ESR) are normal in primary OA — if elevated, consider secondary inflammatory arthritis or pseudogout (calcium pyrophosphate deposition disease, common in elderly).
Management of OA — the stepwise approach:
Non-pharmacological (always first-line): Patient education about the disease process and self-management; weight loss (the most effective intervention for knee OA — 5% body weight loss produces clinically significant pain reduction); physiotherapy — quadriceps strengthening (reduces knee load), range-of-motion exercises, gait training; occupational therapy — joint protection, assistive devices (walking aids, knee orthotics, raised toilet seats); local heat/ice for symptom relief; TENS (transcutaneous electrical nerve stimulation) for some patients.
Pharmacological: Topical NSAIDs (diclofenac gel — effective with minimal systemic absorption; first-line pharmacological choice for knee/hand OA in the elderly to avoid systemic NSAID hazards); oral paracetamol (4 g/day maximum — modest efficacy but safe in appropriate doses; avoid in liver disease); oral NSAIDs (ibuprofen, naproxen, diclofenac — reserve for short-term use only; major risks in elderly: GI ulceration and bleeding, renal impairment, fluid retention, cardiovascular risk — gastroprotection with PPI mandatory; avoid in eGFR <30, heart failure, on anticoagulants); duloxetine (SNRI — approved for chronic musculoskeletal pain including OA; useful when systemic NSAID contraindicated); intra-articular corticosteroids (methylprednisolone 40 mg or triamcinolone 40 mg — short-term significant pain relief 2–8 weeks; maximum 3–4 injections per joint per year — more frequent injections accelerate cartilage loss); intra-articular hyaluronic acid — modest and inconsistent evidence; not routinely recommended by NICE but used in some practice settings.
Surgical: Total knee replacement (TKR) and total hip replacement (THR) are highly effective for end-stage OA with severe pain and functional impairment unresponsive to conservative management. Geriatric considerations: surgery is not contraindicated by age alone; functional status and medical fitness guide decision. Post-operative rehabilitation in the elderly requires early physiotherapy, fall prevention, and anticoagulation for VTE prophylaxis.
Osteoarthritis: X-ray LOSS Features and Management Pyramid