Page 25 of 32
IM25.22 | Geriatric Nutritional Disorders — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis of nutritional disorders in the elderly including protein-energy malnutrition, sarcopaenia, vitamin deficiencies, and micronutrient deficiencies
- Recognise the clinical presentation of malnutrition, sarcopaenia, and specific micronutrient deficiencies in older adults
- Describe complications of nutritional disorders in the elderly including increased infection risk, poor wound healing, falls, and cognitive impairment
- Perform nutritional assessment of an elderly patient using validated tools including MNA, MUST, and anthropometric measures
- Outline the management of nutritional disorders in the elderly including dietary modification, oral nutritional supplements, and enteral nutrition where indicated
INSTRUCTIONS
Nutritional disorders are among the most prevalent yet underdiagnosed conditions in elderly patients. Malnutrition in a hospitalised older adult silently worsens every other disease — it delays wound healing, increases infection susceptibility, prolongs hospital stay, and accelerates functional decline. This module develops your ability to recognise, assess, and manage nutritional disorders as active medical conditions, not as incidental background findings.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 327 — Malnutrition and Nutritional Assessment (textbook)
- API Textbook of Medicine, 10th ed., Section on Geriatrics and Nutrition (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 19 — Nutritional Factors in Disease (textbook)
- ESPEN Guideline on Clinical Nutrition and Hydration in Geriatrics, 2019 (guideline)
- WHO/FAO — Vitamin and Mineral Requirements in Human Nutrition, 2nd ed., 2004 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Meenakshi, 79 years old, is admitted for an elective knee replacement. Pre-operative assessment reveals a BMI of 17.2 kg/m², mid-arm circumference at the 10th percentile for her age, and serum albumin of 2.6 g/dL. She lives alone, cooks infrequently because of arthritic hands, and reports eating 'a little rice and some dal' twice a day. She has lost 6 kg over the past year. The orthopaedic surgeon asks whether the operation should proceed. The anaesthetist notes increased anaesthetic risk. The internist is asked to review. Here is the problem: Meenakshi's knee is the stated reason for admission, but her nutritional state will determine whether the surgery succeeds or fails. Malnourished patients undergoing major surgery have three to five times the complication rate of well-nourished patients — higher infection rates, poorer wound healing, prolonged ICU stays, and increased mortality. Nutritional disorders in the elderly are not a nutritionist's problem: they are a physician's responsibility.
WHY THIS MATTERS
Malnutrition affects approximately 30–50% of hospitalised elderly patients in India, and a further 30–40% are at risk. In community-dwelling Indian elderly, studies report protein-energy malnutrition in 20–30%, with even higher rates among those aged over 80 years, those with multiple comorbidities, and those living alone or in poverty. Despite this prevalence, nutritional screening is performed in fewer than 20% of hospital admissions in most Indian institutions — meaning that the majority of malnourished elderly patients are admitted, treated, and discharged without their nutritional disorder being identified or addressed. The consequences are measurable and severe: each unit decrease in serum albumin below 3.5 g/dL is associated with a 30% increase in hospital mortality; sarcopaenia independently predicts falls, fractures, disability, and mortality. For the NMC competency IM25.22, you must be able to describe the aetiopathogenesis, clinical presentation, complications, assessment, and management of nutritional disorders in the elderly — the full KH spectrum from mechanism to management.
RECALL
Activate your prior knowledge. You have studied protein-energy malnutrition (PEM) in paediatrics — in children it produces kwashiorkor (predominantly protein deficiency: oedema, fatty liver, dermatitis, hair changes) and marasmus (predominantly energy deficiency: severe wasting, loss of subcutaneous fat). In the elderly, PEM presents differently — the dramatic paediatric phenotypes are rarely seen; instead, malnutrition manifests as gradual weight loss, muscle wasting (sarcopaenia), weakness, poor wound healing, and increased susceptibility to infection. Recall also the key micronutrients implicated in specific deficiency syndromes: vitamin C (scurvy — perifollicular haemorrhages, bleeding gums, poor wound healing), vitamin D (osteomalacia, myopathy), vitamin B12 (megaloblastic anaemia, subacute combined degeneration of the cord), thiamine/B1 (Wernicke's encephalopathy, peripheral neuropathy), folate (megaloblastic anaemia), and iron (microcytic anaemia). These syndromes occur in all ages but are disproportionately common in the elderly due to specific age-related mechanisms that this module will detail.
Clinical Presentation of Nutritional Disorders in the Elderly
The clinical presentation of nutritional disorders in elderly patients is characterised by subtlety and non-specificity — features that make recognition challenging but no less urgent. Unlike paediatric malnutrition, which often presents with dramatic syndromic features, geriatric malnutrition tends to present as a cluster of overlapping findings that each individually could be attributed to 'normal ageing' or to another comorbidity. The clinician who recognises this cluster as a nutritional syndrome and acts accordingly changes the patient's outcome; the one who attributes every finding to 'old age' misses a treatable condition.
Protein-energy malnutrition (PEM) in the elderly presents with: unintentional weight loss (a loss of >5% body weight over 6 months or >10% over 12 months is clinically significant); reduced muscle mass and strength — the clinical manifestation of sarcopaenia; generalised weakness and fatigue; impaired immunity manifesting as recurrent infections or atypical infection presentations; delayed wound healing (pressure sores that fail to granulate, surgical wounds that break down); dependent oedema from hypoalbuminaemia (serum albumin <3.5 g/dL indicates significant protein depletion); and hair and skin changes (hair thinning, dry scaly skin, nail ridging). In the hospitalised elderly, PEM compounds every concurrent illness: it extends the catabolic phase of any acute illness, impairs the anabolic phase of recovery, and increases complications across every organ system.
Sarcopaenia — the age-related progressive loss of skeletal muscle mass, strength, and physical performance — deserves specific recognition as its own clinical entity. The European Working Group on Sarcopaenia in Older People (EWGSOP2, 2019) defines probable sarcopaenia as low muscle strength (grip strength <27 kg in men, <16 kg in women, measured by handgrip dynamometry), confirmed sarcopaenia as low muscle strength plus low muscle mass (by DXA or BIA), and severe sarcopaenia as all three criteria plus low physical performance (gait speed <0.8 m/s on the 4-metre walk test, or Short Physical Performance Battery score ≤8). Clinically, sarcopaenia presents as difficulty rising from a chair without using arms, slow gait, frequent falls, and an overall appearance of wasting disproportionate to the patient's body weight. Its importance extends beyond the cosmetic — sarcopaenic patients have higher operative mortality, longer ICU stays, higher 30-day readmission rates, and are at the highest risk of the frailty cascade (acute illness → hospitalisation → immobility → further muscle loss → increased frailty).
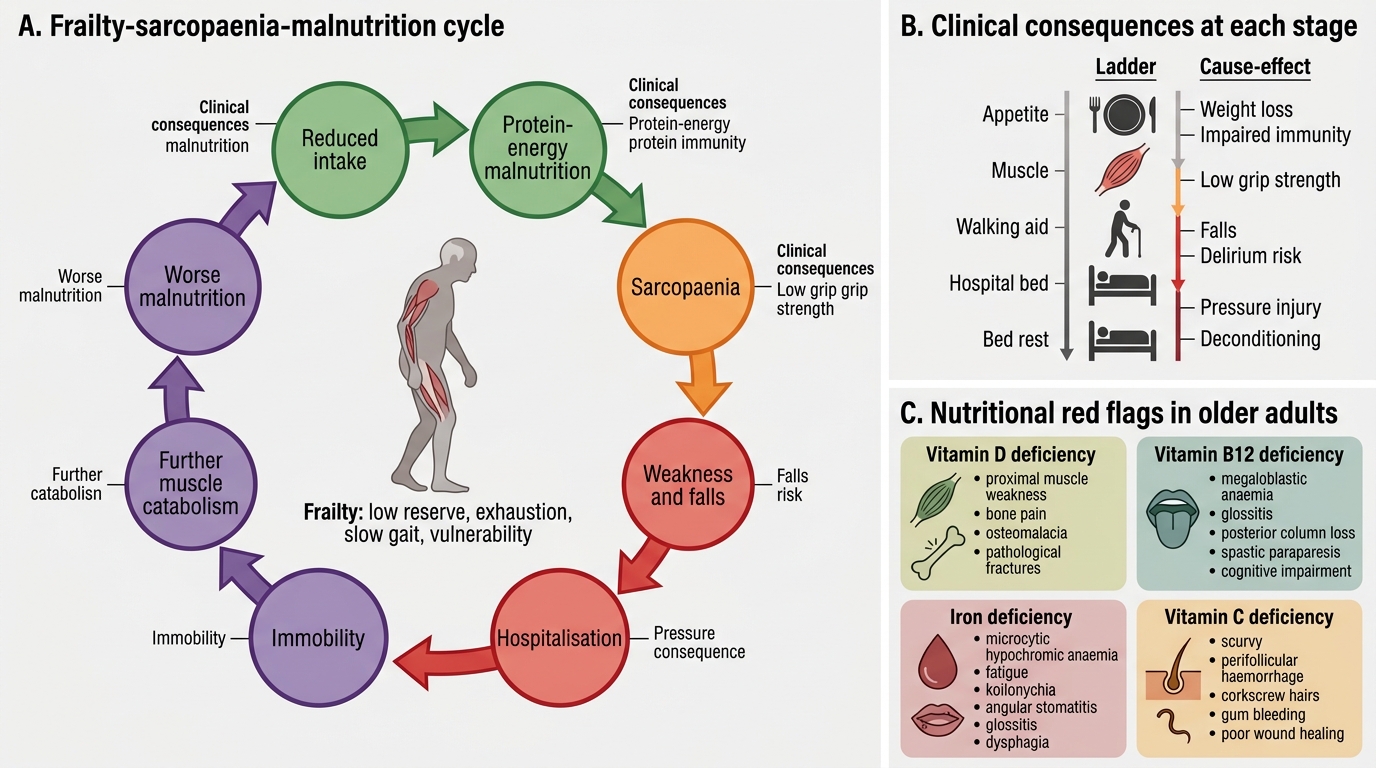
Frailty-Sarcopaenia-Malnutrition Cycle
Specific micronutrient deficiency presentations:
- Vitamin D deficiency: proximal muscle weakness (difficulty rising from chair, climbing stairs), bone pain (especially pelvis, thighs, lower back), waddling gait; in severe cases osteomalacia (diffuse bone pain, Looser zones on X-ray) and pathological fractures. Serum 25-hydroxyvitamin D <20 ng/mL = deficiency; <12 ng/mL = severe deficiency.
- Vitamin B12 deficiency: megaloblastic anaemia (pallor, fatigue, glossitis, jaundice from ineffective erythropoiesis); subacute combined degeneration (SCD) of the spinal cord — demyelination of the posterior (vibration/proprioception loss, positive Romberg) and lateral (corticospinal — spastic paraparesis, hyperreflexia) columns; peripheral neuropathy (glove-and-stocking sensory loss); and cognitive impairment (reversible dementia-like picture). Serum B12 <200 pg/mL; methylmalonic acid and homocysteine are more sensitive markers.
- Iron deficiency: microcytic hypochromic anaemia, fatigue, koilonychia (spoon nails), angular stomatitis, glossitis, dysphagia (Plummer-Vinson syndrome in severe cases).
- Vitamin C (ascorbic acid) deficiency (scurvy): perifollicular haemorrhages (corkscrew hairs with surrounding petechiae on the follicle), gingival bleeding and hypertrophy, poor wound healing, hyperkeratosis, and woody oedema of the lower limbs. Scurvy is increasingly recognised in elderly patients with restricted diets — particularly those who eat few fresh fruits and vegetables.
- Thiamine (B1) deficiency: in the elderly context most commonly presents as peripheral neuropathy (burning feet, distal sensory loss); Wernicke's encephalopathy (ophthalmoplegia, ataxia, confusion — the classic triad) can occur in severely malnourished or alcohol-dependent elderly patients.
- Zinc deficiency: poor wound healing, loss of taste and smell (ageusia/anosmia — often misattributed to ageing), recurrent infections, dermatitis.
Aetiopathogenesis: Why Are the Elderly Nutritionally Vulnerable?
Understanding why older adults are specifically vulnerable to nutritional disorders requires knowing the multiple overlapping mechanisms that act simultaneously on intake, absorption, metabolism, and requirement. These are not simply the consequences of poverty or neglect — they are structural biological and social features of ageing that operate independently of socioeconomic factors, though poverty amplifies every one of them. A framework that organises these mechanisms into four categories — reduced intake, impaired absorption, altered metabolism, and increased requirements — is the most efficient way to understand the aetiopathogenesis and to identify appropriate intervention points.
Reduced intake is driven by multiple factors unique to ageing. The anorexia of ageing is a well-characterised physiological phenomenon caused by delayed gastric emptying (prolonged satiation after meals), increased postprandial release of cholecystokinin (a satiety hormone), and altered central leptin and neuropeptide Y signalling — together these reduce hunger and increase early satiety. Superimposed on this physiological anorexia are multiple pathological contributors: dentition problems (edentulism, poorly fitting dentures) that impair chewing; xerostomia (dry mouth) from anticholinergic medications and autonomic dysfunction that makes swallowing uncomfortable; dysgeusia and anosmia (altered taste and smell) that reduce food palatability; dysphagia from stroke, Parkinson's disease, oropharyngeal muscle weakness, or oesophageal dysmotility; cognitive impairment (forgetting to eat, inability to prepare food, loss of mealtime self-care); depression (a major and frequently missed cause of poor appetite and weight loss in the elderly); polypharmacy (multiple drugs cause anorexia — digoxin, metformin, SSRIs, opioids, bisphosphonates); financial poverty; social isolation (the social facilitation of eating is lost when one eats alone); and mobility limitations that prevent shopping or cooking.
Impaired absorption is a significant contributor in elderly patients. Atrophic gastritis — affecting approximately 30% of those over 60 years — reduces gastric acid production (achlorhydria), which impairs the absorption of vitamin B12 (requires intrinsic factor from parietal cells; atrophic gastritis destroys both acid and intrinsic factor), iron (requires acidic environment for ferric-to-ferrous conversion), calcium, and zinc. Small intestinal bacterial overgrowth (SIBO), which is more common in the elderly due to reduced gastric acid and impaired motility, can cause malabsorption of fat, fat-soluble vitamins, and B12. Pancreatic exocrine insufficiency increases with age, impairing fat and fat-soluble vitamin (A, D, E, K) absorption. Drug interactions with absorption are also important: proton pump inhibitors (the most widely prescribed drug class in the elderly) further reduce gastric acid and impair B12 and iron absorption; cholestyramine impairs fat-soluble vitamin absorption; antacids impair iron absorption.
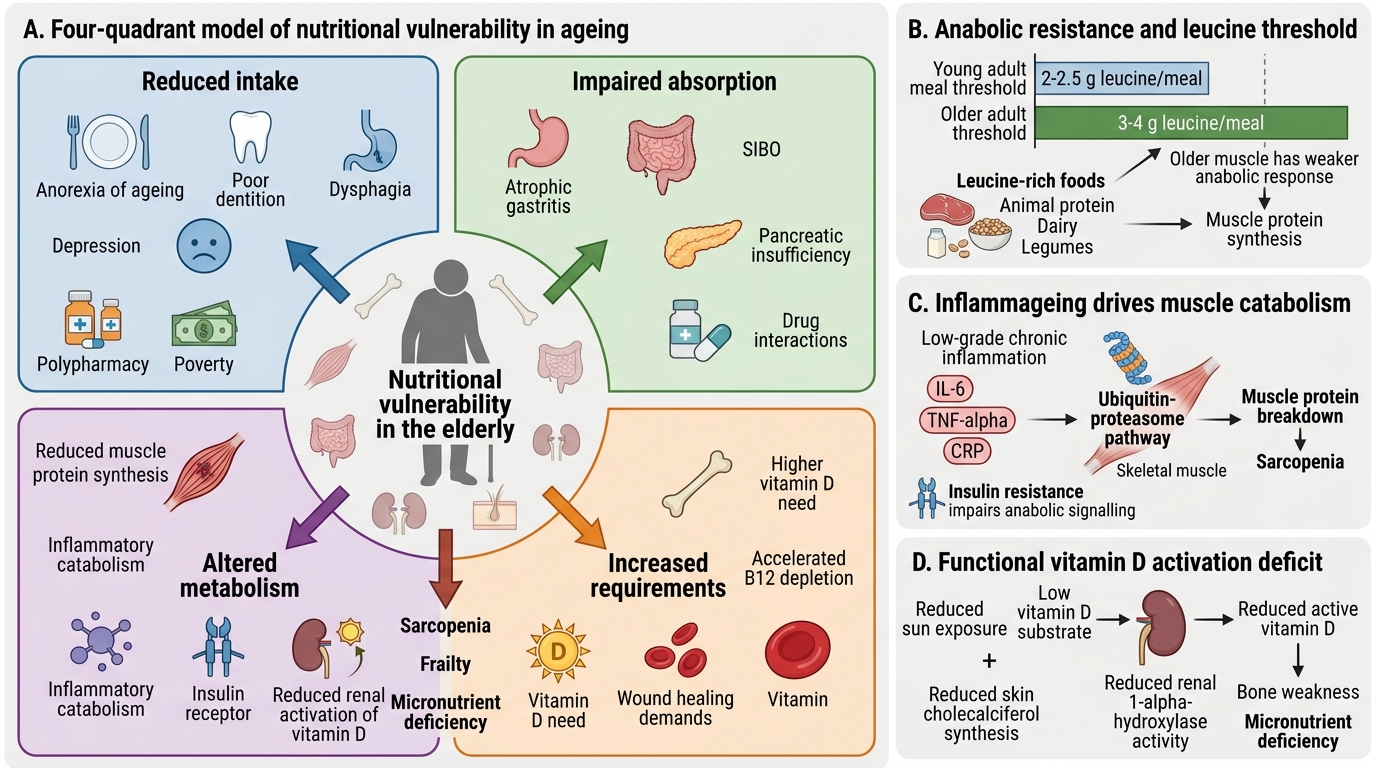
Nutritional Vulnerability in the Elderly
Altered metabolism drives sarcopaenia and micronutrient deficiencies by mechanisms intrinsic to ageing physiology. The elderly have a blunted anabolic response to protein — the leucine threshold for initiating muscle protein synthesis is higher in older adults (approximately 3–4 g per meal vs 2–2.5 g in young adults), meaning that meals need to be higher in leucine-rich proteins (animal proteins, dairy, legumes) to stimulate muscle anabolism. Low-grade chronic inflammation (inflammageing — elevated IL-6, TNF-α, CRP) drives muscle protein catabolism through the ubiquitin-proteasome pathway, contributing to sarcopaenia even when caloric intake appears adequate. Insulin resistance in elderly skeletal muscle impairs anabolic signalling. Reduced sun exposure and diminished skin synthesis of cholecalciferol, combined with reduced renal 1-alpha-hydroxylase activity, create a functional deficit in vitamin D activation even when dietary intake is nominally adequate — this is why the elderly require higher vitamin D supplementation (800–2000 IU/day) than younger adults.
Increased requirements arise from both physiological and pathological factors. Acute illness triggers a hypermetabolic catabolic state with protein requirements increasing to 1.2–1.5 g/kg/day (vs the standard recommendation of 0.8 g/kg/day). Pressure sores, surgical wounds, and chronic inflammatory conditions create localised demands for protein, vitamin C (collagen synthesis), zinc (wound healing), and iron (haemoglobin for oxygen delivery to healing tissue). Concurrent medications create micronutrient competition or depletion — metformin depletes B12 (inhibits ileal absorption), isoniazid depletes B6, furosemide increases renal losses of zinc, potassium, and magnesium.
SELF-CHECK
A 74-year-old woman on long-term metformin for type 2 diabetes presents with a 6-month history of tingling in both feet, unsteadiness on walking in the dark, and a smooth red tongue. Her haemoglobin is 9.2 g/dL with MCV 108 fL. Which nutritional deficiency BEST explains this clinical picture?
A. Iron deficiency
B. Vitamin D deficiency
C. Vitamin B12 deficiency
D. Thiamine deficiency
Reveal Answer
Answer: C. Vitamin B12 deficiency
The combination of macrocytic (high MCV) anaemia, peripheral sensory neuropathy (tingling in feet), dorsal column signs (unsteadiness in the dark = impaired proprioception — positive Romberg), and glossitis (smooth red tongue) is the classic presentation of vitamin B12 deficiency causing subacute combined degeneration of the spinal cord. Metformin inhibits ileal absorption of vitamin B12 — this is a well-documented and common cause of B12 depletion in elderly diabetic patients on long-term metformin. Iron deficiency causes microcytic anaemia (low MCV), not macrocytic. Vitamin D deficiency causes proximal muscle weakness and bone pain, not neuropathy or macrocytic anaemia. Thiamine deficiency causes a neuropathy but not macrocytic anaemia and is associated with ophthalmoplegia, not predominantly dorsal column signs.
Nutritional Assessment: Tools and Methods
Nutritional assessment of the elderly patient requires a systematic approach that combines clinical history, anthropometry, biochemical markers, and validated screening tools. No single parameter is sufficient — BMI alone is unreliable in the elderly (oedema can mask muscle wasting; loss of height with vertebral compression inflates BMI; the healthy weight range shifts upward with age), and biochemical markers such as albumin reflect acute illness and inflammation as much as nutritional status. A composite approach is both more accurate and more actionable.
Clinical history and dietary assessment must cover: recent weight change (unintentional loss of ≥5% body weight over 6 months is the most sensitive single indicator of clinically significant malnutrition); dietary intake history including frequency of meals, types of food consumed, cooking ability, and food security; symptoms that impair intake (dysphagia, nausea, odynophagia, early satiety); medications that affect appetite or absorption; social factors (who buys and prepares food, meal companionship); and recent acute illness that may have increased catabolic demand.
Anthropometry:
- Body weight and BMI: BMI <20 kg/m² in the elderly indicates underweight and risk of malnutrition; however, BMI ≥22–27 is associated with lowest mortality in those over 70 years — the 'obesity paradox' of ageing means the thresholds shift upward.
- Mid-arm circumference (MAC): a surrogate for muscle mass; MAC <22 cm in women and <23 cm in men indicates significant depletion. It is particularly useful when accurate weight is unavailable (e.g., bedbound patients).
- Calf circumference: MAC <31 cm is an indicator of sarcopaenia and protein depletion in the elderly.
- Skin-fold thickness: triceps skinfold measured with Harpenden calipers estimates subcutaneous fat; age-adjusted reference values are used.
- Handgrip strength: measured with a handgrip dynamometer; <27 kg (men) or <16 kg (women) indicates probable sarcopaenia and is an independent predictor of hospital complications and mortality.
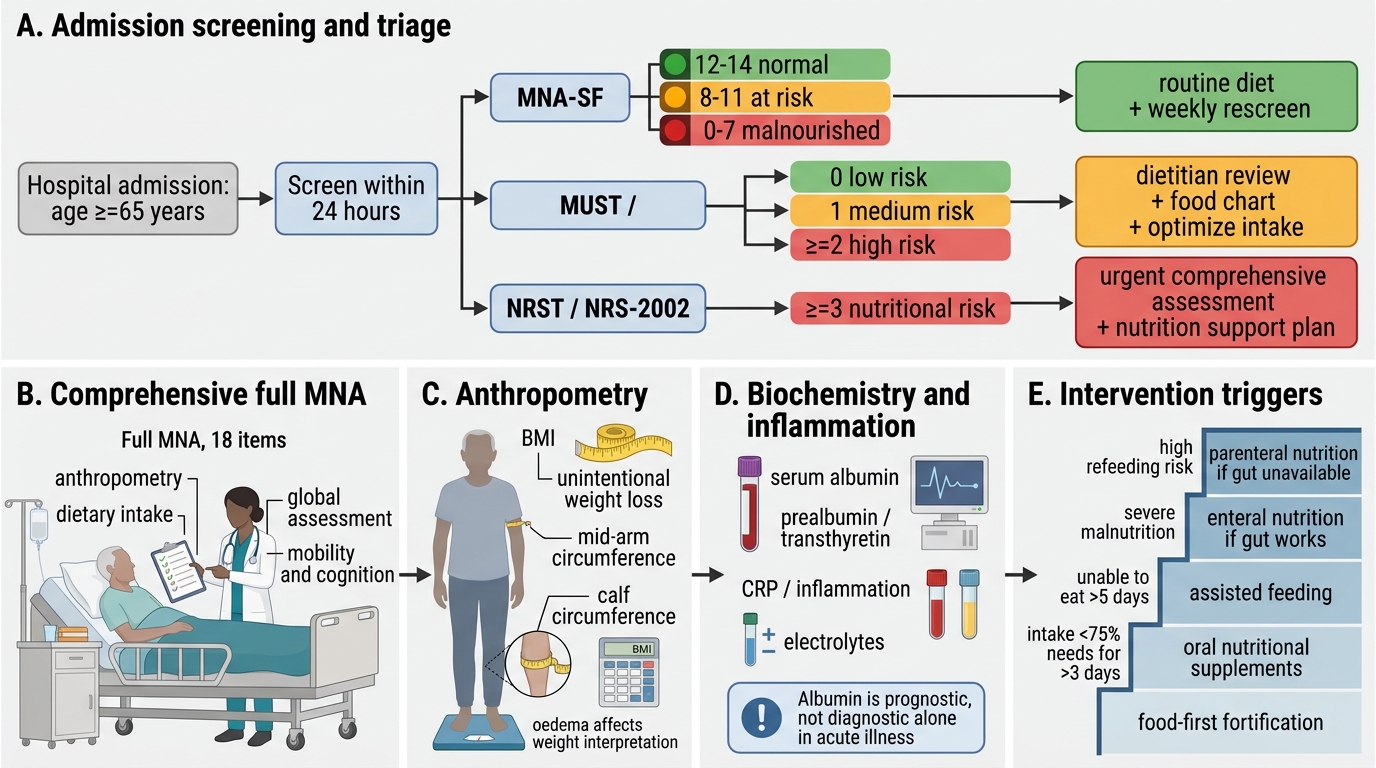
Nutritional Assessment Algorithm in Hospitalised Elderly Patients
Validated screening tools:
- Mini Nutritional Assessment (MNA): the most widely validated tool for geriatric nutritional screening. The MNA-SF (Short Form, 6 questions) is the recommended admission screen: scores 12–14 = normal nutritional status; 8–11 = at risk of malnutrition; 0–7 = malnourished. The full MNA (18 questions) provides comprehensive assessment of nutritional status, anthropometry, dietary assessment, and global assessment.
- MUST (Malnutrition Universal Screening Tool): widely used in UK and internationally for all adult inpatients; scores based on BMI, unintentional weight loss, and presence of acute disease causing reduced intake for >5 days.
- NRS-2002 (Nutritional Risk Screening 2002): preferred by ESPEN for hospitalised adults; combines nutritional status score with disease severity score; NRS ≥3 = at nutritional risk.
Biochemical markers:
- Serum albumin: <3.5 g/dL = mild hypoalbuminaemia; <3.0 g/dL = moderate; <2.5 g/dL = severe; reflects acute-phase response and illness severity as well as nutritional status — NOT a reliable marker of nutritional status in isolation during acute illness, but carries strong prognostic value.
- Serum prealbumin (transthyretin): shorter half-life (2–3 days vs 20 days for albumin) makes it a better marker of recent nutritional changes; <15 mg/dL = at risk.
- Serum transferrin: reflects iron stores as well as protein status.
- Specific micronutrient levels: serum 25-hydroxyvitamin D, B12, folate, iron/TIBC/ferritin, serum zinc.
- C-reactive protein (CRP): important to interpret alongside albumin — in acute inflammation, CRP rises and albumin falls as part of the acute-phase response, not necessarily indicating nutritional depletion.
- Total lymphocyte count: lymphopaenia (<1,500/mm³) is associated with malnutrition and impaired immunity.
SELF-CHECK
An 80-year-old hospitalised patient has serum albumin 2.8 g/dL and CRP 110 mg/L on day 2 of admission for community-acquired pneumonia. The MNA-SF score is 9 (at risk). Which interpretation is MOST accurate?
A. The low albumin confirms severe protein malnutrition requiring immediate enteral feeding
B. The low albumin is likely due to the acute-phase response from pneumonia alone and nutritional status is probably normal
C. The low albumin reflects both acute inflammation and possible underlying nutritional risk; the MNA-SF score should guide intervention, and nutritional support should be initiated alongside treatment of the pneumonia
D. Albumin is not useful in elderly patients and should not be checked
Reveal Answer
Answer: C. The low albumin reflects both acute inflammation and possible underlying nutritional risk; the MNA-SF score should guide intervention, and nutritional support should be initiated alongside treatment of the pneumonia
Albumin is a negative acute-phase reactant — it falls in response to systemic inflammation (e.g., pneumonia) independently of nutritional status. A low albumin in the context of high CRP therefore cannot be attributed solely to malnutrition. However, it does not mean nutritional status is normal either. The MNA-SF score of 9 (at risk) provides nutritional-specific evidence of risk. The correct interpretation integrates both: the low albumin carries prognostic significance regardless of cause, and the MNA-SF confirms nutritional risk requiring intervention. Nutritional support should be initiated — standard is to start oral nutritional supplements in those at risk, with escalation to enteral feeding if oral intake remains inadequate. Albumin is a valid prognostic marker in the elderly despite its confounding by acute inflammation.