Page 19 of 32
IM25.16 | Geriatric Rehabilitation — SDL Guide
Learning Objectives
- Describe the principles of evidence-based geriatric rehabilitation including task-specific training, high intensity, early mobilisation, and interdisciplinary integration
- Apply validated functional assessment tools (Barthel Index, FIM, Modified Rankin Scale, TUG, Berg Balance Scale) to quantify baseline disability and rehabilitation outcomes
- Describe the specific roles of physiotherapy and occupational therapy in geriatric rehabilitation and write a clinically adequate rehabilitation referral
- Identify and manage the major barriers to rehabilitation including post-stroke depression, pain, cognitive impairment, and spasticity
- Prescribe a rehabilitation plan for common geriatric contexts: post-stroke, post-hip fracture, and frailty/deconditioning
- Describe the components of social rehabilitation including community physiotherapy, day hospitals, and carer support
INSTRUCTIONS
This module uses the IM-skills arc to build practical rehabilitation competency: from the clinical indication and principles, through the functional assessment tools that measure progress, to the specific physiotherapy and OT interventions, and finally to prescribing a complete rehabilitation plan with measurable goals and discharge criteria. Rehabilitation is not passive care — it is the most active and evidence-driven intervention in geriatric medicine.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 16 — Principles of Rehabilitation Medicine (textbook)
- API Textbook of Medicine, 11th ed., Chapter on Geriatric Rehabilitation (textbook)
- Royal College of Physicians: National Clinical Guideline for Stroke (5th edition, 2016) (guideline)
- FLAME Trial: Chollet et al., Lancet Neurology 2011 — Fluoxetine for motor recovery after acute ischaemic stroke (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Murugadoss, 80 years old, is on day 5 of his admission following a right MCA ischaemic stroke. He has left hemiparesis (MRC grade 2 in left arm, 3 in left leg), dysphagia requiring thickened fluids, and aphasia that has partly improved. His blood pressure is controlled. The medical team has stabilised the acute event. The senior registrar writes in the notes: 'Medically stable — arrange rehabilitation.' The physiotherapist arrives and asks the question that distinguishes rehabilitation from maintenance: 'What is his goal? Does he want to walk to the bathroom independently, go home to his wife, or attend his granddaughter's wedding in three months?' The answer shapes the rehabilitation prescription. Rehabilitation in geriatric medicine is not a passive process of waiting for recovery — it is an active, goal-directed, evidence-based clinical discipline that exploits neuroplasticity, restores function, prevents secondary complications, and returns the person to their meaningful life. This module builds the knowledge and skills framework for prescribing, monitoring, and evaluating rehabilitation for elderly patients.
WHY THIS MATTERS
Disability is the final common pathway of geriatric disease. Whether the primary event is stroke, hip fracture, COPD exacerbation, major surgery, or a simple fall — the resulting loss of functional independence is the outcome that most impacts quality of life, necessitates institutional care, and predicts mortality. Rehabilitation is the systematic process of reversing that disability by restoring function through targeted intervention by a multidisciplinary team. NMC competency IM25.16 requires KH-level understanding of the principles of physical and social rehabilitation, functional assessment, and the roles of physiotherapy and occupational therapy in the management of disability in the elderly — competencies that every physician will need in every clinical specialty.
RECALL
Activate your understanding of the physiological basis for rehabilitation. Neuroplasticity — the brain's ability to reorganise neural connections in response to experience, training, and injury — is the physiological foundation of stroke rehabilitation. Even after infarction, peri-infarct cortex can reorganise to partially assume functions of the damaged area, especially when driven by intensive repetitive task-specific training. The use-it-or-lose-it principle: disuse atrophy of both neural circuits and muscle occurs rapidly with immobility; early mobilisation counteracts this. Muscle physiology: type II fast-twitch fibres (power, explosive movement) are lost preferentially with ageing and immobility (sarcopenia); type I slow-twitch fibres (endurance) are relatively preserved. Resistance training specifically targets type II fibre recovery. Recall the International Classification of Functioning, Disability and Health (ICF) framework (WHO 2001): rehabilitation operates at three levels — impairment (organ/system dysfunction), activity limitation (difficulty performing tasks), and participation restriction (inability to engage in life roles).
Clinical Indication and Principles of Geriatric Rehabilitation
Geriatric rehabilitation is indicated whenever functional decline — in mobility, self-care, communication, or community participation — follows disease, injury, or surgical intervention in an elderly person who has potential for improvement. The breadth of indication is intentionally wide because the goal of geriatric medicine is to maximise function and quality of life, not merely to treat disease. The major clinical contexts requiring formal rehabilitation are: stroke (the most rehabilitation-intensive condition; goal is to maximise neurological recovery and functional independence within the constraints of the infarct size and location); hip fracture and orthopaedic surgery (restoration of gait, mobility, and ADL function after surgical fixation or arthroplasty); COPD exacerbation (pulmonary rehabilitation to restore exercise capacity and breathlessness control); cardiac events (cardiac rehabilitation post-MI or post-cardiac surgery); frailty and deconditioning (progressive exercise to reverse sarcopenia and improve balance in community-dwelling or long-term care residents); cognitive impairment (cognitive rehabilitation alongside physical rehabilitation in post-delirium recovery and early dementia); and neurological diseases (Parkinson disease, peripheral neuropathy — physiotherapy for gait and balance, speech therapy for dysarthria/dysphagia).
The principles that distinguish evidence-based rehabilitation from the vague injunction to 'get them moving': (1) Task-specific training — rehabilitation exercises must replicate the functional tasks the patient wants to perform (walking rehabilitation uses actual walking, not just leg exercises in bed); neuroplasticity is maximised by practising the specific activity. (2) High intensity — the dose of rehabilitation (frequency × duration × repetitions) is the strongest predictor of outcome; the VECTORS, EXCITE, and ICARE trials in stroke rehabilitation demonstrated that higher-intensity practice produces superior motor recovery. (3) Early mobilisation — starting within 24–48 hours of medical stability reduces hospital complications (VTE, pressure ulcers, aspiration, delirium) and accelerates recovery; the very concept of 'bed rest' as a therapeutic intervention is largely obsolete in geriatric medicine. (4) Interdisciplinary integration — the team does not work in parallel silos; goals, progress, and care plans are shared, communicated daily, and adjusted collectively. (5) Patient-centred goal setting — rehabilitation goals must reflect the patient's own values and priorities (returning to driving, attending a family event, cooking independently); standardised functional assessments provide the baseline and outcomes framework, but the motivating goal is personal. (6) Adaptability and home preparation — rehabilitation must prepare the patient's home environment (grab bars, raised toilet seats, ramp, doorframe widening) alongside preparing the patient themselves.
The rehabilitation team: In the hospital setting, the core interdisciplinary team includes: the geriatrician/physician (overall medical management, comorbidity control, medication review, discharge coordination, goals-of-care discussions); physiotherapist (mobility, gait, balance, respiratory physiotherapy, muscle strengthening, hydrotherapy); occupational therapist (OT) (ADL retraining, home assessment, adaptive equipment, cognitive-perceptual assessment, driving re-assessment); speech and language therapist (SLT) (aphasia, dysphagia assessment and management, communication aids); clinical neuropsychologist (formal cognitive assessment, psychological barriers to rehabilitation, post-stroke depression and anxiety); rehabilitation nurse (continence management, skin integrity, medication adherence, patient and family education); social worker (discharge planning, community services, financial entitlements, carer support); and dietitian (nutritional optimisation for recovery, dysphagia diet textures, nutritional supplements). In the Indian public hospital context, this full team may not be available — the physician must then function as the coordinator and advocate, requesting the available allied health professionals and adapting rehabilitation to available resources.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
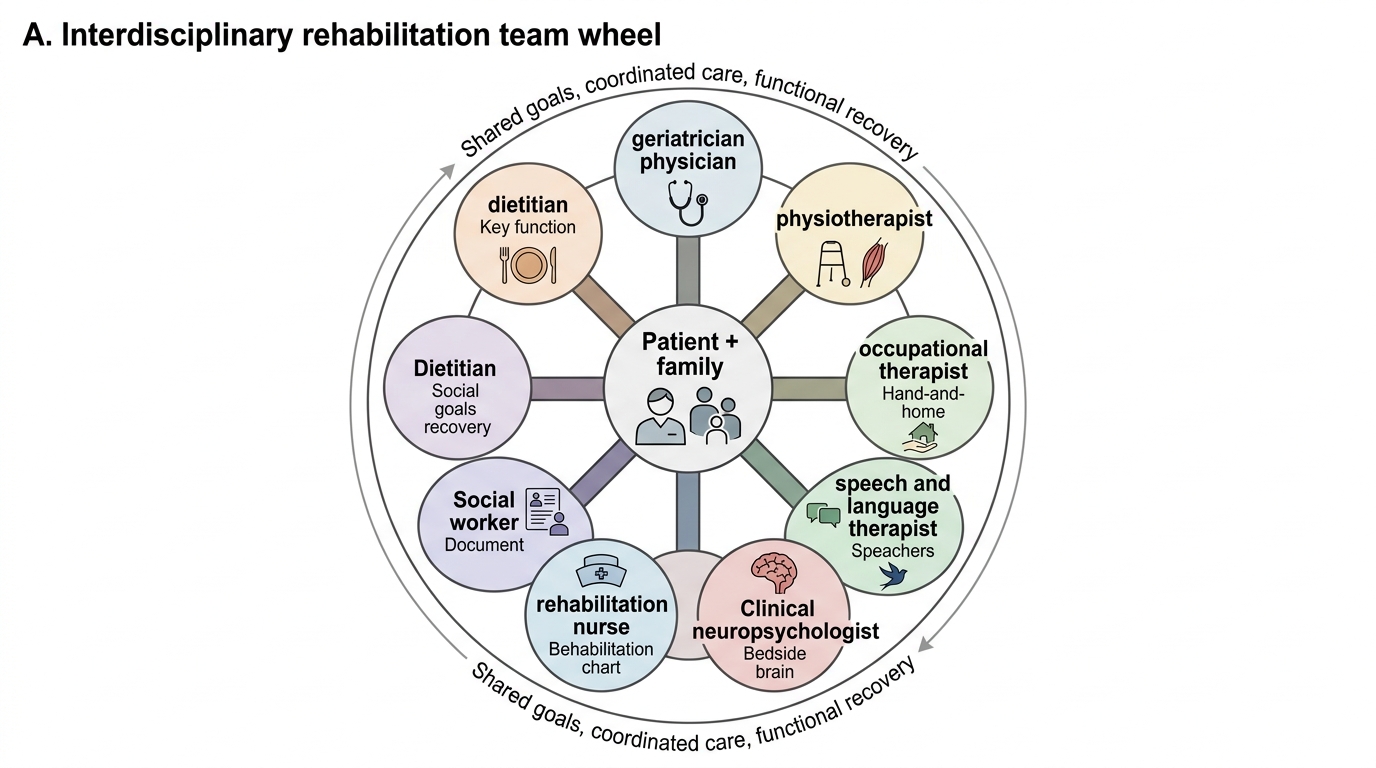
Interdisciplinary Geriatric Rehabilitation Team
Functional Assessment Tools in Rehabilitation
Functional assessment is the language of rehabilitation — it provides objective measurement of where the patient is, where they need to get to, and whether the rehabilitation programme is working. Every rehabilitation encounter must begin with a structured functional assessment and document outcomes with validated instruments. The key principle: functional status must be measured, not estimated. Clinical impressions of function ('seems to be improving') are inadequate for decision-making; validated scales provide reproducible, documentable, and communicable data.
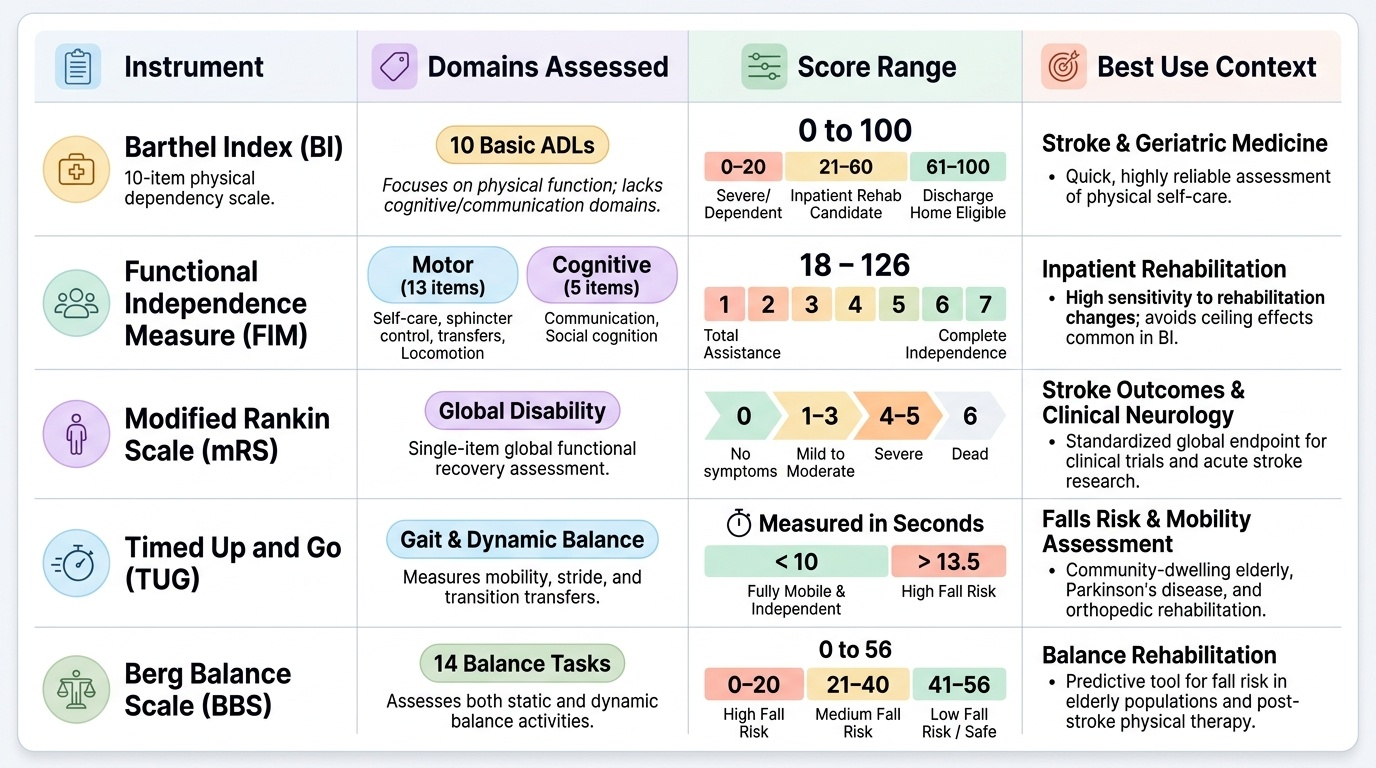
Provided image
The Functional Independence Measure (FIM) is the most widely used standardised rehabilitation outcome measure internationally. It rates independence in 18 activities across 6 domains (self-care, sphincter control, transfer, locomotion, communication, social cognition), each scored 1–7 (1 = total assistance; 7 = complete independence). Total score 18 (total dependence) to 126 (complete independence). The FIM is completed by the MDT based on actual observation of the patient performing the activities. Its key strength: sensitivity to rehabilitation change (it detects improvement that the Barthel Index may miss because of ceiling effects).
Barthel Index (BI) — the most widely used outcome measure in stroke rehabilitation and in geriatric medicine generally. Assesses 10 activities: feeding, bathing, grooming, dressing, bowel continence, bladder continence, toilet use, bed-to-chair transfer, mobility, and stair climbing. Scores range 0–100; 0 = totally dependent; 100 = fully independent. The BI is quick to administer and has excellent reliability. Key thresholds: BI >60 = likely to be discharged home; BI 20–60 = likely to benefit substantially from inpatient rehabilitation; BI <20 = most severely disabled, requiring intensive support. The BI does not capture communication or cognitive domains — the FIM is more comprehensive.
Modified Rankin Scale (mRS) — a 7-point global disability scale used primarily in stroke outcomes research and clinical neurology: 0 = no symptoms; 1 = no significant disability; 2 = slight disability — independent with previous activities; 3 = moderate disability — requires help but independent in walking; 4 = moderately severe — unable to walk unassisted, and unable to attend to bodily needs without assistance; 5 = severe disability — requires nursing care; 6 = dead. An mRS ≤2 at 3 months post-stroke is the standard definition of 'good functional outcome' in clinical trials. It is simple, widely understood, and communicates functional status across the stroke team.
The Timed Up and Go (TUG) test — primary mobility and fall-risk assessment (described in the musculoskeletal module); also a rehabilitation outcome measure for tracking gait recovery after stroke, hip fracture, or frailty intervention. Normal <12 seconds.
Berg Balance Scale (BBS) — 14 functional balance tasks (standing unsupported, sit-to-stand, reaching forward, picking up object from floor, tandem stance, single-leg stance, turning 360°), each 0–4 (total 0–56); <45 = fall risk; often used to track balance recovery in stroke and orthopaedic rehabilitation.
Frenchay Aphasia Screening Test (FAST) — validated 3-minute bedside aphasia screen used by non-SLTs; detects significant aphasia and guides referral to speech and language therapy.
The rehabilitation team reviews outcome measures at least weekly; lack of progress (plateau) over 2–3 weeks triggers reassessment of goals, rehabilitation dose, and barriers to progress (undertreated depression, cognitive impairment, pain, inadequate nutrition, medical instability, or unrealistic goal-setting).
Physiotherapy and Occupational Therapy in Geriatric Rehabilitation
Physiotherapy and occupational therapy are the two core disciplines of physical rehabilitation. While their domains overlap and they share goals, their theoretical bases and practical interventions are complementary and distinct. Understanding both roles enables the physician to write coherent rehabilitation referral requests, monitor progress appropriately, and participate meaningfully in MDT goal-setting.
Physiotherapy in geriatric rehabilitation addresses the physical impairments and activity limitations that prevent independent function. The core physiotherapy interventions in the elderly are:
Gait and mobility rehabilitation: Normal bipedal walking requires coordinated input from multiple systems — motor cortex (voluntary movement), cerebellum (coordination and timing), basal ganglia (rhythm and automation), vestibular system (balance), proprioceptive afferents (limb position sense), and visual input. Stroke, Parkinson disease, cerebellar ataxia, vestibular dysfunction, peripheral neuropathy, and musculoskeletal disease each produce characteristic gait abnormalities: hemiparetic gait (circumduction of paretic leg, reduced arm swing); parkinsonian gait (shuffling, flexed posture, festination, freezing); ataxic gait (wide-based, unsteady, arms outstretched for balance); antalgic gait (painful limb — short stance phase on affected side). Treatment: task-specific walking practice (treadmill training with or without body-weight support; overground walking in progressively challenging environments); Constraint-Induced Movement Therapy (CIMT) for upper limb hemiparesis (constraining the unaffected arm forces use of the paretic arm — drives neuroplasticity); ankle-foot orthosis (AFO) for foot drop.
Balance rehabilitation: Balance exercises exploit the same plasticity that drives motor recovery. The programme is progressive: from sitting balance, to standing with support, to tandem standing, to single-leg stance, to dynamic balance (stepping over objects, walking on varied surfaces). The Otago Exercise Programme (leg strengthening and balance exercises — described in the musculoskeletal module) reduces falls by 35% in community-dwelling elderly. Vestibular rehabilitation therapy (VRT) — specific for benign paroxysmal positional vertigo (BPPV, the Epley manoeuvre) and for chronic vestibular hypofunction (gaze stabilisation exercises, habituation exercises).
Respiratory physiotherapy: In post-operative patients and COPD exacerbation, respiratory physiotherapy uses active cycle of breathing techniques (ACBT), airway clearance (percussion, vibration, postural drainage), incentive spirometry, and directed coughing to mobilise secretions, prevent atelectasis, and improve respiratory muscle endurance. In pulmonary rehabilitation for COPD: aerobic training (walking, cycling) at 60–70% maximum heart rate for ≥20 minutes, 3 times per week, for ≥6 weeks — the evidence-based protocol.
Occupational therapy (OT) focuses on enabling the patient to perform the occupations (activities, tasks, roles) that are meaningful to them. OT in geriatric rehabilitation encompasses:
ADL retraining: Teaching adaptive techniques for performing dressing, bathing, toileting, cooking, and other ADLs despite residual physical or cognitive impairment. Examples: one-handed dressing technique for hemiparesis; non-slip mats and grab bars for bath; long-handled reachers and sock aids for patients with hip arthroplasty who cannot flex beyond 90 degrees; weighted utensils for patients with tremor (Parkinson disease).
Assistive technology: Prescribing and training in the use of assistive devices: walking aids (Zimmer frame, rollator, elbow crutches — each with specific indication and gait implication); wheelchair prescription and postural management (correct pressure cushion and tilt for those who will use a wheelchair long-term); cognitive aids (electronic calendars, medication reminder systems for patients with mild dementia).
Home assessment and environmental modification: The OT home visit (or virtual assessment) identifies and addresses barriers to safe independent living: removal of floor-level hazards (rugs, cords), installation of grab rails (bathroom, toilet, stair), adequate lighting, ramp for wheelchair access, kitchen adaptation. This is one of the highest-value interventions in preventing falls and delaying institutionalisation.
Vocational and leisure rehabilitation: For elderly patients who were employed or actively engaged in community activities — assessing and facilitating return to driving (standardised driving assessment), gardening, crafts, or community groups as part of meaningful occupation and mental health recovery.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
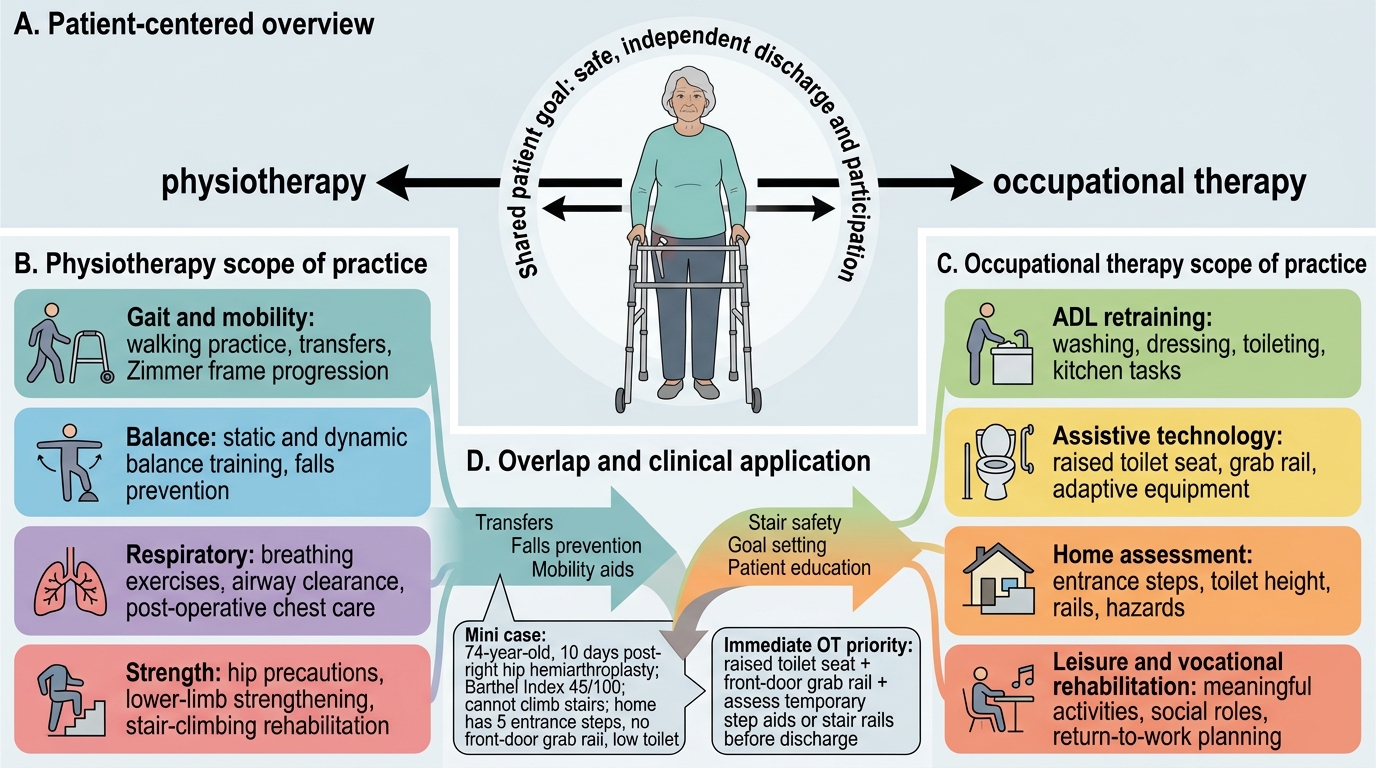
Physiotherapy and Occupational Therapy in Geriatric Rehabilitation
SELF-CHECK
A 74-year-old woman is 10 days post-right hip hemiarthroplasty for a neck of femur fracture. She can stand with a Zimmer frame but cannot climb stairs. Her Barthel Index is 45/100. The physiotherapist reports she has achieved her short-term goal (standing and transferring safely) and can progress to stair-climbing rehabilitation. The occupational therapist has visited her home and identified: no grab rail at the front door, five steps to the entrance, and a low toilet. Which of the following BEST describes the most impactful immediate OT intervention?
A. Arrange transfer to a residential nursing home since she cannot manage stairs
B. Provide a raised toilet seat and arrange installation of a front door grab rail and assess for temporary step-climbing aids or stair rails before discharge
C. Prescribe a motorised stair lift as the definitive solution
D. Delay discharge until Barthel Index reaches 80/100
Reveal Answer
Answer: B. Provide a raised toilet seat and arrange installation of a front door grab rail and assess for temporary step-climbing aids or stair rails before discharge
Occupational therapy home assessment identifies modifiable barriers to independent living; the interventions here are: raised toilet seat (reduces hip flexion beyond 90 degrees — a standard hip arthroplasty precaution), grab rail at the front door (provides safe entry and exit), and assessment of the five entry steps (options: stair rail, OT-guided stair practice with physiotherapy, or temporary step-climbing aids if available). These are standard OT rehabilitation interventions that enable discharge to home — the goal. Residential nursing home is premature for a Barthel of 45 with active rehabilitation potential. A stair lift is a permanent home modification that requires far more assessment and is expensive. Delaying discharge until BI 80 is not evidence-based and prolongs hospital risks (delirium, infection).