Page 17 of 32
IM25.{15,17} | Geriatric Sensory Loss — SDL Guide (Part 2)
Integrated Geriatric Management: Rehabilitation and Prevention
Restoring sensory function in the elderly requires more than a surgical or pharmaceutical prescription — it demands an integrated management approach that addresses the downstream consequences of sensory loss (falls, depression, social isolation) alongside the sensory deficits themselves. The concept of sensory rehabilitation extends from the immediate technical intervention (hearing aid fitting, cataract surgery, anti-VEGF injections) to the broader functional and psychological recovery that enables the patient to re-engage with daily life, social participation, and independent living.
Low-vision rehabilitation for irreversible visual impairment (advanced dry AMD, diabetic maculopathy, post-glaucoma field loss) encompasses a range of assistive strategies: high-contrast large-print materials; magnifying glasses and stand-mounted magnifiers; illuminated magnifiers for reading; eccentric viewing training (teaching patients with central scotoma to use peripheral vision for tasks); talking clocks, talking mobile phones, and screen-reader software; home hazard modification by occupational therapist (remove tripping hazards, improve lighting levels to compensate for reduced pupil size and contrast sensitivity); and orientation and mobility training (white cane use for outdoor navigation in those with severe visual loss). The National Programme for Control of Blindness and Visual Impairment (NPCB+VI) provides free cataract surgery and glasses at district hospitals across India — awareness of this pathway is critical for referring elderly patients who cannot afford private care.
Hearing rehabilitation beyond hearing aids: After hearing aid fitting, realistic expectation setting is essential — modern digital hearing aids provide significant benefit but do not restore normal hearing; the elderly require 4–6 weeks of adaptation to adjust to amplified sound (the brain must relearn to interpret amplified signals, particularly after years of sensory deprivation). Auditory training programmes — structured exercises to improve speech discrimination and listening in background noise — are available as smartphone apps and in structured programmes. Communication strategies for the hearing-impaired: speak face-to-face (lip-reading supplements hearing), reduce background noise, speak clearly and at moderate pace (not shouting — which distorts speech), and use written communication for complex instructions in healthcare settings. Telephone captioning services and loop systems in public spaces restore telephone and community participation.
Preventing sensory loss: Primary prevention is partially achievable. Hearing protection (ear muffs, plugs) for occupational noise exposure — recommended by the Occupational Safety and Health Administration for environments >85 dB. Avoidance of ototoxic drugs where possible; if aminoglycosides are unavoidable, monitor serum levels and use minimum effective duration. Sun protection for AMD risk reduction (ultraviolet light exposure is a risk factor for dry AMD). Smoking cessation (smoking doubles AMD risk and accelerates cataract development). Strict glycaemic control for diabetic retinopathy prevention. Regular blood pressure control (reduces risk of hypertensive retinopathy). Regular eye examinations from age 60 (annually if diabetic or glaucoma suspect).
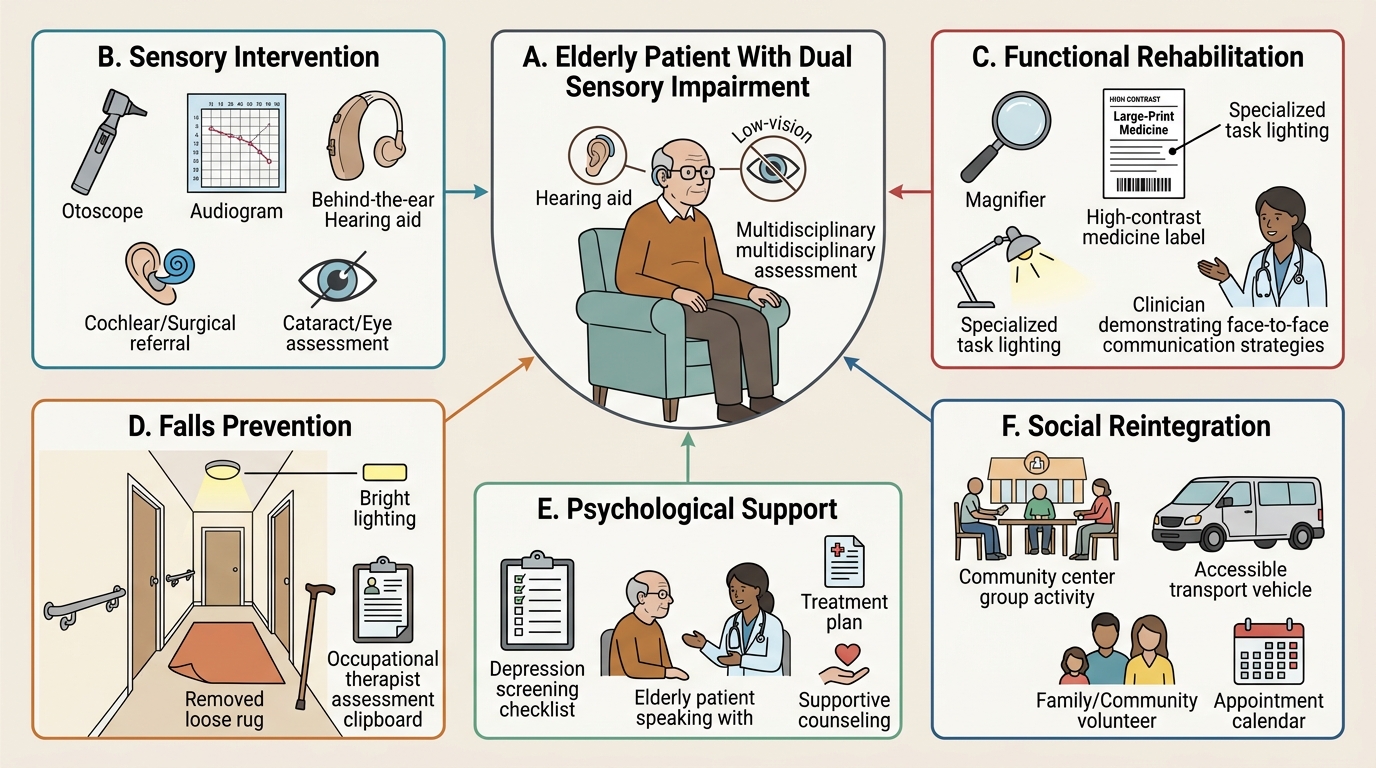
Integrated Rehabilitation Plan for Dual Sensory Loss in Geriatrics
Self-Assessment: Sensory Loss in Geriatric Practice
The following scenarios integrate the clinical assessment, diagnosis, and management frameworks from this module. Apply the sensory examination and diagnostic criteria before reading the analysis.
Scenario A: Rajan, 74 years old, retired auto-mechanic, presents with bilateral hearing difficulty worsening over 5 years. Rinne test: positive bilaterally (air > bone bilaterally — SNHL pattern). Weber test: lateralises to the right. No discharge, no vertigo, no tinnitus described. He asks if a hearing aid will help. What additional investigation is needed before prescribing a hearing aid, and what finding would change your management?
Analysis: The Weber lateralising to the RIGHT (the 'better' side) is the pattern of SNHL (lateralises to better ear in SNHL, because bone conduction is relatively better in the ear with better cochlear function — the right ear in this case, suggesting LEFT ear SNHL is slightly worse). Audiometry is needed to quantify the degree and frequency pattern of hearing loss and provide the fitting parameters for a hearing aid. The key concerning finding that would change management: asymmetrical SNHL — if audiometry shows significantly more loss in one ear (>15 dB interaural asymmetry) or unilateral sudden SNHL, MRI of the internal auditory meatus is indicated to exclude acoustic neuroma (vestibular schwannoma). In this case, Weber lateralises to the right (better ear), suggesting the left is worse — a 5-year history with asymmetry warrants audiometry with careful comparison between ears. If symmetric: fit bilateral hearing aids (both ears — monaural fitting is inferior for speech discrimination and localisation in background noise).
Scenario B: Mrs Anasuya, 72 years old, Type 2 diabetes for 15 years (HbA1c 9.2%), presents with reduced vision in the right eye over 3 months. She reports the vision is 'foggy in the centre' and straight lines appear wavy when she looks with her right eye. Fundoscopy by her GP showed 'something unusual at the back of the eye' and she was referred. VA: 6/36 right eye, 6/12 left eye. What is the most likely diagnosis and what constitutes the emergency component of her care?
Analysis: Wet AMD in the right eye (sudden/subacute central vision loss, metamorphopsia — wavy lines — is the classic symptom of choroidal neovascularisation affecting the macula). The combination of diabetes AND age makes both diabetic macular oedema (left eye — HbA1c 9.2% and 6/12) and wet AMD (right eye — wavy lines, more acute onset) possible. The emergency: wet AMD causing rapid central vision loss is a vitreo-retinal emergency — anti-VEGF injection (ranibizumab or bevacizumab) must be started within days; every week of delay with active choroidal neovascularisation leads to permanent scarring of the macula. Refer immediately to vitreoretinal specialist. Simultaneously: optimise glycaemic control (HbA1c 9.2% — diabetic retinopathy risk is high); left eye requires dilated fundal examination for diabetic changes.
Scenario C: Mrs Savithri, 80 years old, lives alone. Her daughter reports she recently stopped going to temple (couldn't follow the service), stopped using the telephone (can't hear callers), and has become withdrawn and tearful. She scored 7/15 on GDS. She has not had a hearing assessment. Her GP attributed the withdrawal to 'normal ageing.' What is the priority intervention and how does it address the psychiatric comorbidity?
Analysis: Presbycusis causing social isolation, functional dependence, and secondary depression — this is the sequence: untreated hearing loss → communication failure → social withdrawal → depression → further isolation. The GP's attribution to 'normal ageing' is incorrect — hearing loss is a treatable cause of this presentation. Priority: formal pure-tone audiometry + hearing aid fitting as the primary intervention; bilateral digital hearing aids will improve communication, facilitate return to temple and telephone use, and reduce isolation. Secondary depression (GDS 7 = probable depression): antidepressant (SSRI — escitalopram/sertraline) + referral for social engagement and reminiscence therapy, with review after hearing rehabilitation. The interaction between sensory loss and depression is bidirectional — treating the hearing loss often produces substantial mood improvement in addition to SSRI therapy. She should be informed that hearing aids take 4–6 weeks of adaptation before their full benefit is experienced.
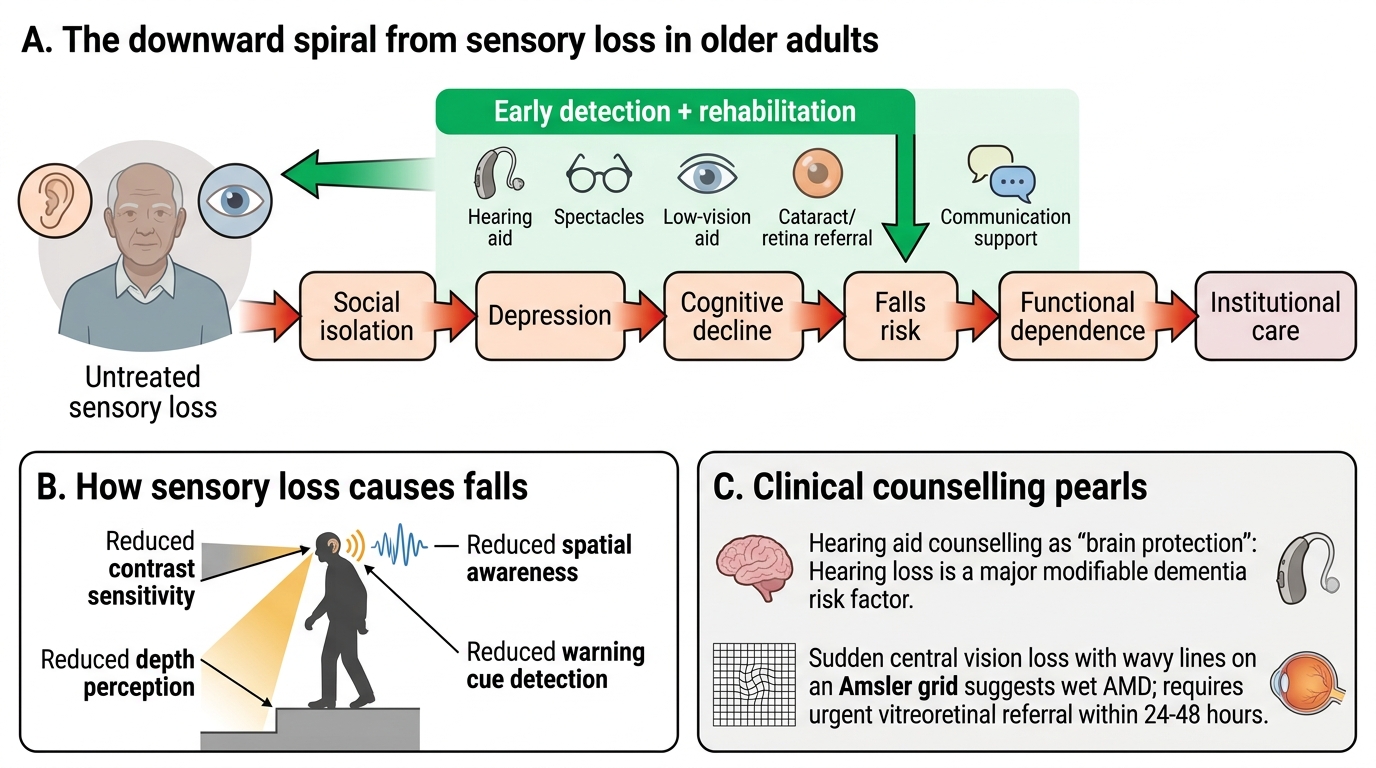
Sensory Loss Impact Cascade in Older Adults
CLINICAL PEARL
Two pearls that define clinical competence in geriatric sensory loss: (1) Hearing loss is the single largest modifiable risk factor for dementia (Lancet Commission on Dementia Prevention, 2020 and 2024). Early hearing aid fitting reduces cognitive decline rates — this framing transforms hearing aid counselling from 'help with hearing' to 'brain protection.' Elderly patients who refuse hearing aids because of stigma or denial deserve to know this evidence. (2) Wet AMD causing sudden central vision loss with metamorphopsia is a time-sensitive emergency — every week without anti-VEGF treatment leads to permanent scarring. The classic symptom is straight lines appearing wavy on the Amsler grid. Any elderly patient complaining of sudden central vision loss or distorted straight lines must be referred to vitreoretinal services within 24–48 hours, not at the next available routine ophthalmology slot.