Page 22 of 32
IM25.19-21 | Geriatric Social and Ethical Care — SDL Guide
Learning Objectives
- Enumerate and describe the social problems of elderly patients including isolation, abuse, and changing family structures
- Describe available social interventions — domiciliary services, rehabilitation facilities, old-age homes, and state programmes
- Apply ethical principles of autonomy, beneficence, non-maleficence, and justice to clinical decisions in elderly care
- Discuss capacity assessment, informed consent, and advance directives in the elderly
- Identify indicators of elder abuse and describe appropriate clinical and legal responses
INSTRUCTIONS
Geriatric social and ethical care addresses the non-biomedical dimensions of ageing that profoundly determine health outcomes. Social isolation, elder abuse, eroding family structures, and a complex ethical landscape around autonomy and capacity challenge every clinician who cares for older adults. This module equips you to recognise these problems, navigate available social interventions in the Indian context, and reason clearly through ethical dilemmas — skills as essential as any clinical skill in geriatric practice.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 13 — Care of the Older Adult (textbook)
- API Textbook of Medicine, 10th ed., Section on Geriatrics (textbook)
- WHO Global Strategy and Action Plan on Ageing and Health 2016–2020 (guideline)
- Maintenance and Welfare of Parents and Senior Citizens Act, 2007 (India) (policy)
- National Policy for Older Persons (NPOP), Ministry of Social Justice and Empowerment, India, 1999 (revised 2011) (policy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Gopal, 74 years old, is brought to the emergency department by a neighbour after being found confused and malnourished in his apartment. His children live in another city. His daughter, reached by phone, tells you he is 'difficult' and has been refusing help. On examination he has multiple bruises in different stages of healing on his arms and back. When the neighbour steps outside, Gopal becomes tearful and says, 'They come sometimes and take my pension money.' Is this abuse? Does Gopal have the capacity to refuse hospitalisation? Who has the right to make decisions for him if he lacks capacity? What services exist in India to protect him? These questions sit at the intersection of social medicine and clinical ethics — the domain of geriatric social and ethical care. The clinician who can answer them is equipped not merely to treat Gopal's acute illness but to protect his dignity, safety, and right to self-determination.
WHY THIS MATTERS
India's elderly population — those aged 60 and above — numbered approximately 138 million in 2021 and is projected to reach 300 million by 2050, making India's ageing transition one of the most consequential demographic shifts in history. Yet the social infrastructure for older adults remains fragile. Nuclear family migration, urbanisation, and changing gender roles have eroded the joint family system that was the traditional safety net for India's elderly. Against this backdrop, social isolation, financial dependence, elder abuse, and inadequate care are not rare edge cases but systemic realities that every physician in India will encounter. For the NMC competencies IM25.19–IM25.21, you must be able to enumerate social problems, describe social interventions, and discuss ethical issues — at the KH (Knowledge and Understanding applied in clinical scenarios) level. The ability to conduct a social screen, identify abuse, and initiate an appropriate ethical response is a core clinical skill.
RECALL
Activate your prior knowledge before proceeding. The Comprehensive Geriatric Assessment (CGA) you studied in the geriatric foundations module explicitly includes a social domain — it evaluates family and caregiver support, living situation, financial resources, and cultural factors alongside the medical and functional domains. You will also apply four principles of biomedical ethics established by Beauchamp and Childress: (1) autonomy — the patient's right to make informed decisions about their own care; (2) beneficence — the duty to act in the patient's best interest; (3) non-maleficence — the duty to avoid harm; and (4) justice — fair distribution of resources and equitable treatment. In geriatric care, these four principles frequently create tension with each other — a patient may refuse care that is clearly beneficial, or a family may demand interventions that cause more harm than good. Recall also the Mental Capacity Act principles: capacity is decision-specific, time-specific, and presumed present unless demonstrated otherwise.
Social Problems of the Elderly: Isolation, Abuse, and Family Change
The social problems of elderly patients are not merely background context — they are primary determinants of health outcomes, hospital re-admission rates, and mortality. Understanding them is the first step in the IM-skills arc of clinical indication and relevance: the clinician must know why these problems arise and what they look like clinically before attempting any intervention.
Social isolation is one of the most prevalent and harmful social conditions affecting older adults. It is defined as objective lack of social contact (social isolation) and subjective experience of loneliness — though the two often coexist. In India, the joint family system historically provided a natural buffer against isolation, but urban migration, nuclear family formation, and increasing geographical dispersion have progressively eroded this structure. Elderly spouses increasingly live alone after a partner's death; widows in India face particular vulnerability due to cultural marginalisation and financial dependence. The health consequences of social isolation are well-documented and severe: increased all-cause mortality (comparable in magnitude to smoking 15 cigarettes per day, per meta-analyses), accelerated cognitive decline, depression, anxiety, impaired immune function, and delayed recovery from illness. Isolated older adults are also more likely to present late to medical services, less likely to adhere to treatment, and more likely to be institutionalised. The UCLA Loneliness Scale and similar instruments can quantify isolation, but clinical screening need not be complex — simply asking 'Do you have someone to talk to when you are worried?' and 'How often do you see family or friends?' captures the essential information.
Elder abuse is a single or repeated act — or lack of appropriate action — occurring within a relationship where there is an expectation of trust, causing harm or distress to an older person. The World Health Organization recognises six forms of elder abuse: (1) physical abuse — hitting, slapping, burning, improper physical restraint; (2) psychological or emotional abuse — intimidation, humiliation, verbal aggression, threats, and coercive control; (3) financial or material abuse — theft, misuse of funds, exploiting power of attorney; (4) sexual abuse — non-consensual sexual contact; (5) neglect — failure to provide adequate food, shelter, medical care, or supervision; and (6) abandonment — desertion by caregiver. In the Indian context, financial abuse — particularly misappropriation of pension, property, or savings by family members — is particularly prevalent and often under-reported due to the victim's dependence on the perpetrator, cultural norms of family loyalty, and fear of worse consequences if they speak out. The prevalence of elder abuse in India is estimated at 14–23% in community surveys, with substantially higher rates in institutional settings. Physical indicators include unexplained bruises in unusual locations, fractures inconsistent with stated mechanism, pressure sores from neglect, and malnutrition. Behavioural indicators include fearfulness in the presence of a specific caregiver, withdrawal, and inconsistency between the patient's and caregiver's accounts. The EASI (Elder Abuse Suspicion Index) is a validated 6-item screening tool that can be administered in a clinical consultation.
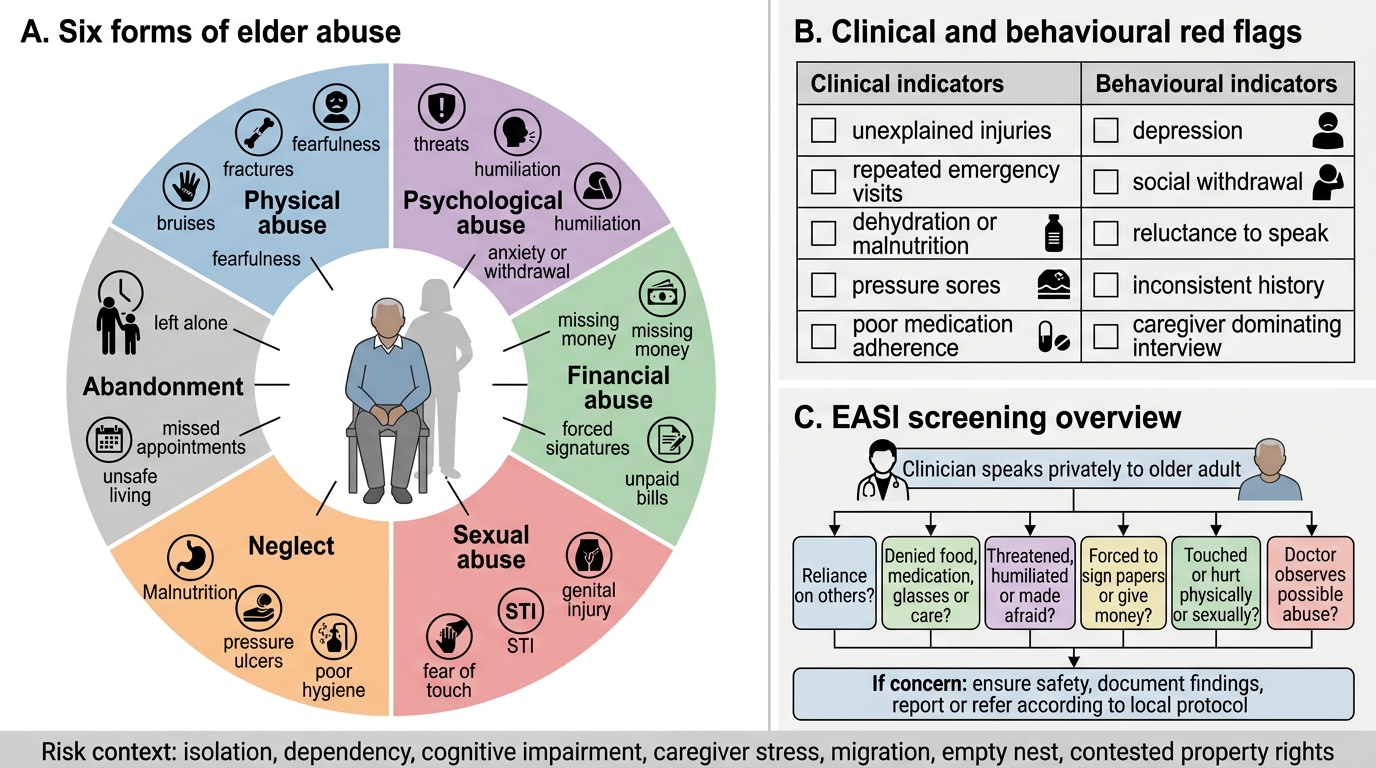
Elder Abuse: Forms, Red Flags, and EASI Screening
Changing family structure is the structural underpinning of many of the above problems. The shift from the joint family (multigenerational co-residence with shared resources and mutual support) to nuclear family units has left many older adults without the automatic caregiving that traditional Indian society assumed. Contributing factors include rural-to-urban migration for employment, women's increasing workforce participation (who were the traditional family caregivers), smaller family sizes, and increasing life expectancy creating a 'sandwich generation' that simultaneously cares for children and parents. Additionally, the changing status of elderly women is particularly concerning: widows face social restrictions, re-marriage stigma, property rights that are still contested in practice, and economic dependency that increases vulnerability to abuse. The 'empty nest' phenomenon — elderly couples left alone after adult children migrate — is now common in tier-2 and tier-3 Indian cities, creating a cohort of older adults with intact physical health but profound social vulnerability.
Social Interventions: Domiciliary Services, Residential Care, and State Programmes
Governing principles for social interventions in elderly care are grounded in two overarching values: enabling the maximum possible ageing-in-place (remaining in one's own home and community for as long as safely possible), and ensuring a spectrum of alternatives when home care is no longer adequate. The clinician must know this spectrum — from minimal support at home through supported housing to full institutional care — in order to match the level of intervention to the patient's need, preference, and available resources.
Domiciliary (home-based) services represent the first tier of social intervention and are generally the preferred option for both patients and healthcare systems. They include: (a) home health aides and personal care attendants who assist with ADLs (bathing, dressing, feeding, toileting, mobility) and IADLs (medication management, meal preparation, shopping, housekeeping); (b) domiciliary nursing visits for wound care, injection administration, and monitoring; (c) physiotherapy and occupational therapy at home for post-hospitalisation rehabilitation; (d) meals delivery programmes (such as Anganwadi-linked or NGO-run tiffin services) that ensure nutritional security; (e) telehealth and remote monitoring — increasingly available via smartphone-based platforms; and (f) befriending and social support volunteers to address isolation. In India, home health aide infrastructure is largely in the informal sector, with variable training and quality; several NGOs (e.g., HelpAge India, Silver Innings) operate structured domiciliary services in urban areas. The ASHA (Accredited Social Health Activist) network under the National Health Mission can play a role in monitoring elderly community members in rural areas.
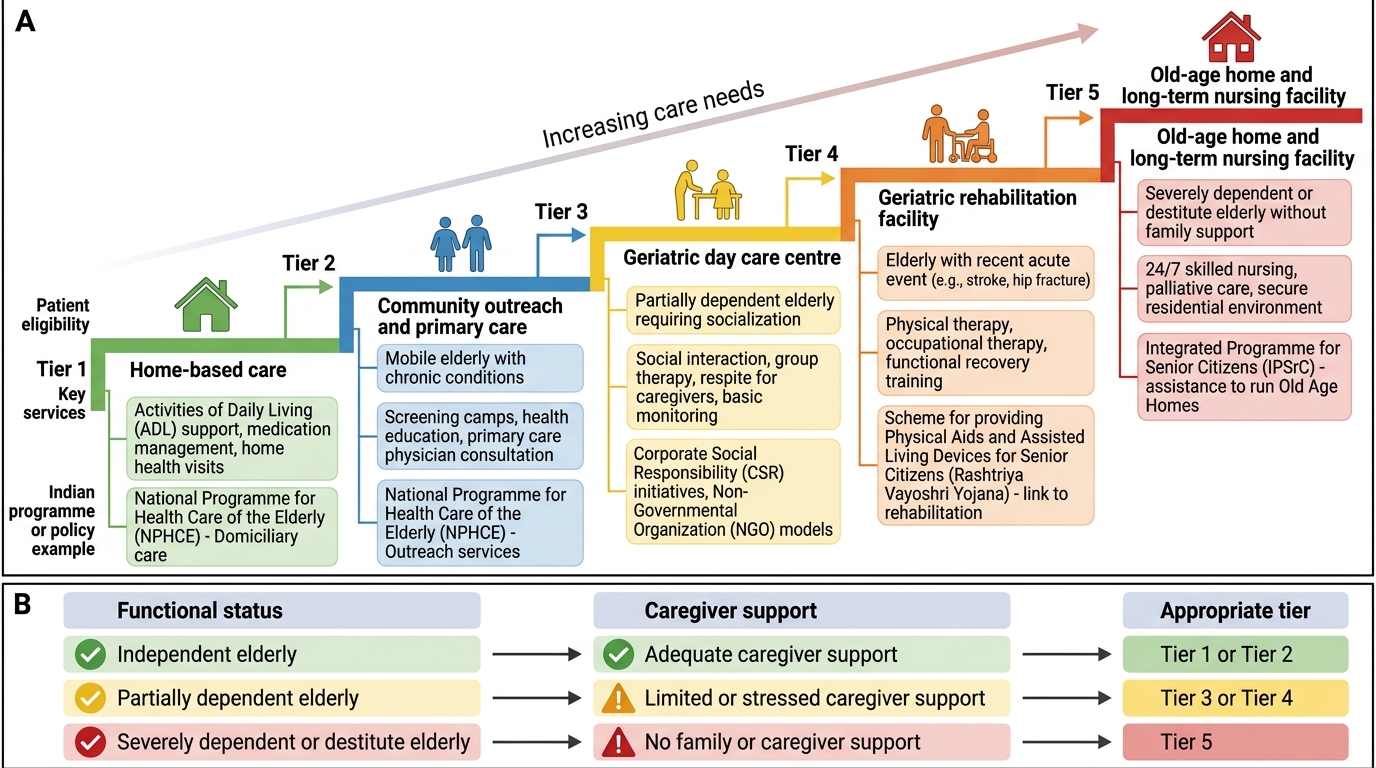
Tiered Care Continuum for Elderly Care in India
Day care and rehabilitation centres occupy the intermediate tier. Geriatric day care centres provide structured daytime programming — medical monitoring, physiotherapy, occupational therapy, social activities, and meals — while allowing the patient to return home in the evening, relieving caregiver burden. Geriatric rehabilitation facilities (inpatient or outpatient) provide structured multidisciplinary rehabilitation after hospitalisation for stroke, hip fracture, or major surgery. Day programmes reduce social isolation, delay institutionalisation, and improve functional outcomes.
Old age homes and long-term care facilities constitute the highest tier of residential care. In India, these are categorised as: (a) free homes for destitute elderly run by government or charitable organisations; (b) subsidised homes for low-income elderly with partial government support; and (c) private residential facilities for those who can afford to pay. The National Policy for Older Persons (NPOP) 1999 (revised 2011) outlines government responsibilities including financial security, health care, and residential facilities for the elderly. The Maintenance and Welfare of Parents and Senior Citizens Act, 2007 creates a legal obligation on children and heirs to maintain elderly parents, with provisions for maintenance tribunals that can order up to ₹10,000/month in maintenance payments. It also empowers authorities to set up old-age homes in every district for BPL elderly. The Pradhan Mantri Vaya Vandana Yojana (PMVVY) provides pension security, and Indira Gandhi National Old Age Pension Scheme (IGNOAPS) provides monthly pension to BPL elderly aged 60 and above (₹200/month for 60–79 years, ₹500/month for ≥80 years). The Geriatric Care Division under the Ministry of Health and Family Welfare coordinates health-related provisions. HelpAge India and ARDSI (Alzheimer's and Related Disorders Society of India) are key voluntary sector organisations. The clinician should be familiar enough with this ecosystem to make appropriate referrals rather than leaving patients and families to navigate it unaided.
SELF-CHECK
A 70-year-old widow living alone in a rural area is found to be malnourished with multiple unexplained bruises. Her son visits infrequently and controls her pension account. Which form of elder abuse is MOST likely occurring?
A. Physical abuse only
B. Psychological abuse only
C. Financial and physical abuse
D. Neglect only
Reveal Answer
Answer: C. Financial and physical abuse
The clinical picture suggests multiple concurrent forms of abuse. The unexplained bruises suggest physical abuse. The son controlling the pension account is a classic pattern of financial abuse — one of the most common forms of elder abuse in India. Neglect may also be present given the malnourishment. Elder abuse frequently involves multiple concurrent forms occurring within a single relationship of trust. Identifying all forms matters because the legal and intervention pathways differ: financial abuse is addressed by the Maintenance and Welfare of Parents and Senior Citizens Act 2007 and civil authorities; physical abuse may require police involvement.
Ethical Issues in Elderly Care: Autonomy, Capacity, and End-of-Life Decisions
Ethical reasoning in geriatric practice requires fluency with the four principles of biomedical ethics and their application to the specific challenges that arise when caring for older adults. The key ethical dilemmas in geriatric medicine cluster around three themes: respecting autonomy when capacity is uncertain, balancing beneficence against non-maleficence in aggressive versus palliative care, and distributing limited resources fairly in a context of multiple competing needs. Mastering the procedure of ethical reasoning in these contexts is the core clinical skill this section aims to develop.
Mental capacity and informed consent are the foundation of all ethical decision-making in medicine. Capacity is defined as the ability to (1) understand information relevant to a decision, (2) retain that information, (3) use and weigh that information to arrive at a decision, and (4) communicate that decision. Crucially, capacity is decision-specific and time-specific — a patient may lack capacity for a complex decision about cardiac surgery but retain capacity to decide about a diet or discharge destination. Capacity is also presumed present unless demonstrated otherwise — this is the legal default in Indian jurisprudence and internationally. The assessment of capacity uses structured bedside tools such as the MacArthur Competence Assessment Tool for Treatment (MacCAT-T): ask the patient to paraphrase what you have explained (understanding), to recall it 5 minutes later (retention), to weigh up pros and cons (reasoning), and to express a stable choice (communication). Capacity assessment is a clinical skill, not a legal determination — the physician makes the assessment; a court makes the legal determination only when disputed.
When a patient is found to lack capacity, the legal framework for proxy decision-making in India is less well-developed than in Western jurisdictions. Advance directives (also called living wills) — documents signed by a person with capacity specifying their treatment preferences in advance of loss of capacity — are legally recognised in India following the Supreme Court judgment in Common Cause v. Union of India (2018), which upheld the right to die with dignity and the right to refuse treatment through a living will. The Supreme Court specified a mechanism for executing and implementing advance directives, including registration with the local Collector's office and a requirement for a Medical Board to assess capacity when the advance directive is invoked. In practice, very few patients in India currently have advance directives, and the clinical discussion about goals of care (what the patient would want) must therefore rely on family history-taking and careful clinical judgment.
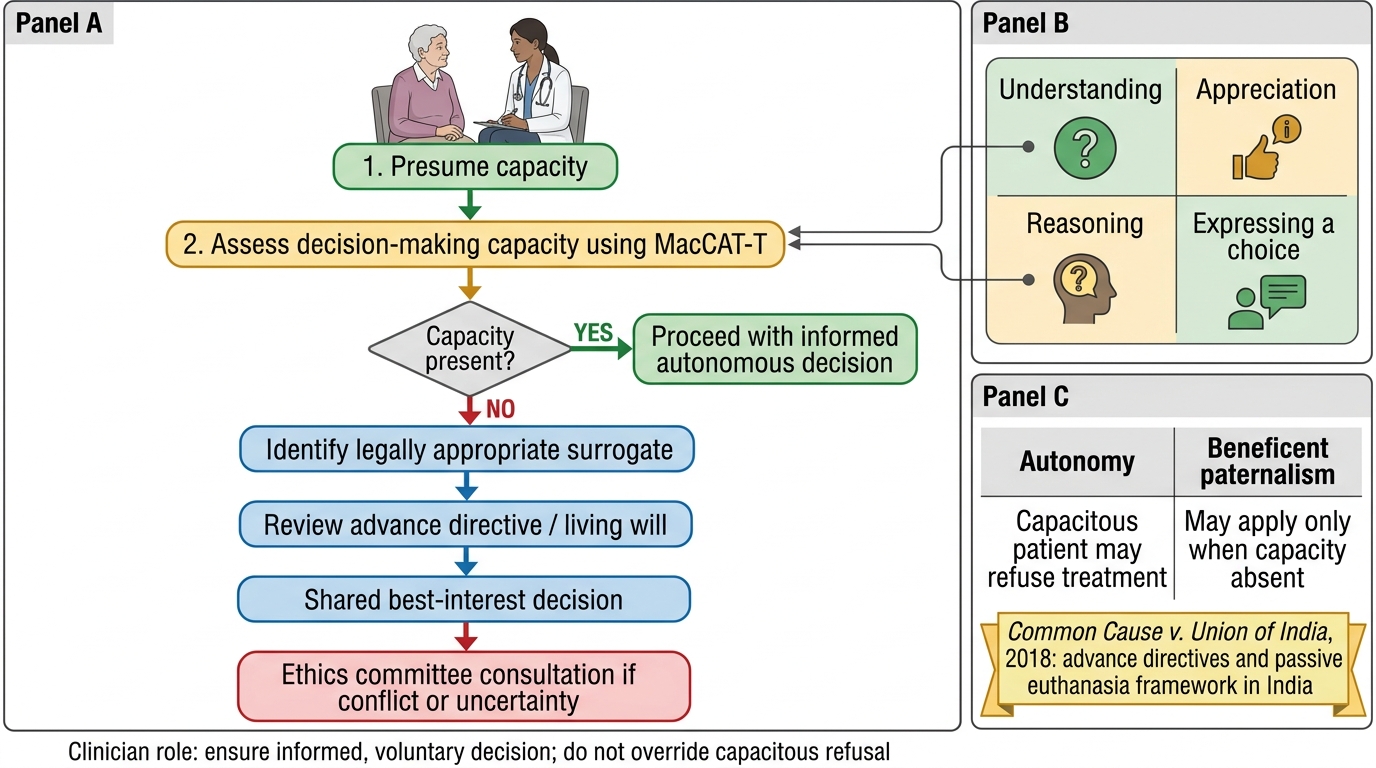
Ethical Decision-Making When Capacity Is in Doubt
Paternalism versus autonomy is a recurring tension. Beneficent paternalism — overriding a patient's expressed preference in what the clinician judges to be the patient's best interest — may be appropriate when a patient lacks capacity. But for capacitous patients, autonomy takes precedence over beneficence: a patient who understands the risks and implications of refusing treatment has the right to refuse, even if their clinician disagrees. This principle is especially important in geriatric care, where patients frequently refuse hospitalisation, surgery, or aggressive treatment — and where their refusal may reflect genuine, considered preferences rather than cognitive impairment or depression. The clinician's role is to ensure the decision is informed and voluntary, not to override it.
Polypharmacy and harm prevention raise non-maleficence issues. Prescribing a medication that is appropriate for a 50-year-old may be actively harmful in an 80-year-old with multiple comorbidities, impaired renal function, and altered pharmacokinetics. The Beers Criteria and STOPP-START criteria (addressed in the geriatric foundations SDL) are ethical tools as much as clinical ones — using them is part of the duty of non-maleficence. Failure to review and rationalise a polypharmacy list is an ethical failure as well as a clinical one.
Resource allocation and justice become acute when, for example, ICU beds are limited, or when expensive investigation or treatment is ordered for an elderly patient whose benefit is marginal. The principle of justice requires that decisions not be made on the basis of age alone — ageism in medicine (withholding care on the basis of age rather than clinical indicators of benefit) is ethically impermissible. Prognostic tools such as the Clinical Frailty Scale and performance-status measures are appropriate guides for resource allocation; chronological age alone is not. The issue of futile treatment — continuing aggressive interventions beyond the point where they offer meaningful benefit, often at the insistence of families — is a common ethical challenge. Clinicians must be able to initiate and facilitate a goals-of-care conversation that clarifies what the patient would want, what is medically appropriate, and what the family understands.
SELF-CHECK
An 82-year-old with moderate dementia is brought to hospital in a hypertensive emergency. His daughter insists on aggressive intervention including ICU admission. The patient has no advance directive but had previously told his GP he did not want 'machines'. The doctor assesses that the patient currently lacks capacity to make this specific decision. What is the MOST appropriate next step?
A. Proceed with full aggressive treatment as demanded by the daughter
B. Refuse all treatment because the patient previously expressed a wish not to be on machines
C. Treat the acute hypertensive emergency, then hold a structured goals-of-care conversation with the family using the patient's known values as a guide
D. Refer immediately to the court for a legal determination
Reveal Answer
Answer: C. Treat the acute hypertensive emergency, then hold a structured goals-of-care conversation with the family using the patient's known values as a guide
The immediate life-threatening emergency must be treated — withholding acute treatment entirely without a properly documented advance directive refusing it would breach beneficence and possibly endanger life. However, once the acute crisis is stabilised, a proper goals-of-care discussion must occur. The patient's previously expressed preference ('no machines') is important evidence of his values and should inform — but not legally bind — the surrogate decision-making process. Full ICU without any consideration of the patient's known values is inappropriately paternalistic. Routine cases do not require immediate court referral — courts are reserved for disputed cases where the clinical team and family cannot reach consensus.