Page 8 of 32
IM25.{4,9} | Geriatric Vascular Events and Stroke — SDL Guide (Part 2)
Secondary Prevention, Long-Term Management and Rehabilitation
Stroke secondary prevention is the arena where knowledge of stroke mechanism directly determines treatment, and where getting it wrong causes recurrent stroke. The key principle: antiplatelet therapy prevents recurrent thromboembolism from atherothrombotic and lacunar stroke; anticoagulation prevents recurrent cardioembolic stroke; both together cause excess bleeding without added benefit.
Provided image
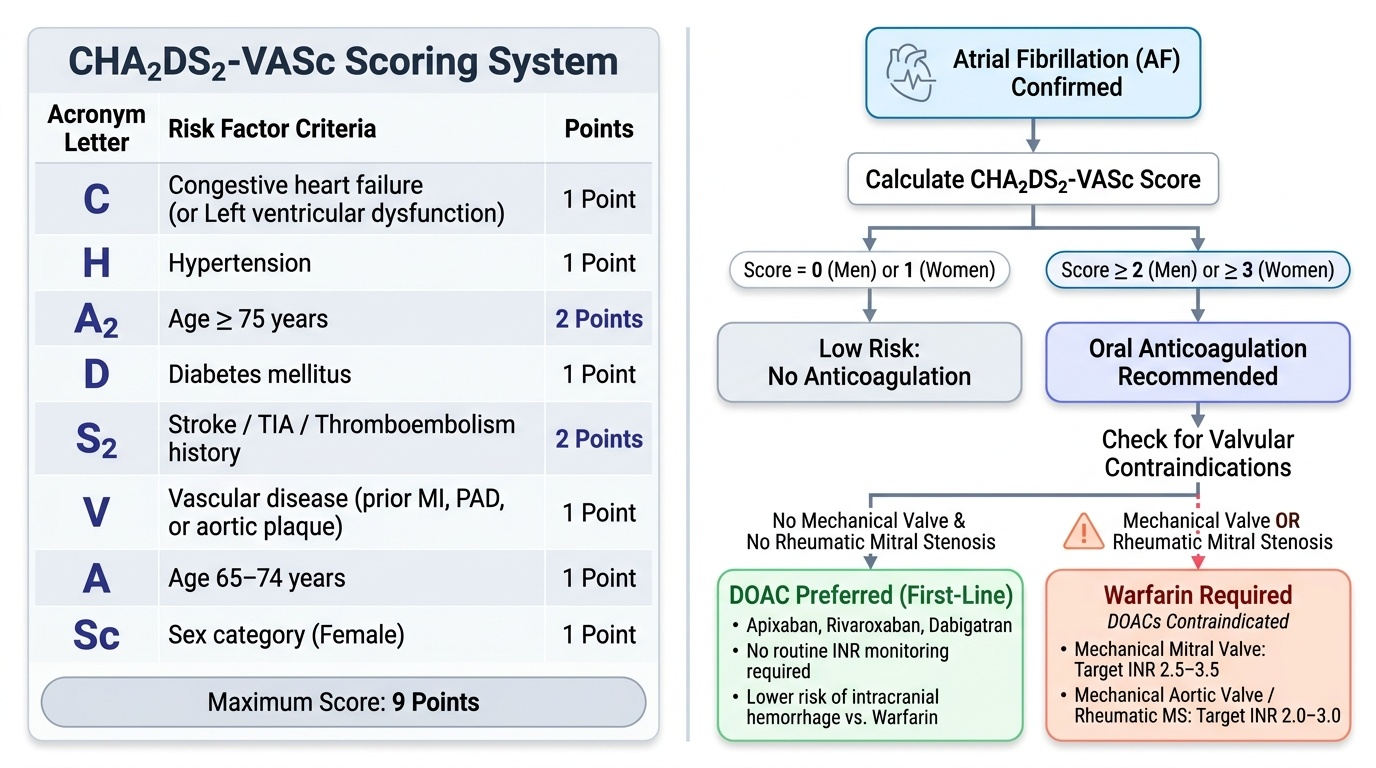
Atrial fibrillation and anticoagulation: AF is the most important modifiable risk factor for cardioembolic stroke in the elderly. The CHA₂DS₂-VASc score quantifies annual stroke risk and guides anticoagulation decisions: Congestive heart failure (1) + Hypertension (1) + Age ≥75 years (A₂, 2 points) + Diabetes (1) + Stroke/TIA history (S₂, 2 points) + Vascular disease (1) + Age 65–74 (1) + Sex category female (1). Maximum 9 points. Guidelines recommend oral anticoagulation for: men with score ≥2, women with score ≥3. In older patients with AF and prior stroke, the CHA₂DS₂-VASc score is typically ≥4–6, making anticoagulation clearly indicated. Direct oral anticoagulants (DOACs) — apixaban, rivaroxaban, dabigatran — are preferred over warfarin in non-valvular AF in the elderly: equal or superior efficacy, significantly lower rates of intracranial haemorrhage, no routine INR monitoring required. The exception: mechanical heart valve prostheses require warfarin (DOACs are contraindicated; target INR 2.5–3.5 for mechanical mitral valve, 2–3 for mechanical aortic valve). Rheumatic mitral stenosis with AF also requires warfarin. The HAS-BLED score quantifies bleeding risk and should be calculated alongside CHA₂DS₂-VASc — a high HAS-BLED score prompts addressing modifiable bleeding risk factors (labile INR, uncontrolled hypertension, concomitant NSAID/aspirin use) rather than withholding anticoagulation.
Antiplatelet therapy for non-cardioembolic stroke: Aspirin 150–300 mg loading dose within 24–48 hours of ischaemic stroke (after haemorrhage excluded), then aspirin 75–100 mg daily long-term. The combination of aspirin + clopidogrel (dual antiplatelet therapy, DAPT) for 21 days is recommended after minor ischaemic stroke or high-risk TIA (ABCD² ≥4) — based on CHANCE and POINT trial evidence reducing 90-day stroke risk. Long-term DAPT beyond 3 months does not provide additional stroke prevention benefit and increases bleeding risk. Statins: High-intensity statin therapy (atorvastatin 40–80 mg/day) is recommended for all ischaemic stroke patients regardless of baseline LDL-C (the SPARCL trial demonstrated a 16% relative risk reduction in recurrent stroke with atorvastatin). In the very elderly (>80 years), statin initiation requires weighing benefit against polypharmacy burden and patient preference.
Carotid endarterectomy (CEA) and stenting: For symptomatic carotid stenosis ≥70% (ipsilateral to the stroke or TIA), CEA within 2 weeks of the index event reduces 5-year stroke risk by approximately 50% (NNT=6 for 70–99% stenosis, from NASCET/ECST trials). Age alone should not preclude CEA — elderly patients have equivalent relative risk reduction. The absolute benefit is greatest in the first two weeks.
Stroke rehabilitation: Recovery after stroke begins in the acute phase and continues in the community for months to years. The principles of neuroplasticity-based rehabilitation: early mobilisation (within 24–48 hours of stable ischaemic stroke), high intensity of task-specific practice, and multidisciplinary team approach. Components: physiotherapy for motor recovery (hemiparesis, gait, balance — using constraint-induced movement therapy, treadmill training); speech and language therapy for aphasia and dysphagia (nasogastric tube feeding for severe dysphagia — early feeding reduces complications; percutaneous endoscopic gastrostomy (PEG) for long-term dysphagia); occupational therapy for ADL retraining and assistive device assessment; neuropsychology for cognitive rehabilitation and depression management (post-stroke depression occurs in 30–40% of stroke survivors and requires active treatment with SSRI — most evidence for fluoxetine, citalopram); bladder and bowel management for incontinence; anticoagulation management for AF patients.
Specific geriatric rehabilitation considerations: falls risk is very high post-stroke (hemiparesis, visuospatial neglect, spasticity, medications); spasticity management (physiotherapy, oral baclofen, botulinum toxin injections for focal spasticity); communication barriers (aphasia — requires augmentative and alternative communication strategies); driving reassessment (mandatory for any patient with new focal neurological deficit); caregiver burden (as with dementia, stroke caregiving is intensely demanding — carer support and respite must be part of the discharge plan).
SELF-CHECK
A 76-year-old woman with atrial fibrillation, hypertension, type 2 diabetes, and a TIA six months ago (now resolved) presents for review. She is currently on aspirin 75 mg daily — her cardiologist started anticoagulation 'on hold' pending further assessment. Her CHA₂DS₂-VASc score is calculated. Which treatment decision is most appropriate?
A. Continue aspirin 75 mg alone — sufficient for TIA secondary prevention in AF
B. Start dual antiplatelet therapy with aspirin plus clopidogrel for secondary prevention of cardioembolic stroke
C. Start oral anticoagulation (DOAC preferred for non-valvular AF) — her CHA₂DS₂-VASc score indicates high stroke risk clearly mandating anticoagulation
D. Start warfarin — DOACs are contraindicated in patients over 75
Reveal Answer
Answer: C. Start oral anticoagulation (DOAC preferred for non-valvular AF) — her CHA₂DS₂-VASc score indicates high stroke risk clearly mandating anticoagulation
CHA₂DS₂-VASc calculation: Hypertension (1) + Age ≥75 (A₂, 2) + Diabetes (1) + Stroke/TIA (S₂, 2) = 6 points. This represents very high stroke risk — annual stroke rate approximately 9.8% without anticoagulation. Oral anticoagulation is strongly indicated. DOAC (apixaban or rivaroxaban preferred) is preferred over warfarin in non-valvular AF at any age — DOACs have equivalent or superior stroke prevention with significantly lower intracranial haemorrhage rates compared to warfarin; age >75 is not a contraindication to DOACs. Antiplatelet therapy alone is markedly inferior to anticoagulation for cardioembolic stroke prevention and should not be used as a substitute when anticoagulation is indicated.
Self-Assessment: Vascular Events in the Elderly
The following clinical scenarios integrate the full arc from presentation through to secondary prevention, testing the NMC KH-level requirement to apply clinical reasoning across the full stroke management continuum. Work through each scenario before reading the analysis.
Scenario A: Mr Rajendran, 79 years old with hypertension and type 2 diabetes, is brought to the emergency department with right-sided weakness and slurred speech that started 3 hours ago. BP 192/108 mmHg. CT brain shows no haemorrhage. NIHSS score 12. There is no large vessel occlusion on CTA. He takes metformin and amlodipine. His daughter reports he is independent and lives at home. Should he receive IV thrombolysis, and what BP management is required?
Analysis: He is within the 4.5-hour window; no haemorrhage on CT; no obvious contraindications. IV alteplase is indicated. Pre-thrombolysis BP management: reduce BP to <185/110 mmHg before administration (use IV labetalol or nicardipine — avoid nitroprusside in acute stroke). Post-thrombolysis: maintain BP <180/105 mmHg for 24 hours. His metformin and amlodipine should be continued. At 79, age alone is not a contraindication to thrombolysis — functional independence and absence of major contraindications guide the decision.
Scenario B: Mrs Devi, 72 years old with known atrial fibrillation (not anticoagulated, 'to be reviewed'), presents 30 minutes after sudden onset of complete left-sided weakness, dense neglect of the left side, and inability to understand speech (global aphasia). BP 168/96 mmHg. NCCT shows no haemorrhage. CTA shows complete right MCA occlusion. INR 1.1 (no anticoagulant). What is the treatment sequence and what definitive secondary prevention is required?
Analysis: Reperfusion strategy: IV alteplase (within 4.5 hours), followed immediately (or in parallel if door-to-needle time >60 min) by mechanical thrombectomy for the large vessel occlusion — this is the most effective combination for MCA-LVO. Secondary prevention: she has atrial fibrillation with prior stroke — CHA₂DS₂-VASc ≥4 — start DOAC (apixaban 5 mg twice daily or rivaroxaban 20 mg once daily) after 2 weeks (to allow haemorrhagic transformation risk to stabilise after large cardioembolic infarct — timing of anticoagulation initiation after stroke is based on the HAEST/EAFT guidelines: minor stroke/TIA = start early at 1–3 days; moderate stroke = 6–8 days; large infarct = 2–4 weeks).
Scenario C: Mr Balasubramaniam, 82 years old, experienced a 15-minute episode of right hand numbness and weakness (fully resolved) three days ago. He did not seek attention, attributing it to 'old age.' His GP now sends him to the outpatient with a note: 'possible TIA.' ABCD² score: Age ≥60 (1) + BP 158/94 (1) + unilateral weakness (2) + 10–59 minutes (1) + no diabetes (0) = 5 (moderate-to-high risk). What is the management priority and which secondary prevention should be initiated immediately?
Analysis: Moderate-to-high risk TIA (ABCD² 5) — risk of stroke within 2 days is approximately 4%; within 90 days is 10–15%. Immediate management: MRI brain (DWI to identify if small infarct already occurred, upgrading this to stroke); carotid Doppler/CTA (exclude symptomatic carotid stenosis ≥70%); cardiac monitoring (24–48 hour Holter for paroxysmal AF). Start aspirin 300 mg immediately (then 75 mg/day), and if no AF on cardiac monitoring, add clopidogrel (DAPT for 21 days). If carotid stenosis ≥70% found — refer for CEA within 2 weeks. If paroxysmal AF found — start DOAC. The 72-hour delay in seeking care is a teachable moment: public education about TIA as a 'warning stroke' requiring emergency evaluation can prevent completed stroke.
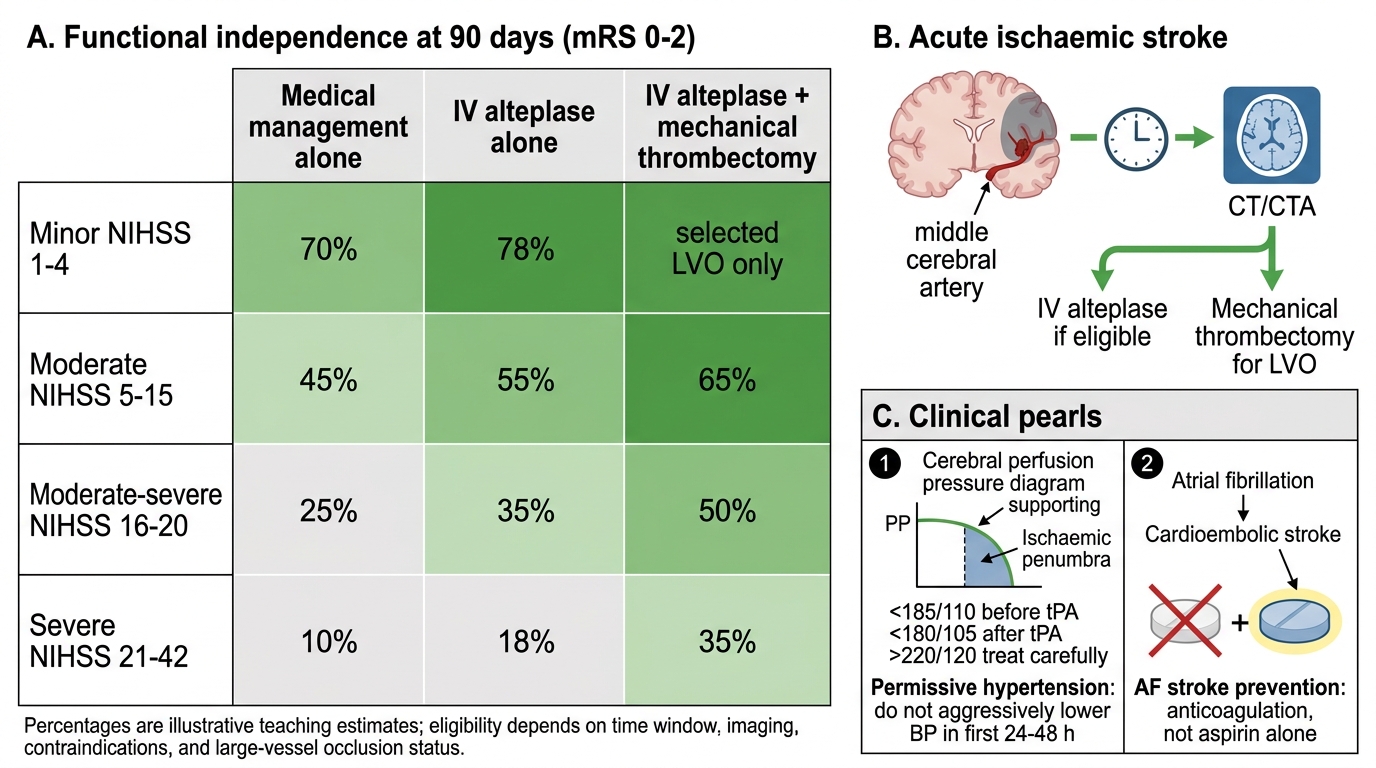
Ischaemic Stroke Outcomes by NIHSS Severity
CLINICAL PEARL
The two most important clinical rules in acute stroke management that are frequently violated: (1) Do NOT aggressively lower blood pressure in the first 24–48 hours of ischaemic stroke — permissive hypertension up to 220/120 mmHg is the guideline. The reflex to 'treat the high BP' is dangerous; the ischaemic penumbra is perfusion-pressure dependent, and aggressive BP reduction extends the infarct. Antihypertensive therapy is only indicated pre-thrombolysis (target <185/110 before tPA), post-tPA (target <180/105), or if BP >220/120 mmHg. (2) Atrial fibrillation causing cardioembolic stroke requires anticoagulation, not antiplatelet therapy. Aspirin is standard care after atherothrombotic or lacunar stroke. In AF-related stroke, aspirin offers only a fraction of the protection of anticoagulation and should not substitute for it when anticoagulation is indicated. A patient who has a cardioembolic stroke on aspirin was undertreated from the start.