Page 9 of 35
IM26.12-13 | Central Nervous System and Clostridial Infections — SDL Guide
Learning Objectives
- Describe the common causes, clinical features, and management of bacterial and viral meningitis with emphasis on CSF profile interpretation
- Describe the common causes, clinical features, and management of encephalitis including herpes simplex encephalitis
- Describe the aetiology, pathogenesis, clinical features, and management of tetanus including the role of tetanospasmin
- Describe the aetiology, pathogenesis, clinical features, and management of botulism distinguishing it from tetanus
- Describe the aetiology, pathogenesis, clinical features, and management of gas gangrene (clostridial myonecrosis)
INSTRUCTIONS
This SDL covers two groups of life-threatening infections that share a common theme: the consequences of toxins acting on the nervous system. CNS infections (meningitis and encephalitis) demand rapid diagnosis using CSF analysis and immediate empirical treatment. Clostridial infections (tetanus, botulism, gas gangrene) are toxin-mediated diseases where understanding the molecular mechanism of the toxin predicts the clinical syndrome.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 133 — Meningitis, Encephalitis; Ch. 129 — Tetanus, Botulism, Gas Gangrene (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 13 — Infectious Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old student is brought to the emergency department at midnight with severe headache, photophobia, and neck stiffness that developed over 6 hours. His temperature is 39.8°C and he has a non-blanching petechial rash on his trunk and lower limbs. In the adjacent bay, a 45-year-old farm labourer who sustained a deep puncture wound to his foot three days ago now presents with jaw stiffness making it impossible to open his mouth, with progressive muscle spasms in his neck and back — every external stimulus (a door closing, bright light) triggers a violent whole-body convulsion. These two patients illustrate the range of nervous system infections: the student has meningococcal meningitis, where minutes without antibiotics mean irreversible brain injury or death; the farm worker has tetanus, where the toxin is already fixed to spinal cord synapses and the treatment is now about controlling the consequences rather than eliminating the pathogen. Both require ICU-level care, but the mechanism of injury, the diagnostic approach, and the management are entirely different. This module prepares you to recognise and manage both.
WHY THIS MATTERS
CNS infections are among the true emergencies of internal medicine: delay in diagnosis and treatment of bacterial meningitis measurably increases mortality and neurological sequelae — every hour without antibiotics matters. Encephalitis, particularly herpes simplex encephalitis (HSE), has a mortality of 70% untreated and requires empirical aciclovir before CSF PCR results return. Tetanus remains a significant cause of morbidity and mortality in India — particularly in newborns (neonatal tetanus from contaminated cord stumps) and in unimmunised adults with contaminated wounds. These infections collectively test the physician's ability to recognise neurological emergencies, interpret CSF results accurately, and initiate the correct empirical treatment without waiting for all diagnostic certainty to arrive.
RECALL
Before proceeding, recall the relevant anatomy and microbiology. The blood-brain barrier (BBB) protects the CNS from pathogens but also limits antibiotic penetration — only lipid-soluble antibiotics and certain beta-lactams (ceftriaxone, penicillin at high doses) achieve adequate CSF concentrations. The meninges — dura mater, arachnoid mater, and pia mater — enclose the subarachnoid space through which CSF circulates; meningitis = inflammation of the meninges. The brain parenchyma itself is the target in encephalitis. From neurology: recall the signs of meningism — Kernig's sign (resistance and pain on extension of the knee with the hip flexed to 90°) and Brudzinski's sign (involuntary hip/knee flexion when the neck is passively flexed). Tetanospasmin is a zinc-metalloprotease; botulinum toxin cleaves SNARE proteins — both act at synapses, but in opposite directions: tetanus produces spastic/convulsive paralysis, botulism produces flaccid paralysis.
Clinical Presentation of CNS Infections: Meningitis and Encephalitis
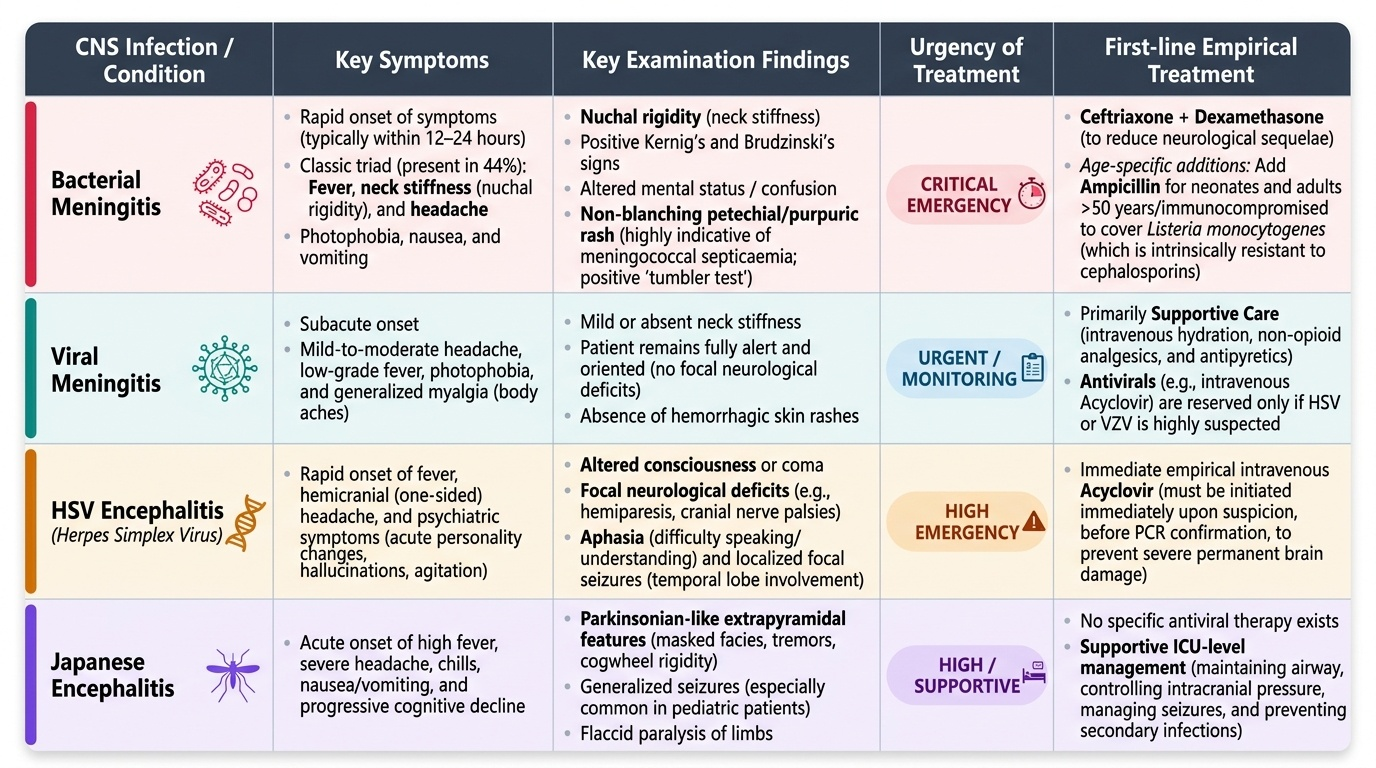
Bacterial meningitis is a medical emergency defined by bacterial infection of the meninges and subarachnoid space, producing intense inflammatory exudate in the CSF. It is the most dangerous form of meningitis — carrying an untreated mortality of close to 100% and a treated mortality of 15–30% — and neurological sequelae (hearing loss, cognitive impairment, focal deficits) occur in 10–20% of survivors even with optimal treatment. The speed of clinical progression is its most dangerous feature: the disease can evolve from mild headache to unconsciousness within 12–24 hours, and to death within 24–48 hours of onset.
Provided image
The classic clinical triad of bacterial meningitis is: fever + neck stiffness (nuchal rigidity) + headache. All three are present in only 44% of adult patients — so the absence of one component does not exclude the diagnosis. The most sensitive individual symptom is headache (present in ~87% of adult bacterial meningitis cases); the most specific sign combination is fever + neck stiffness + altered consciousness. The non-blanching petechial/purpuric rash of meningococcal disease is the most important dermatological sign in medicine — it indicates septicaemia and demands immediate antibiotic administration before any further diagnostic step. The rash begins as a few petechiae and rapidly progresses to coalescent purpura and ecchymoses. The 'tumbler test' — pressing a glass against the skin — confirms non-blanching.
The causative organisms vary by age, and age is the most powerful single predictor of the causative bacterium:
| Age group | Dominant organisms | Key empirical note |
|---|---|---|
| Neonates (0–28 days) | Streptococcus agalactiae (GBS), E. coli K1, Listeria monocytogenes | Ampicillin + cefotaxime |
| Infants (1–23 months) | S. pneumoniae, N. meningitidis, H. influenzae type b | Ceftriaxone + dexamethasone |
| Young adults (16–50 years) | N. meningitidis, S. pneumoniae | Ceftriaxone + dexamethasone |
| Adults >50 years / immunocompromised | S. pneumoniae, Listeria monocytogenes | Ceftriaxone + ampicillin (Listeria) + dexamethasone |
Listeria monocytogenes deserves special emphasis: it is intrinsically resistant to ALL cephalosporins (including ceftriaxone). The clinical clue is an older patient (>50 years), immunocompromised, pregnant, or diabetic with purulent meningitis — ampicillin must always be added in these cases.
Encephalitis is inflammation of the brain parenchyma — distinct from meningitis (meninges) or meningoencephalitis (both). It presents with altered consciousness, behavioural changes, and focal neurological deficits, often with fever and headache. The most important form is herpes simplex encephalitis (HSE), caused predominantly by HSV-1. Its characteristic tropism for the temporal lobes produces: psychiatric symptoms (personality change, confusion), temporal lobe seizures (olfactory/gustatory hallucinations, lip-smacking automatisms), aphasia, and memory impairment. MRI brain (FLAIR) shows hyperintense signal in the temporal lobes — often asymmetric. CSF HSV PCR is the confirmatory test (sensitivity >95%). Critical principle: aciclovir 10 mg/kg IV 8-hourly must be started empirically as soon as HSE is suspected — mortality is 70% untreated vs ~25% with aciclovir. Never await MRI or PCR results before starting aciclovir.
Japanese encephalitis (JE) is caused by Japanese encephalitis virus, a flavivirus transmitted by Culex mosquitoes breeding in rice paddies — prevalent in agricultural Northeast and Southern India during monsoon. Clinical features: fever, parkinsonian features (rigidity, tremor), seizures, mask-like facies. MRI shows bilateral thalamic T2 hyperintensity — a characteristic pattern. Diagnosis: serum and CSF anti-JEV IgM ELISA. No specific antiviral; management is supportive. Prevention: JE vaccine is included in the National Immunisation Schedule for high-endemic states.
Pathogenesis of CNS Infections and Clostridial Toxin Mechanisms
Understanding the pathogenesis of CNS infections and clostridial toxin mechanisms is not merely academic — it explains the specific clinical syndromes, predicts complications, and rationalises every treatment choice. The two groups covered in this SDL cause disease through fundamentally different mechanisms: CNS infections cause disease through the host's own inflammatory response to the pathogen within the protected CNS compartment, while clostridial infections cause disease through exotoxins that act directly on nerve synapses.
Pathogenesis of bacterial meningitis: Bacteria enter the subarachnoid space via haematogenous seeding (most common), direct spread from adjacent structures (otitis media, sinusitis, mastoiditis), or post-neurosurgical/traumatic introduction. Once in the CSF — which is relatively immunodeficient compared to blood (low immunoglobulin, low complement) — bacteria multiply rapidly. The release of bacterial cell wall components (LPS from Gram-negatives; peptidoglycan and teichoic acid from Gram-positives) triggers meningeal and choroid plexus cells to release pro-inflammatory cytokines (IL-1β, TNF-α, IL-6), chemokines, and prostaglandins. This inflammatory cascade is the primary mediator of injury — not the bacteria directly — producing: (a) cerebral oedema (vasogenic from BBB disruption, cytotoxic from neuronal injury, and interstitial from hydrocephalus), (b) cerebral vasculitis and thrombosis → infarction, (c) raised intracranial pressure → herniation, and (d) sensorineural hearing loss (inflammatory damage to the cochlear nerve). This is why dexamethasone — by suppressing the cytokine response — reduces mortality and hearing loss even though it does not kill bacteria directly.
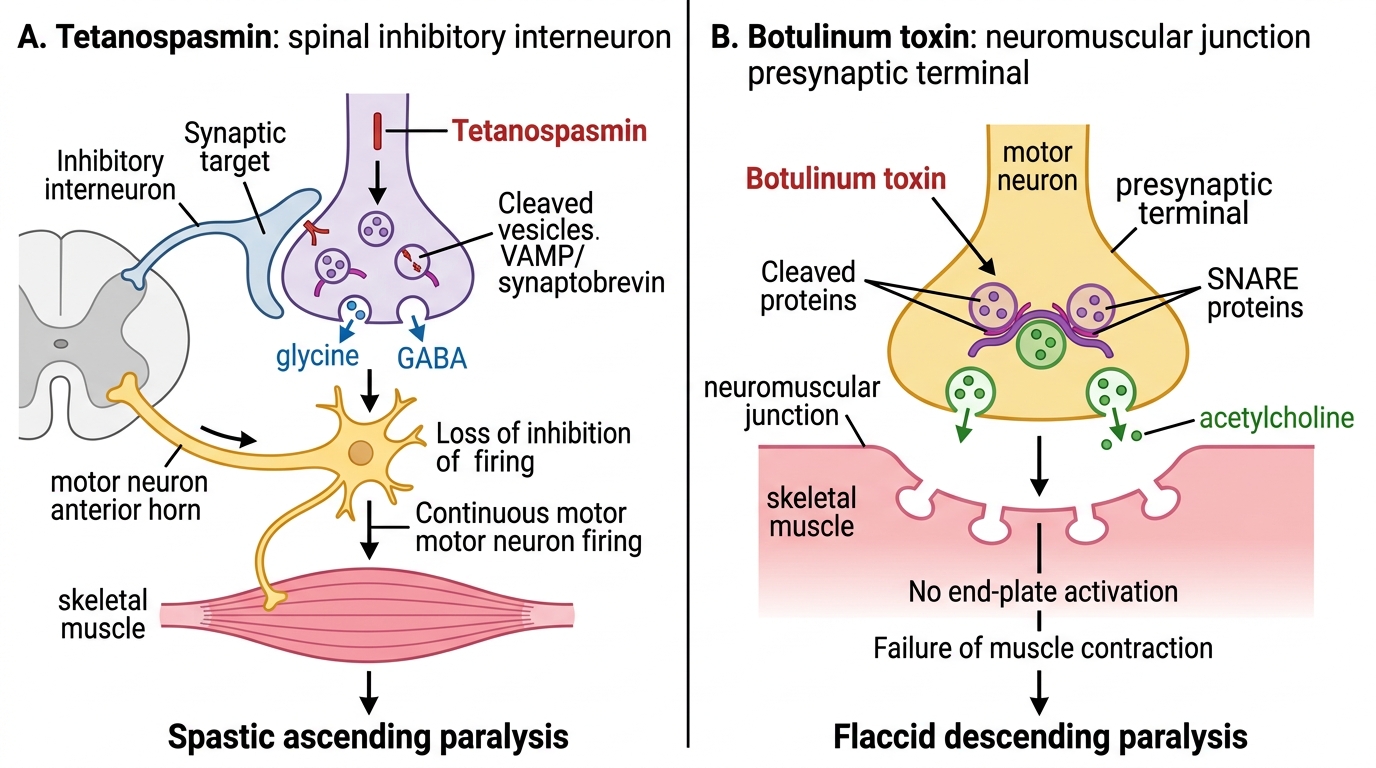
Tetanospasmin mechanism — the molecular basis of tetanus: Clostridium tetani spores contaminate a wound. In the anaerobic environment of devitalised tissue, spores germinate into vegetative organisms producing tetanospasmin. The toxin binds to ganglioside receptors at peripheral nerve terminals, undergoes retrograde axonal transport to the spinal cord and brainstem interneurons, then transcytoses to the presynaptic terminals of glycinergic and GABAergic inhibitory interneurons. Tetanospasmin is a zinc-metalloprotease that cleaves synaptobrevin (VAMP) — the SNARE protein required for vesicle fusion with the presynaptic membrane. Without vesicle fusion, inhibitory neurotransmitters (glycine and GABA) cannot be released. The result: motor neurons fire continuously and uncontrollably in response to any stimulus → ascending spastic paralysis, rigid muscles, and reflex convulsive spasms (tetanic spasms).
The crucial therapeutic implication: once tetanospasmin is bound to neural tissue, it cannot be displaced by antitoxin (HTIG). HTIG only neutralises unbound toxin still circulating in the bloodstream. This is why HTIG must be given as early as possible (to prevent additional toxin from binding) and why established tetanus must be managed by controlling the consequences (muscle relaxation, airway) rather than the cause.
Botulinum toxin mechanism — the molecular basis of botulism: Clostridium botulinum toxin also acts on synaptic vesicle release machinery, but at a different anatomical site and with the opposite clinical effect. Botulinum toxin cleaves SNARE proteins (SNAP-25 and syntaxin for types A and C; VAMP for types B, D, F, G) at the presynaptic cholinergic terminals of the neuromuscular junction — preventing acetylcholine release. Without ACh release: (a) voluntary muscles cannot contract → descending flaccid paralysis (cranial nerve NMJs, with their shortest axons, are affected first); (b) autonomic cholinergic synapses are also blocked → dry mouth, constipation, urinary retention, blurred vision from ciliary muscle paralysis; (c) consciousness is preserved (toxin does not cross the BBB); (d) no fever (no tissue invasion).
Tetanus vs Botulism: Toxin Mechanisms
CSF Analysis: Diagnosis of Meningitis and Encephalitis
Cerebrospinal fluid (CSF) analysis is the single most important investigation in suspected meningitis and encephalitis. The CSF profile distinguishes bacterial from viral, tubercular, and fungal meningitis with high specificity — and this distinction has direct, immediate therapeutic consequences that cannot be delayed. Before performing lumbar puncture (LP), assess for contraindications to LP: papilloedema, focal neurological signs, or depressed consciousness (GCS <10) raise the risk of cerebral herniation and mandate CT head first. However, CT is normal in 85% of bacterial meningitis cases and must not be used as a routine prerequisite that delays LP or antibiotic initiation. The guiding principle is: if LP is safe, perform it; if CT must precede LP, start antibiotics immediately and perform LP immediately after CT. The analytical yield of CSF is reduced but not eliminated by prior antibiotic doses — Gram stain and antigen tests may still be positive.
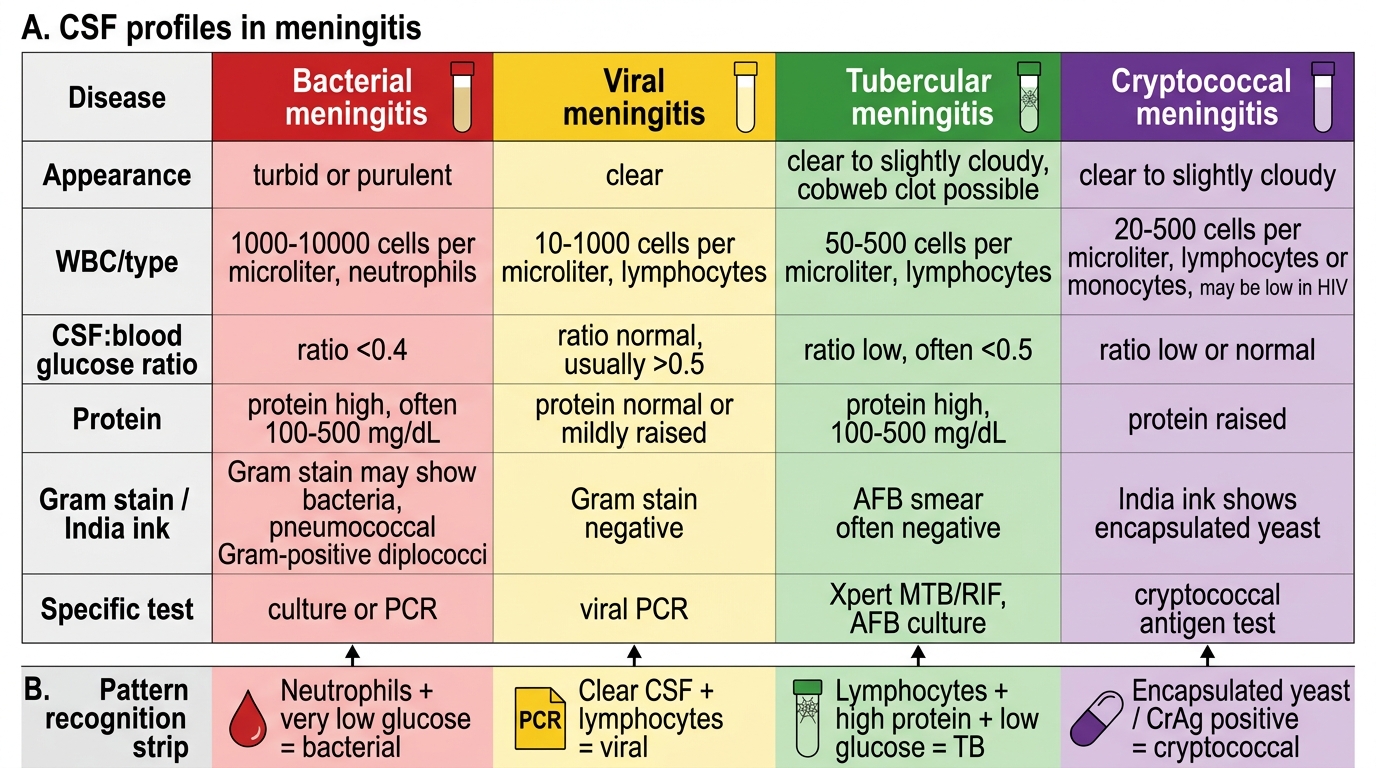
The four CSF parameters most discriminative for aetiology are: (1) appearance, (2) cell count and differential, (3) glucose (as the CSF:blood ratio), and (4) protein. The full CSF profile comparison:
| Feature | Normal | Bacterial | Viral | Tubercular | Cryptococcal |
|---|---|---|---|---|---|
| Appearance | Clear | Turbid/purulent | Clear/slightly turbid | Clear/slightly turbid | Clear |
| Opening pressure | 5–20 cm H₂O | Very high (>30) | Normal/mildly elevated | Elevated (20–40) | Elevated |
| WBC count | <5/µL | 1000–10,000/µL | 50–1000/µL | 10–500/µL | 20–500/µL |
| Cell type | Lymphocytes | PMNs (neutrophils) | Lymphocytes | Lymphocytes | Lymphocytes |
| Glucose | 50–80 mg/dL | Very low (<40 mg/dL; ratio <0.4) | Normal (ratio ≥0.6) | Low (<45 mg/dL; ratio <0.5) | Low |
| Protein | 15–45 mg/dL | Very high (100–500 mg/dL) | Mildly elevated (50–100 mg/dL) | Moderately elevated (100–500) | Moderately elevated |
| Gram stain | Negative | Positive in 60–90% (before Abx) | Negative | Negative | Negative |
| India ink | Negative | Negative | Negative | Negative | Positive (encapsulated yeasts) |
| Key specific test | — | Meningococcal/pneumococcal PCR | HSV/JEV PCR | GeneXpert CSF for MTB; AFB smear | CrAg latex agglutination |
Key interpretation pitfalls:
- Early viral meningitis may initially show PMN pleocytosis, mimicking bacterial meningitis — the glucose is normal in viral; repeat LP at 6–12 hours shows shift to lymphocyte predominance
- TB meningitis: glucose can be near-normal in very early disease; a cobweb clot in the CSF tube (high fibrin) is characteristic; always request AFB smear + GeneXpert CSF + LJ culture simultaneously
- Partially treated bacterial meningitis: PMNs shift toward lymphocytes; Gram stain may be negative but antigen tests (CIE, latex agglutination) or PCR may still be positive
- HSV encephalitis: CSF may contain red blood cells (haemorrhagic necrosis of temporal lobe) alongside lymphocytic pleocytosis — a useful diagnostic clue
- Normal CSF does NOT exclude very early bacterial meningitis (first 1–6 hours of illness)
CSF Profiles in Meningitis
SELF-CHECK
A 25-year-old student presents with 12 hours of fever (39.8°C), severe headache, and neck stiffness. CT head is normal. CSF shows: turbid, WBC 8,400/µL (90% neutrophils), glucose 28 mg/dL (blood glucose 92 mg/dL), protein 420 mg/dL, Gram stain: Gram-positive diplococci. Which is the MOST appropriate immediate treatment?
A. IV aciclovir 10 mg/kg 8-hourly — Gram-positive diplococci suggest herpes simplex encephalitis
B. IV ceftriaxone 2g 12-hourly + IV dexamethasone 0.15 mg/kg 6-hourly × 4 days
C. IV vancomycin alone — Gram-positive diplococci indicate MRSA meningitis
D. Oral amoxicillin 500 mg three times daily × 7 days — the patient is young and otherwise healthy
Reveal Answer
Answer: B. IV ceftriaxone 2g 12-hourly + IV dexamethasone 0.15 mg/kg 6-hourly × 4 days
This is classic bacterial meningitis — turbid CSF, >1000 WBC predominantly neutrophils, very low glucose ratio (28/92 = 0.30, below 0.4), very high protein, and Gram-positive diplococci in pairs = Streptococcus pneumoniae. IV ceftriaxone 2g 12-hourly is the first-line empirical treatment. IV dexamethasone 0.15 mg/kg 6-hourly × 4 days should be given with or before the first antibiotic dose — it reduces the inflammatory response and has been shown to reduce mortality and hearing loss in adults with pneumococcal meningitis (de Gans trial, NEJM 2002). Aciclovir is for herpes encephalitis, not purulent bacterial meningitis. Oral antibiotics are entirely inadequate.