Page 12 of 35
IM26.15-16 | Gram Negative Nonfermenter and Helicobacter Infections — SDL Guide
Learning Objectives
- Describe the etiopathogenesis, clinical features, complications, and management of Helicobacter pylori infections including its role in peptic ulcer disease and gastric cancer
- Describe the clinical features, complications, and management of infections due to Pseudomonas aeruginosa and Burkholderia species
- Explain the mechanisms by which Pseudomonas and Burkholderia resist antibiotics and the implications for empirical antibiotic selection
- Apply knowledge of H. pylori eradication regimens including first-line and second-line options relevant to Indian resistance patterns
INSTRUCTIONS
This SDL covers two distinct Gram-negative bacterial infections with very different clinical roles: Helicobacter pylori as a pathogen in gastroduodenal disease (one of the most prevalent infections globally, responsible for the majority of peptic ulcers), and Pseudomonas/Burkholderia as opportunistic and nosocomial pathogens with complex antibiotic resistance. Both require precise antibiotic management decisions that reflect the India-specific resistance landscape.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 162 — Helicobacter pylori; Ch. 164 — Pseudomonas and Burkholderia (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (textbook)
- Indian Consensus on H. pylori Management, 2019 (Kolkata Consensus) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old software engineer presents with 6 months of recurrent epigastric pain, typically worse before meals and relieved by eating, associated with occasional nausea. An upper GI endoscopy reveals a 1.2 cm duodenal ulcer. Rapid urease test: positive. His older brother had a duodenal ulcer 10 years ago treated with omeprazole alone — it recurred twice. Across the ward, a 55-year-old with acute myeloid leukaemia on induction chemotherapy develops fever (39.2°C), deteriorating lung function, and a CXR showing rapidly confluent bilateral infiltrates. Blood culture flags positive at 18 hours: Gram-negative rods, oxidase-positive. These two cases illustrate the two extremes of Gram-negative bacterial infection covered in this module: H. pylori causes chronic, indolent gastroduodenal disease (treatable with a 14-day eradication course that cures the ulcer permanently), while Pseudomonas aeruginosa causes rapidly lethal opportunistic infections in the immunocompromised. The drugs used for each are entirely different, and the urgency is entirely different — but the principle is the same: identify the pathogen, understand its biology, and select the right treatment.
WHY THIS MATTERS
Helicobacter pylori infects approximately 50% of the world's population and is the leading cause of peptic ulcer disease and a type-1 carcinogen for gastric adenocarcinoma — making it one of the most clinically significant infections in internal medicine despite its slow clinical course. In India, seroprevalence reaches 70–80% in adult populations due to waterborne transmission and crowded living conditions. Pseudomonas aeruginosa is the archetype of the dangerous nosocomial Gram-negative pathogen — intrinsically resistant to many antibiotics, capable of rapidly acquiring additional resistance, and causing lethal infections in immunocompromised, ventilated, and burn patients. Burkholderia pseudomallei causes melioidosis, an important tropical infection endemic in South and Southeast Asia, including Northeastern India. Together, these NMC competencies IM26.15–IM26.16 represent essential knowledge for the physician practising in both primary care and the hospital setting.
RECALL
Recall the basic microbiology of these organisms. Helicobacter pylori is a spiral-shaped, microaerophilic, urease-producing Gram-negative bacillus — its most important biochemical property is urease production, which allows it to survive in the gastric acid environment by generating an ammonia cloud that neutralises local pH. It colonises the gastric mucosa, not the duodenal mucosa — yet duodenal ulcers are its most common complication (through gastric metaplasia in the duodenum). Pseudomonas aeruginosa is an aerobic, non-fermenting Gram-negative bacillus distinguished by its blue-green pigment (pyocyanin), fruity odour (pyocyanin/pyoriverdine), and its ability to form robust biofilms on medical devices. Burkholderia pseudomallei is also a Gram-negative non-fermenter found in soil and water in tropical latitudes; it is an intracellular pathogen capable of survival within macrophages, producing the disease melioidosis — a great clinical mimic.
Helicobacter pylori: Pathogenesis, Clinical Presentation, and Complications
Helicobacter pylori is a microaerophilic, spiral, Gram-negative bacillus that colonises the gastric mucosa of approximately 4.4 billion people globally. Despite this extraordinary prevalence, only about 15–20% of infected individuals develop clinically significant disease — a proportion determined by a complex interplay of bacterial virulence factors, host immune response, and environmental co-factors. Understanding which patients need testing and treatment is as important as knowing the treatment regimen itself. In India, seroprevalence reaches 70–80% in adult populations, driven by waterborne and faecal-oral transmission in settings with inadequate sanitation and crowded living conditions. The vast majority of infected individuals remain asymptomatic throughout their lives; this is because H. pylori colonisation of the stomach produces a spectrum of outcomes — from clinically silent gastritis to peptic ulcer disease to gastric carcinoma — determined by the interplay of the specific bacterial virulence genotype (particularly whether CagA is expressed), host genetic susceptibility (IL-1β polymorphisms that influence acid secretion), and environmental factors such as diet, smoking, and non-steroidal anti-inflammatory drug (NSAID) use.
Pathogenesis: H. pylori colonises the antrum of the stomach (preferentially — where acid production is lower), residing beneath the mucous layer adherent to gastric epithelial cells. Its key virulence factors:
- Urease: produces ammonia from urea, creating a local alkaline microenvironment that allows survival in gastric acid. Ammonia itself is directly toxic to gastric epithelium — contributing to mucosal injury.
- CagA protein (cytotoxin-associated gene A): injected into gastric epithelial cells via a type IV secretion system; disrupts cell signalling, alters epithelial polarity, promotes oncogenic transformation → strongly associated with gastric carcinoma and MALT lymphoma.
- VacA protein (vacuolating cytotoxin A): forms pores in gastric epithelial cell membranes, causing cytoplasmic vacuolation, mitochondrial damage, and apoptosis.
- Outer membrane proteins (adhesins): facilitate firm attachment to gastric epithelium.
The sequence from infection to disease proceeds through three stages: (1) initial acute gastritis (often subclinical — transient nausea, abdominal pain); (2) chronic gastritis — H. pylori triggers a persistent Th1 inflammatory response with IL-8 recruitment of neutrophils → chronic active gastritis; (3) the downstream consequence depends on the pattern of gastritis: antral-predominant gastritis (the most common in India) → high acid output → increased risk of duodenal ulcer; pangastritis → corpus involvement → atrophic gastritis → hypochlorhydria → increased risk of gastric ulcer and gastric carcinoma.
Clinical presentations of H. pylori infection:
1. Chronic peptic ulcer disease (PUD): H. pylori accounts for ~80–90% of duodenal ulcers and ~70–80% of gastric ulcers (NSAID use is the second major cause). Classic duodenal ulcer: epigastric pain, gnawing or burning, worse when stomach is empty (2–3 hours after meals) and at night, relieved by food or antacids. Gastric ulcer: epigastric pain often precipitated by eating. Complications: haemorrhage (haematemesis, melaena), perforation (sudden severe abdominal pain, peritonitis), gastric outlet obstruction (recurrent vomiting of undigested food).
2. Functional dyspepsia: a significant proportion of H. pylori-positive patients have dyspepsia (upper abdominal discomfort, bloating, nausea) without ulcer on endoscopy. H. pylori eradication benefits a subgroup (~10% have symptom resolution — the 'test and treat' strategy is cost-effective in this setting).
3. Gastric adenocarcinoma: H. pylori is a WHO Group I carcinogen for non-cardia gastric cancer. The carcinogenic sequence (Correa cascade): H. pylori chronic gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → carcinoma. This sequence takes decades, but H. pylori eradication at any stage before dysplasia halts progression.
4. MALT lymphoma (Mucosa-Associated Lymphoid Tissue lymphoma): a low-grade B-cell lymphoma of the gastric MALT; driven by chronic antigen stimulation from H. pylori. H. pylori eradication alone leads to complete remission in 60–80% of low-grade MALT lymphoma confined to the stomach (Stage I).
5. Extra-gastric associations: H. pylori has been associated with iron-deficiency anaemia (gastric acid is needed for non-haem iron absorption; H. pylori reduces acid and competes for iron), idiopathic thrombocytopenic purpura (ITP — platelet antibodies may cross-react with H. pylori antigens; eradication improves platelet count in ~50%), and ischaemic heart disease (less established).
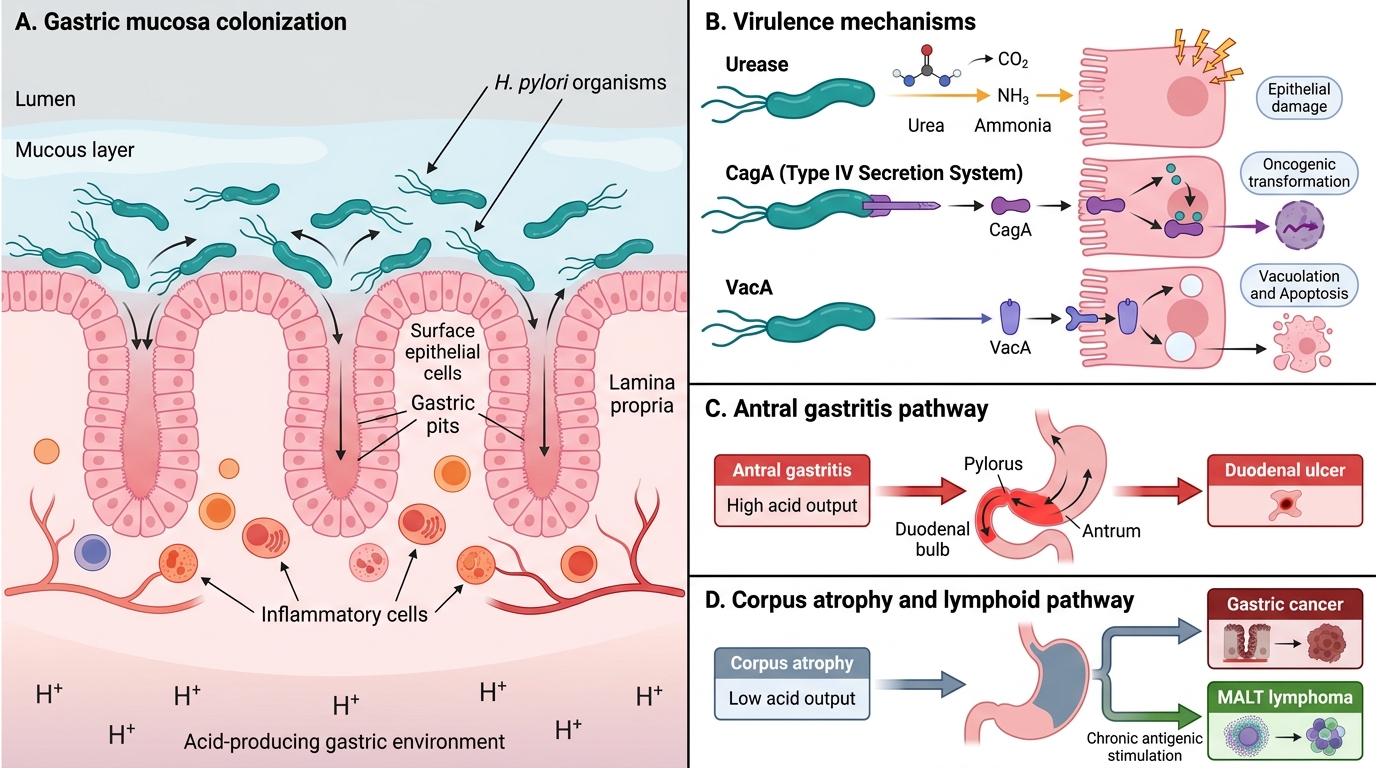
H. pylori Pathogenesis and Disease Spectrum
H. pylori Diagnosis and Eradication Therapy
Diagnosis of H. pylori uses either non-invasive tests (when endoscopy is not required for clinical management) or invasive endoscopy-based tests (when endoscopy is already indicated for other reasons — e.g., suspected PUD, upper GI bleeding, suspected malignancy). All tests have specific requirements regarding proton pump inhibitor (PPI) and antibiotic use before testing — failure to observe these washout periods causes false-negative results. The choice of diagnostic test is guided by clinical context: when endoscopy is being performed anyway (for ulcer confirmation, bleeding, or suspicion of malignancy), the rapid urease test on an antral biopsy provides an immediate result with high sensitivity and negligible additional cost; when endoscopy is not clinically indicated (young patient with dyspepsia, no alarm features), a non-invasive test avoids unnecessary invasive procedures and is both accurate and cost-effective. Understanding the strengths and limitations of each test — particularly the washout requirements — prevents the common error of false-negative results in patients who tested positive on a prior occasion but are now being reassessed after stopping PPIs only days before the test.
Non-invasive tests:
- Urea breath test (UBT) — gold standard for non-invasive testing: the patient ingests ¹³C-labelled urea; H. pylori urease hydrolyses it to labelled CO₂, which is detected in exhaled breath. Sensitivity ~95%, specificity ~96%. Requires PPI stopped ≥2 weeks before the test; antibiotics stopped ≥4 weeks before. The preferred test for confirming eradication (performed ≥4 weeks after completing treatment).
- H. pylori stool antigen test (HpSA ELISA): detects H. pylori antigens in stool; sensitivity ~94%, specificity ~97%. Requires same washout as UBT. Practical in resource-limited settings. Also used to confirm eradication.
- Serology (IgG ELISA): detects antibodies to H. pylori; sensitivity ~85%, specificity ~79% in India. Does NOT distinguish active from past infection — remains positive for years after eradication. NOT recommended for confirming eradication. Used primarily for epidemiological surveys.
Invasive (endoscopy-based) tests:
- Rapid urease test (RUT / CLO test): antral biopsy placed in urea-containing medium with pH indicator; urease from H. pylori hydrolyses urea → ammonia → colour change. Result in 30–60 minutes; sensitivity ~90%, specificity ~95%. The most widely used test in India when endoscopy is performed. Requires PPI stopped ≥2 weeks.
- Histology: multiple biopsies from antrum + corpus; Giemsa or Warthin-Starry staining; gold standard for mucosal staging (gastritis, atrophy, metaplasia, dysplasia); important when carcinoma or MALT is suspected.
- Culture: required when antibiotic susceptibility testing is needed (treatment failure, suspected resistant H. pylori); technically demanding; not routine.
Indications for H. pylori testing and eradication: the 'test and treat' strategy is appropriate in all patients with: (1) confirmed peptic ulcer disease; (2) uninvestigated dyspepsia in patients <45 years without alarm features (test before endoscopy); (3) MALT lymphoma; (4) early gastric cancer post-resection; (5) first-degree relatives of gastric cancer patients; (6) long-term NSAID or aspirin use (reducing ulcer risk). All confirmed H. pylori-positive patients should be offered eradication.
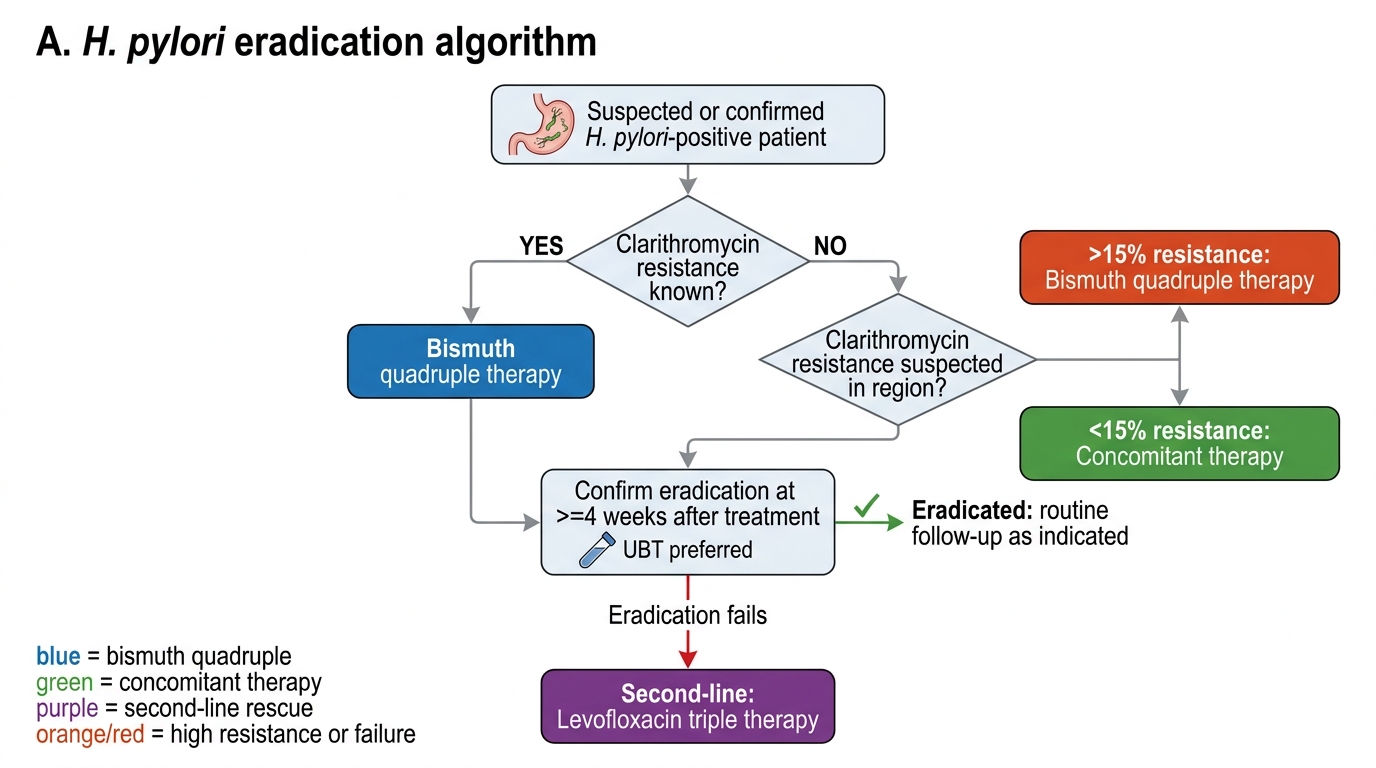
Eradication regimens — India-specific: Clarithromycin resistance is rising in India (estimated 15–30% in many states), meaning the traditional 7-day triple therapy (PPI + clarithromycin + amoxicillin) achieves only ~70–75% eradication rates — below the acceptable threshold of >90%. Current guidelines (Kolkata Consensus 2019) recommend:
| Regimen | Drugs | Duration | Notes |
|---|---|---|---|
| Bismuth quadruple therapy (first-line in high clarithromycin resistance areas) | Bismuth subsalicylate 525 mg QID + PPI BD + metronidazole 500 mg TID + tetracycline 500 mg QID | 14 days | Eradication rate >90%; preferred when clarithromycin resistance >15% |
| Concomitant therapy (non-bismuth quadruple, first-line alternative) | PPI BD + clarithromycin 500 mg BD + amoxicillin 1g BD + metronidazole 500 mg BD | 14 days | All four drugs given simultaneously; eradication ~88–92% |
| Sequential therapy (declining use) | PPI + amoxicillin 1g BD × 5 days, then PPI + clarithromycin + metronidazole × 5 days | 10 days | Historically used; lower eradication in high-metronidazole resistance settings |
| Levofloxacin triple therapy (second-line / rescue) | PPI BD + levofloxacin 500 mg OD + amoxicillin 1g BD | 14 days | Used after first-line failure; check local fluoroquinolone resistance |
Key eradication principles: (1) always confirm eradication with UBT or stool antigen at ≥4 weeks post-treatment; (2) proton pump inhibitor use significantly enhances antibiotic efficacy — ensure PPI compliance; (3) metronidazole-resistant strains are common in India; (4) after successful eradication, duodenal ulcers heal without further antisecretory therapy in most patients; gastric ulcers should be re-endoscoped to confirm healing and exclude malignancy; (5) MALT lymphoma should be re-staged endoscopically at 3 months post-eradication to confirm regression.
H. pylori Eradication Algorithm
SELF-CHECK
A 42-year-old man with a 1.5 cm duodenal ulcer on endoscopy tests positive for H. pylori by rapid urease test. He has no penicillin allergy. You plan to prescribe H. pylori eradication therapy. In a region with known high clarithromycin resistance (estimated 25%), which regimen is MOST appropriate?
A. 7-day standard triple therapy: PPI + clarithromycin + amoxicillin
B. 14-day bismuth quadruple therapy: PPI + bismuth + metronidazole + tetracycline
C. 14-day PPI monotherapy — H. pylori eradication is not needed for duodenal ulcers
D. 10-day sequential therapy: PPI + amoxicillin × 5 days, then PPI + clarithromycin + metronidazole × 5 days
Reveal Answer
Answer: B. 14-day bismuth quadruple therapy: PPI + bismuth + metronidazole + tetracycline
When clarithromycin resistance is >15%, standard triple therapy (PPI + clarithromycin + amoxicillin) achieves unacceptably low eradication rates (~70–75%). Bismuth quadruple therapy (PPI + bismuth + metronidazole + tetracycline × 14 days) achieves eradication rates >90% regardless of clarithromycin resistance, and is the preferred regimen in high-resistance areas per the Kolkata Consensus 2019. PPI monotherapy does not eradicate H. pylori — the ulcer will recur. Sequential therapy achieves lower eradication rates in settings with high metronidazole resistance, which is also common in India.
Pseudomonas aeruginosa and Burkholderia Infections
Pseudomonas aeruginosa is one of the most dangerous nosocomial Gram-negative pathogens, combining three characteristics that make it particularly difficult to treat: (1) intrinsic resistance to many antibiotics; (2) rapid acquisition of additional resistance through mutation and horizontal gene transfer; and (3) biofilm formation on medical devices (ventilator tubing, urinary catheters, central venous lines, prosthetic joints) that renders infections effectively untreatable without device removal. Understanding which patients are at risk for Pseudomonas, which antibiotics retain activity, and how resistance develops is essential for both empirical antibiotic selection and stewardship.
Provided image
Pseudomonas virulence and pathogenesis: P. aeruginosa is ubiquitous in the environment (water, soil, drains, hospital water systems) and is a commensal of the gastrointestinal and skin flora in up to 10% of healthy individuals. It causes disease almost exclusively in the setting of impaired host defences — it is the archetype of the opportunistic pathogen. Virulence mechanisms:
- Biofilm formation: encased in an alginate polysaccharide matrix, Pseudomonas in biofilms is 100-fold more antibiotic-resistant and essentially invisible to host phagocytes
- Type III secretion system: injects exotoxins (ExoS, ExoT, ExoU) directly into host cells; ExoU causes acute alveolar damage and is associated with rapid lung destruction in ventilator-associated pneumonia
- Exotoxin A: ADP-ribosylates elongation factor 2 (EF-2) → inhibits protein synthesis (similar mechanism to diphtheria toxin)
- Proteases, elastases, and phospholipases: destroy connective tissue, enabling invasive spread
- Pyocyanin: a blue-green pigment that generates reactive oxygen species, damaging host tissues
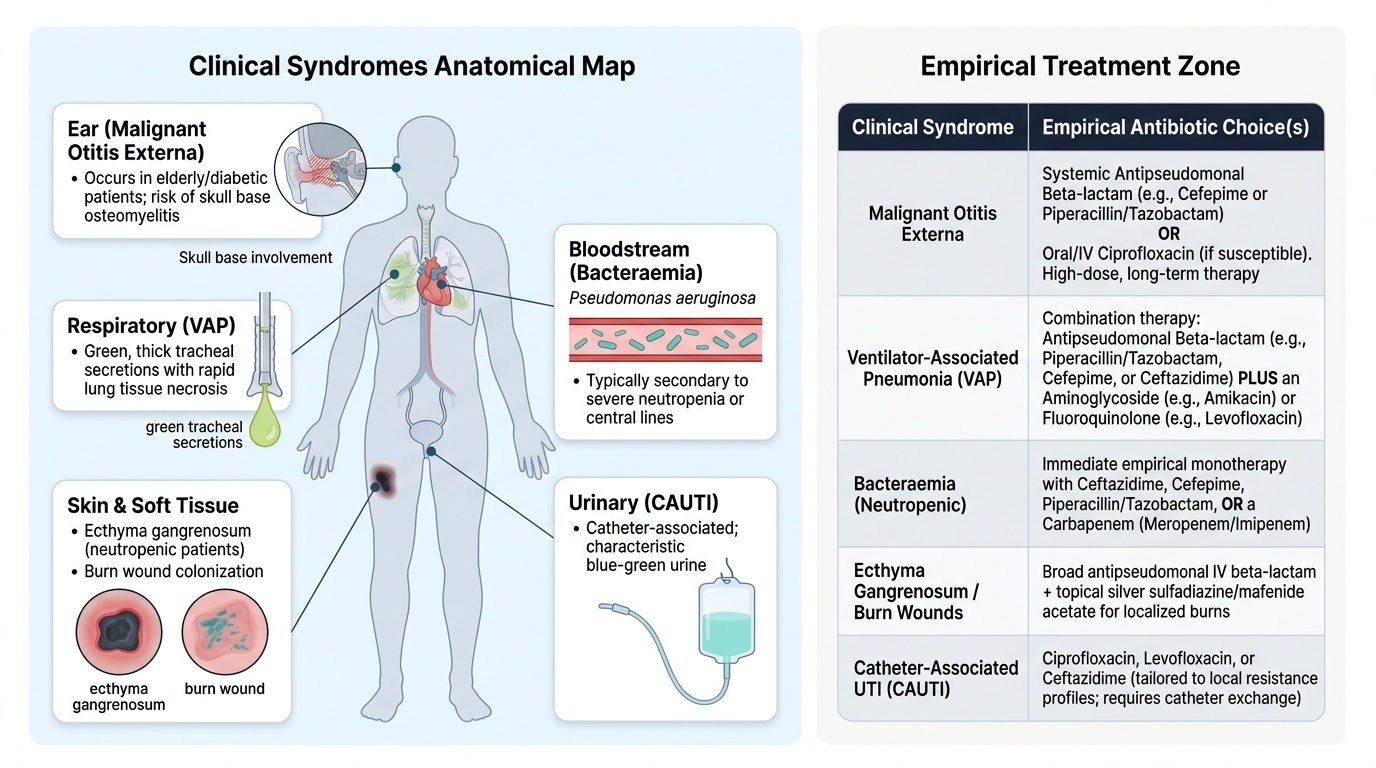
Clinical syndromes caused by Pseudomonas aeruginosa:
- Ventilator-associated pneumonia (VAP): P. aeruginosa is the single most common cause of VAP in ICU patients (20–30% of VAP cases). Intubated patients colonised with Pseudomonas are at high risk of progression to VAP. Clinical features: fever, increasing tracheal secretions (often greenish), worsening oxygenation, new CXR infiltrates. Diagnosis: quantitative tracheal aspirate or bronchoalveolar lavage (BAL) culture. Treatment: IV anti-pseudomonal beta-lactam (piperacillin-tazobactam, cefepime, or meropenem) ± anti-pseudomonal aminoglycoside (amikacin) or IV ciprofloxacin for combination therapy in severe cases. Duration: 8 days (non-inferior to 15 days, reduces resistance selection).
- Bacteraemia (Pseudomonas bloodstream infection): occurs in neutropenic patients (haematological malignancy, chemotherapy), burns, and patients with central venous catheters. Mortality 20–40% without appropriate antibiotics. Characteristic skin lesion: ecthyma gangrenosum — a necrotic skin ulcer with a black eschar and surrounding erythema, caused by Pseudomonas vascular invasion; pathognomonic in a neutropenic febrile patient.
- Burn wound infection: P. aeruginosa is the leading cause of wound infection and septicaemia in burns (>25% TBSA). The devascularised eschar provides an ideal anaerobic, nutrient-rich environment for growth.
- Otitis externa (swimmer's ear): localised Pseudomonas infection of the external auditory canal; usually benign and treated with topical ciprofloxacin or gentamicin. Malignant otitis externa is an invasive Pseudomonas infection of the external ear canal extending to the temporal bone and skull base — occurs almost exclusively in elderly diabetics; cranial nerve VII palsy (and other cranial nerve palsies) develop as the infection spreads; treated with IV anti-pseudomonal therapy for 6 weeks.
- Hot tub folliculitis: Pseudomonas folliculitis from contaminated water in hot tubs or swimming pools; self-limited; no systemic antibiotics needed.
- Urinary tract infection: common in catheterised patients; produces characteristic blue-green discolouration of urine and tubing (pyocyanin pigment).
Antibiotic resistance in Pseudomonas: P. aeruginosa is intrinsically resistant to aminopenicillins, first and second-generation cephalosporins, and most carbapenems except imipenem/meropenem. Active against Pseudomonas: piperacillin-tazobactam, ceftazidime, cefepime, imipenem, meropenem, ciprofloxacin, amikacin, colistin. Resistance mechanisms: (a) AmpC beta-lactamase (inducible, chromosomal) — derepressed during beta-lactam therapy; (b) efflux pumps (MexAB-OprM) — reduce intracellular antibiotic concentration; (c) loss of OprD outer membrane porin — confers carbapenem resistance. Combination therapy (two active agents) is used in life-threatening Pseudomonas infections to reduce the emergence of resistance.
Burkholderia pseudomallei and melioidosis: B. pseudomallei is an intrinsically antibiotic-resistant Gram-negative non-fermenter found in soil and water in tropical latitudes. It is endemic in Southeast Asia and is increasingly recognised in Northeastern India, Odisha, and Tamil Nadu. Melioidosis is called the 'great mimicker' because it can present as pneumonia, septicaemia, cutaneous abscess, liver/spleen abscess, or neurological infection — mimicking TB, typhoid, and other common tropical diseases. Transmission: inhalation or skin contact with contaminated soil/water, particularly during the monsoon season. Risk factors: diabetes mellitus (the single strongest risk factor — accounting for 50–60% of cases), renal disease, thalassaemia, excessive alcohol use. Treatment: intensive phase — IV ceftazidime 2g 8-hourly OR IV meropenem 1g 8-hourly × 10–14 days; eradication phase — oral TMP-SMX (co-trimoxazole) + doxycycline × 3–6 months (to prevent relapse, which occurs in ~15% without eradication therapy). Important: B. pseudomallei is intrinsically resistant to ampicillin, first-generation cephalosporins, gentamicin, and colistin — these must not be used.
SELF-CHECK
A 65-year-old male diabetic is hospitalised for uncontrolled diabetes and develops fever (39.5°C), severe right ear pain, purulent ear discharge, and facial nerve palsy (right). Examination reveals granulation tissue in the external auditory canal. Blood culture grows Pseudomonas aeruginosa. What is the MOST appropriate management?
A. Topical ciprofloxacin ear drops for 7 days — otitis externa is a localised infection
B. IV piperacillin-tazobactam for 6 weeks + CT scan of temporal bone/skull base to assess extent
C. IV vancomycin — Pseudomonas otitis externa is usually caused by MRSA in diabetics
D. Oral ciprofloxacin 500 mg twice daily for 14 days — fluoroquinolones have excellent Pseudomonas coverage
Reveal Answer
Answer: B. IV piperacillin-tazobactam for 6 weeks + CT scan of temporal bone/skull base to assess extent
This is malignant (necrotising) otitis externa — a Pseudomonas infection in an elderly diabetic that has extended to the temporal bone and skull base, evidenced by cranial nerve VII palsy and granulation tissue in the auditory canal. It requires IV anti-pseudomonal therapy for 6 weeks (piperacillin-tazobactam, ceftazidime, or ciprofloxacin IV) plus CT/MRI skull base to delineate extent and guide surgical debridement of necrotic tissue. Topical drops are for uncomplicated swimmer's ear — entirely inadequate here. Oral ciprofloxacin alone is insufficient for invasive skull base infection with bacteraemia. Vancomycin has no anti-pseudomonal activity.