Page 16 of 35
IM26.18-20 | Zoonotic Rickettsial and Filamentous Bacterial Infections — SDL Guide (Part 2)
Management Summary and Diagnostic Approach for Zoonotic and Rickettsial Infections
The management of zoonotic and rickettsial infections requires two key clinical skills that complement each other: first, the ability to generate the correct syndromic diagnosis from the epidemiological exposure and clinical pattern before test results return; second, the ability to select the correct specific antibiotic regimen, since the pathogens in this group are not covered by standard empirical broad-spectrum regimens (beta-lactams are inactive against rickettsiae, Brucella, and Leptospira; doxycycline — the most important antibiotic in this group — is not included in most hospital empirical protocols). Recognising these infections early is critical because the window between presentation and life-threatening organ failure is narrow for plague, inhalation anthrax, severe leptospirosis, and rickettsial encephalitis.
Diagnostic approach — the exposure-to-syndrome matrix: When evaluating any patient with unexplained acute febrile illness, a structured exposure history unlocks the differential diagnosis in this group:
| Exposure | Time to illness | Distinguishing feature | Likely diagnosis |
|---|---|---|---|
| Waterlogged fields / flooding / swimming in contaminated water | 2–30 days | Conjunctival suffusion, AKI, jaundice | Leptospirosis |
| Cattle, goats, sheep (calving, abattoir, unpasteurised dairy) | 1–4 weeks | Undulating fever, night sweats, back pain/sacroiliitis | Brucellosis |
| Rodent exposure (rat flea bite) / urban slum | 1–2 weeks | Macular rash trunk→periphery, no eschar | Endemic (murine) typhus |
| Tick/chigger bite (forest, grassland, post-monsoon) | 1–3 weeks | Eschar + fever + rash | Scrub typhus |
| Animal hide/wool/carcass contact (cattle, goats) | 1–5 days | Painless black eschar with gelatinous oedema | Cutaneous anthrax |
| Crowded, unsanitary conditions / louse infestation | 1–2 weeks | Severe headache, rash (spares face/palms/soles) | Epidemic typhus |
| Rat/flea exposure + inguinal painful lymph node mass | 2–8 days | Bubo (acutely tender lymph node) + fever | Bubonic plague |
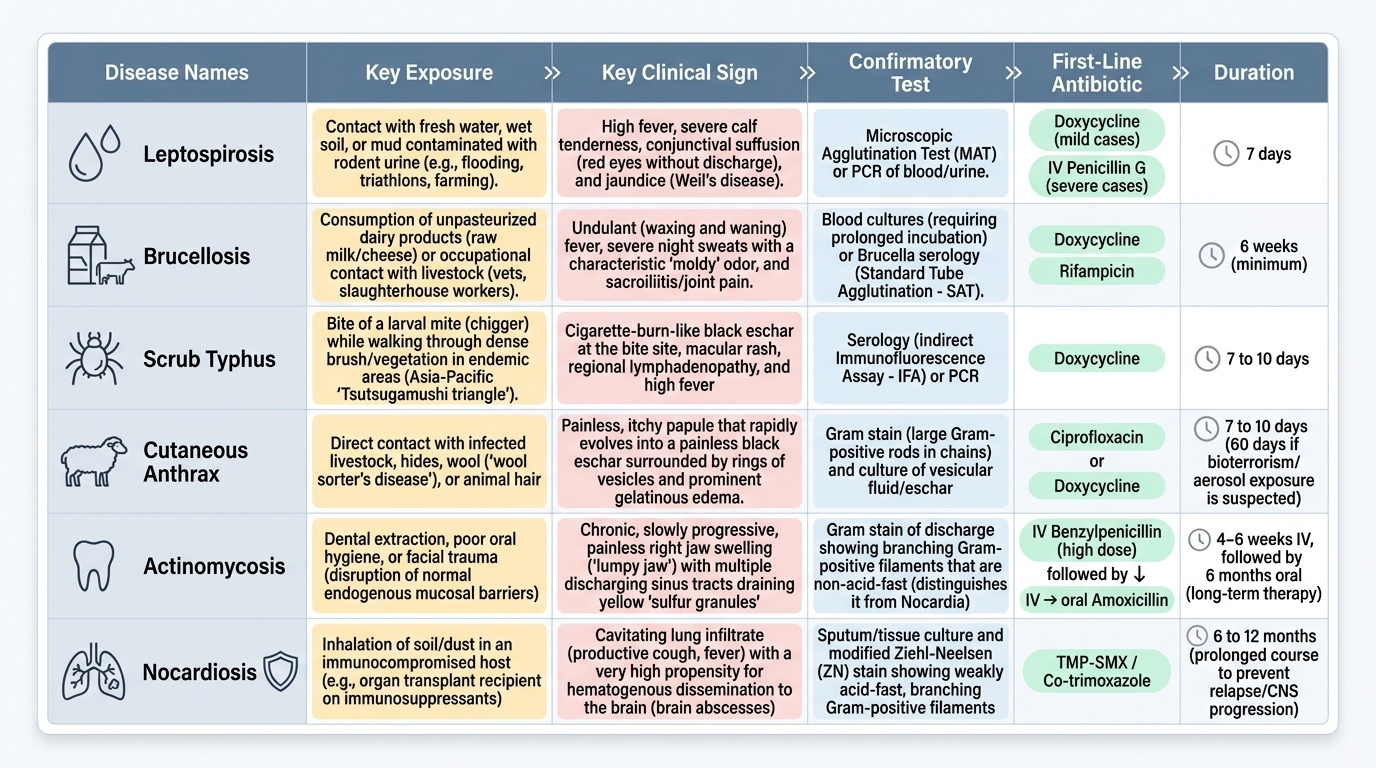
Treatment summary:
| Infection | First-line treatment | Duration | Key notes |
|---|---|---|---|
| Leptospirosis (mild) | Doxycycline 100 mg BD oral | 7 days | Start early |
| Leptospirosis (severe — Weil's) | IV penicillin G 1.5 MU 6-hourly OR IV ceftriaxone 1g daily | 7 days | ICU, dialysis if AKI |
| Brucellosis (uncomplicated) | Doxycycline 100 mg BD × 6 weeks + gentamicin IV × 7 days (or rifampicin × 6 weeks) | 6 weeks | Never monotherapy |
| Brucellosis (spondylodiscitis) | Doxycycline + rifampicin + streptomycin | 3–6 months | Neurosurgery if cord compression |
| Scrub typhus | Doxycycline 100 mg BD | 7 days | Fever resolves in 24–48h |
| Epidemic/endemic typhus | Doxycycline 100 mg BD | 7 days | Same regimen |
| Bubonic plague | Gentamicin 5 mg/kg IV daily OR streptomycin 15 mg/kg IM BD | 10 days | Doxycycline alternative |
| Cutaneous anthrax | Ciprofloxacin 500 mg BD oral | 7 days | IV for severe cases |
| Actinomycosis | Benzylpenicillin IV → oral amoxicillin | 6–12 months | Long course essential |
| Nocardiosis (pulmonary) | TMP-SMX | 6–12 months | IV imipenem + amikacin for CNS |
Doxycycline as the 'umbrella antibiotic' for this group: Doxycycline covers leptospirosis (mild), all rickettsial diseases (scrub, epidemic, endemic typhus, RMSF), brucellosis (component of combination), plague (alternative to gentamicin), and cutaneous anthrax (alternative to ciprofloxacin). In a febrile patient with zoonotic exposure and no organ failure, empirical doxycycline is appropriate while awaiting specific serology results — the risk-benefit strongly favours early treatment.
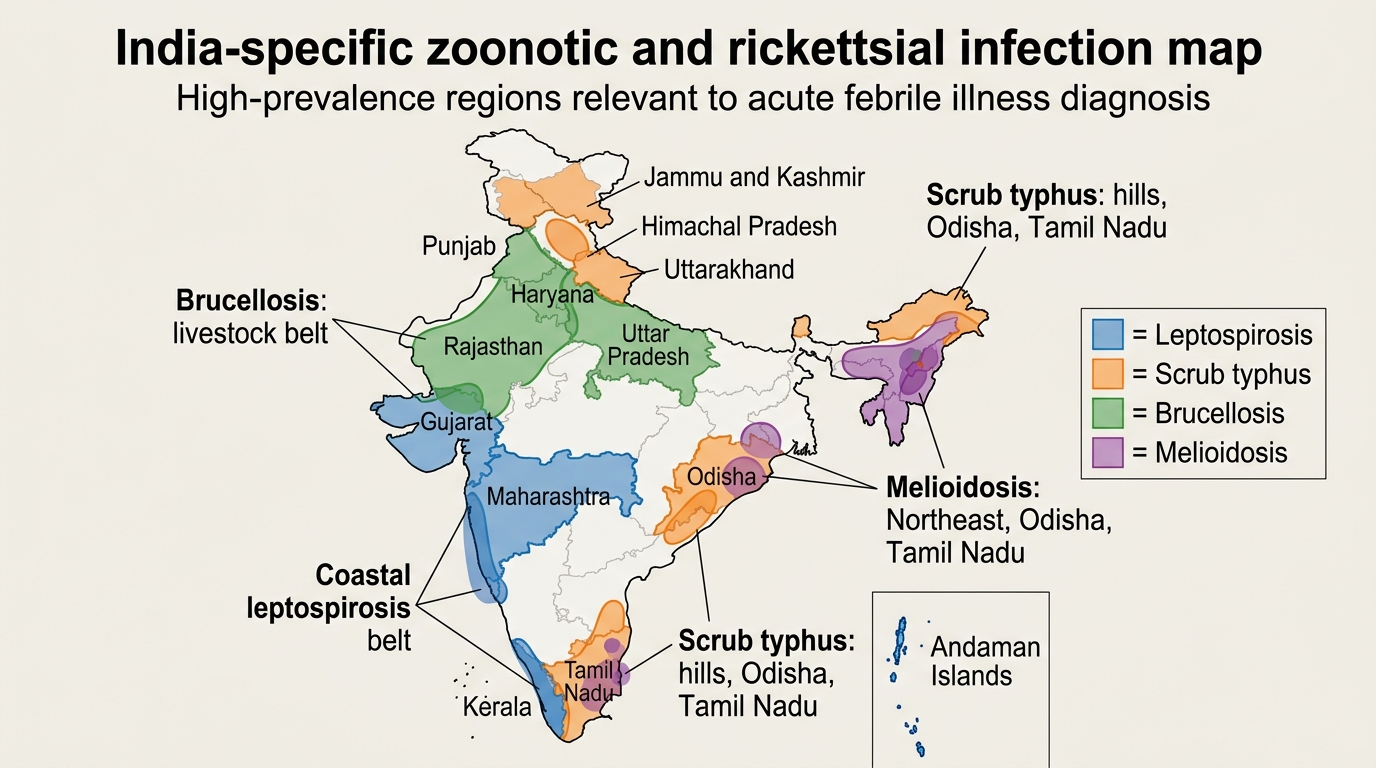
India Map of Key Zoonotic and Rickettsial Infections
Self-Assessment: Zoonotic, Rickettsial, and Filamentous Bacterial Infections
You have now covered the full spectrum of zoonotic and rickettsial infections, including leptospirosis, brucellosis, plague, anthrax, actinomycosis, nocardiosis, and the three major rickettsial syndromes. The scenarios below apply the exposure-to-syndrome diagnostic framework across these conditions. Work through each before reading the analysis.
Provided image
Scenario A: A 55-year-old woman presents with 4 months of progressively worsening right jaw swelling, low-grade fever, and multiple discharging sinuses through the skin overlying the jaw. She had a molar extraction 5 months ago. The discharge contains small yellow granules. Gram stain of the discharge: branching Gram-positive filaments, non-acid-fast.
Analysis: Dental extraction triggering jaw swelling → multiple discharging sinuses → yellow sulphur granules → branching Gram-positive filaments = cervicofacial actinomycosis. Non-acid-fast distinguishes Actinomyces from Nocardia (which is weakly acid-fast). Treatment: IV benzylpenicillin 18–24 million units/day × 4–6 weeks, then oral amoxicillin × 6 months. Surgical debridement of the fibrous mass may be needed. Key: the diagnosis is often delayed because the chronic indolent presentation mimics malignancy or TB.
Scenario B: A 42-year-old male renal transplant recipient on tacrolimus and prednisolone presents with 3 weeks of productive cough, fever, and weight loss. CXR shows a right upper lobe cavitating infiltrate. AFB smear is negative ×3. Sputum culture grows aerobic filamentous bacteria that are weakly acid-fast on modified ZN stain. A brain MRI is ordered to check for dissemination.
Analysis: Immunocompromised patient (tacrolimus + prednisolone) + cavitating lung infiltrate + AFB-negative + weakly acid-fast filamentous bacteria = pulmonary nocardiosis (Nocardia asteroides). Brain MRI is essential — 25% of disseminated nocardiosis has concurrent brain abscess. Treatment: oral TMP-SMX (co-trimoxazole) for uncomplicated pulmonary nocardiosis in a stable immunocompromised patient; IV imipenem + amikacin + TMP-SMX triple therapy if CNS involvement. Duration: 6–12 months.
Scenario C: A 26-year-old medical student doing elective fieldwork in Tamil Nadu during the post-monsoon season develops fever (40°C), headache, and an intensely black 8 mm lesion in his left axilla that he didn't notice until the clinical examination. He recalls working in a forested area collecting tick samples 10 days ago. IgM ELISA for scrub typhus: reactive. He has no drug allergies.
Analysis: Tick/mite exposure in Tamil Nadu during post-monsoon season + eschar in the axilla + IgM ELISA positive = scrub typhus. Start doxycycline 100 mg twice daily × 7 days immediately. Expect fever to resolve within 24–48 hours — this dramatic response is itself a diagnostic indicator. The eschar is the key clinical finding; explicit examination of concealed skin folds (axilla, groin, scalp hairline, popliteal fossa, belt line) is essential in any febrile patient from an endemic region.
Scenario D: During flood relief operations in Kerala, a 35-year-old rescue worker develops acute onset fever (39.8°C), severe bilateral calf muscle pain, and conjunctival suffusion on day 5 of the operation. Urinalysis shows 2+ proteinuria and haematuria. Creatinine 2.8 mg/dL. Bilirubin 4.2 mg/dL (conjugated). Platelet count 68,000/µL.
Analysis: Flood relief work (waterlogged soil exposure) + conjunctival suffusion + AKI + hepatic involvement + thrombocytopenia = Weil's disease (severe leptospirosis). This is beyond the anicteric phase — organ failure is present. LEPTO IgM ELISA (ordered now — will be positive by day 5–7); treat immediately: IV penicillin G 1.5 MU 6-hourly × 7 days (or IV ceftriaxone 1g daily). ICU management: IV fluid resuscitation for AKI (maintain urine output >0.5 mL/kg/hour), monitor for pulmonary haemorrhage syndrome (the most feared complication), dialysis if oliguria or creatinine worsening. Notify local health authorities (notifiable disease).
CLINICAL PEARL
Three high-yield clinical pearls for this SDL: (1) The eschar of scrub typhus is in concealed skin folds — groin, axilla, scalp hairline, popliteal fossa, belt line. Every febrile patient from an endemic region during post-monsoon season must have these sites explicitly examined; missing the eschar means missing the diagnosis. (2) Brucellosis must NEVER be treated with a single antibiotic — monotherapy leads to relapse in >80% of cases. The minimum is doxycycline × 6 weeks paired with either a 7-day gentamicin course or rifampicin × 6 weeks. (3) Doxycycline is the 'umbrella antibiotic' for this group — it covers leptospirosis, all rickettsial diseases, brucellosis (as part of combination), plague, and cutaneous anthrax. In a febrile patient with zoonotic exposure and no immediate life-threatening organ failure, empirical doxycycline is a reasonable and often life-saving bridge while awaiting specific serology.