Page 5 of 22
IM28.8-10 | Obstructive Airway Disease Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit, document, and present a focused medical history that differentiates aetiologies of obstructive airway disease, assesses severity, and identifies precipitants
- Perform a systematic respiratory examination that establishes diagnosis and severity, including measurement of respiratory rate, assessment of respiratory distress, breath sounds, added sounds, and identification of consolidation, pleural effusion, and pneumothorax
- Generate a prioritised differential diagnosis for obstructive airway disease based on clinical features and history
INSTRUCTIONS
Clinical evaluation of obstructive airway disease is a skills-based competency that requires integrating history, examination, and clinical reasoning to distinguish asthma from COPD, identify severity and precipitants, and generate a differential diagnosis. This module builds the systematic clinical method you will use at every patient encounter involving breathlessness and wheeze.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 281–282 — Clinical Assessment in Asthma and COPD (textbook)
- API Textbook of Medicine, 10th ed. — History and Examination in Respiratory Disease (textbook)
- Hutchison's Clinical Methods, 24th ed., Ch. 5 — Respiratory System (textbook)
- GINA Report 2023 — Clinical Diagnosis and Severity Assessment (guideline)
- GOLD Report 2023 — Diagnosis and Assessment of COPD (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive in the same outpatient clinic. The first is a 24-year-old woman who describes episodic chest tightness and wheeze that began after a cold three months ago — worse at night, better by midday, and triggered by exercise at the gym. Her FEV1 before and after salbutamol shows a 400 mL improvement. The second is a 62-year-old retired farmer who has had a daily productive cough for five years and increasing breathlessness for two — he smokes 30 cigarettes a day and cannot walk more than 100 metres on the flat. Both have airway obstruction, but the history alone separates them before a single investigation is ordered. In clinical practice, 80% of the diagnostic information in respiratory disease comes from the history. Mastering the structured history and systematic examination is not a preamble to 'real' medicine — it IS the medicine.
WHY THIS MATTERS
The ability to take a targeted history and perform a systematic examination that yields a working diagnosis and severity assessment is the core clinical skill tested in NMC final-year OSPE and clinical examinations. In real practice — particularly in resource-limited Indian settings where spirometry may not be immediately available — the clinical evaluation must carry the diagnostic weight. Competencies IM28.8, IM28.9, and IM28.10 require you not only to know what to ask and examine, but to perform these skills demonstrably — at the SH (Skills and Higher) level — and to generate a reasoned differential diagnosis from the findings.
RECALL
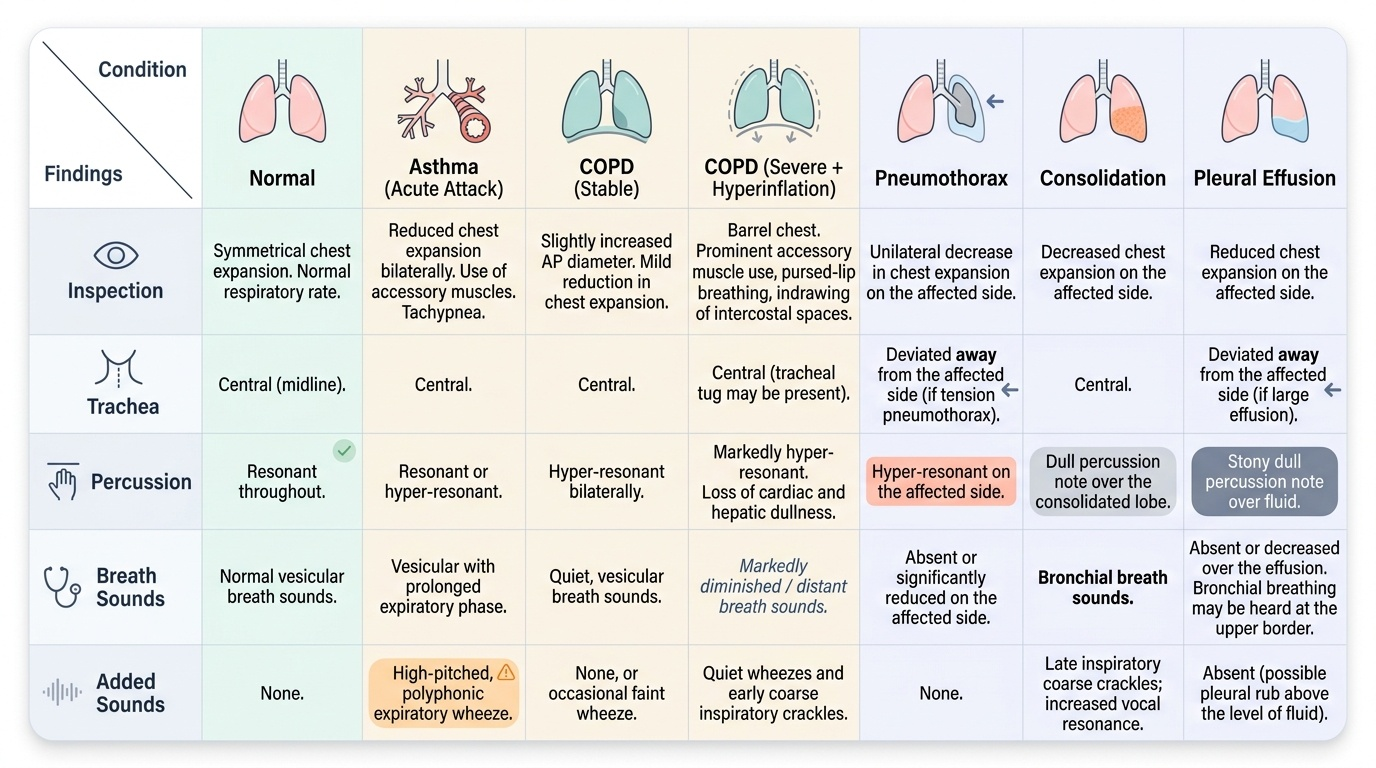
Before proceeding, recall the normal respiratory examination findings. On inspection: the chest is symmetrical, respiratory rate 12–18/min in adults, no accessory muscle use, no cyanosis or finger clubbing. Trachea is central. On percussion: resonant throughout both lung fields. On auscultation: vesicular breath sounds (soft, rustling, heard throughout inspiration and the first third of expiration) are normal; no added sounds. Abnormal added sounds include wheeze (continuous musical sound from oscillating airway walls — high-pitched if small airways, low-pitched rhonchi if large airways), crackles (discontinuous short sounds from re-opening of collapsed small airways — early inspiratory crackles in small airway disease, late inspiratory crackles in pulmonary oedema and fibrosis), and pleural rub (leathery creaking from inflamed pleural surfaces). Bronchial breath sounds (harsh, tubular, with an audible expiratory pause equal to inspiration) indicate consolidation. Recall also that percussion dullness indicates consolidation or effusion; hyper-resonance indicates pneumothorax or emphysematous hyperinflation.
Taking the History: Indication, Relevance, and Structured Approach
The clinical indication for a detailed respiratory history is any presentation involving breathlessness, cough, wheeze, chest tightness, or recurrent respiratory infections. In the context of suspected obstructive airway disease, the history must accomplish five specific goals: (1) characterise the nature and pattern of symptoms to determine whether the clinical picture is consistent with asthma, COPD, or another diagnosis; (2) quantify severity — using validated frameworks like the MRC dyspnoea scale for COPD and GINA control levels for asthma; (3) identify precipitants and triggers — because knowing what makes the patient worse is directly actionable for management; (4) establish risk factor exposure — smoking history (pack-years), biomass fuel use, occupational exposures, atopy, and childhood respiratory illness; and (5) assess impact on function and quality of life — to inform the treatment goal and to anchor the severity assessment in the patient's lived experience rather than just physiological parameters.
Provided image
A structured history in obstructive airway disease follows the standard format but with disease-specific elaborations at each step:
Presenting complaint and history of presenting complaint:
For each respiratory symptom — breathlessness, cough, wheeze, chest tightness — ask about onset (sudden vs gradual), duration (episodic vs constant), pattern (daily, nocturnal, exercise-related, seasonal, occupational), triggers (cold air, exercise, allergens, infections, NSAIDs, occupational exposures), severity (how far can you walk? can you climb stairs? are you breathless at rest?), relieving factors (does it resolve spontaneously? with an inhaler? how quickly?), and associated symptoms (fever — suggests infection; haemoptysis — raises TB, malignancy, bronchiectasis; weight loss — TB, malignancy; orthopnoea, ankle oedema — heart failure as confounder or comorbidity).
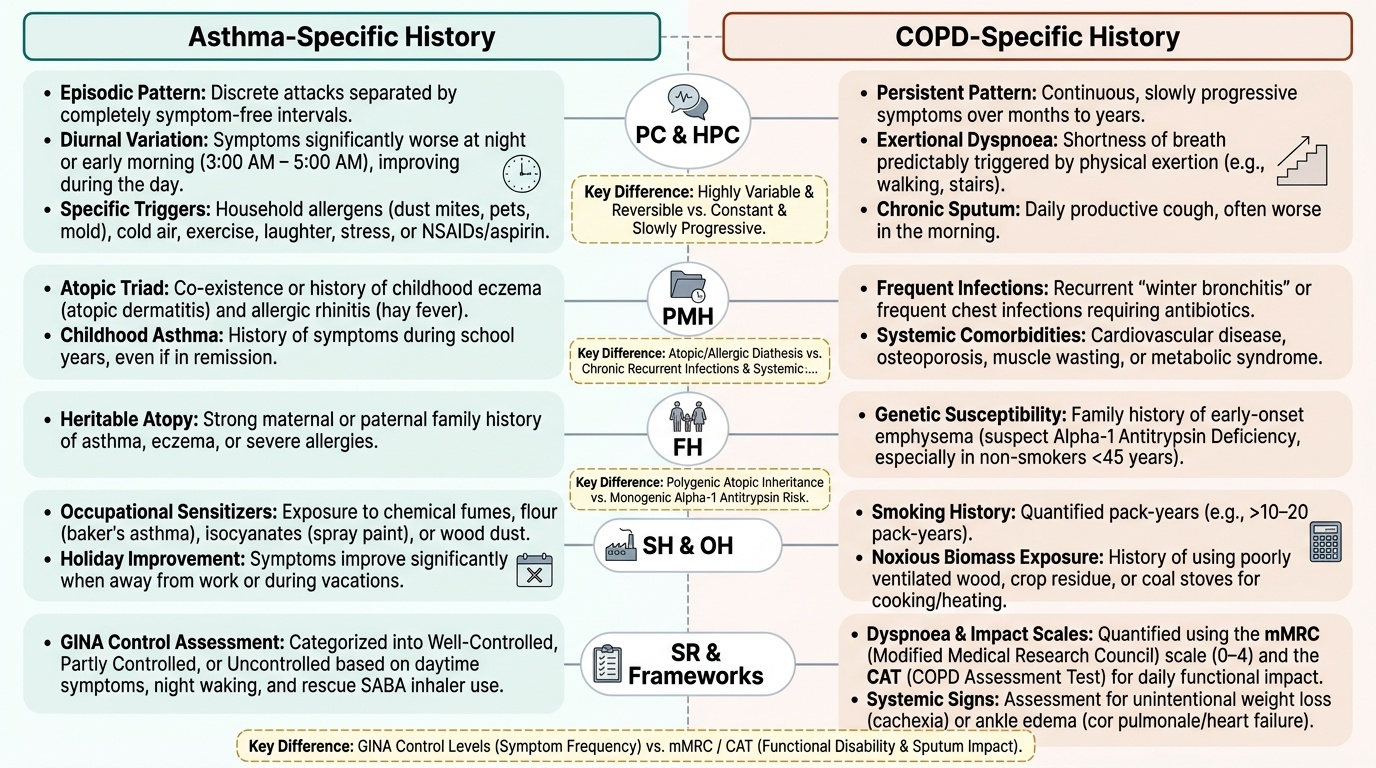
For asthma history, the following specific features are high yield:
- Diurnal pattern: symptoms worse in early morning (3–5 AM) or night-time; improvement during the day; symptom-free intervals between episodes
- Episodic pattern: discrete attacks separated by normal periods
- Triggers: household allergens (dust, pets, mould), exercise, cold air, viral URTIs, aspirin/NSAIDs, occupational agents, stress
- Seasonal variation: pollinosis-associated worsening (post-monsoon, winter)
- Atopic history: personal or family history of eczema, allergic rhinitis ("hay fever"), food allergy
- Response to bronchodilator: rapid, complete relief with salbutamol inhaler — highly characteristic
For COPD history, the high-yield specific features are:
- Chronicity: progressive breathlessness over years, not episodic attacks
- Productive cough: daily cough with mucoid or purulent sputum; chronic bronchitis definition (≥3 months/year for ≥2 years)
- Exacerbation history: how many hospital admissions in the past year? antibiotic courses required? — this establishes exacerbation frequency, a key prognostic and therapeutic determinant
- Smoking history: must be quantified in pack-years (number of packs/day × number of years smoked; 1 pack = 20 cigarettes)
- Biomass fuel exposure: cooking fuel type, ventilation of cooking area, hours of daily exposure — especially in women
- Occupational history: dusty workplaces, chemical exposures, textile mills, mining
- Exercise tolerance using MRC dyspnoea scale: Grade 1 (only with strenuous exertion) → Grade 5 (too breathless to leave the house)
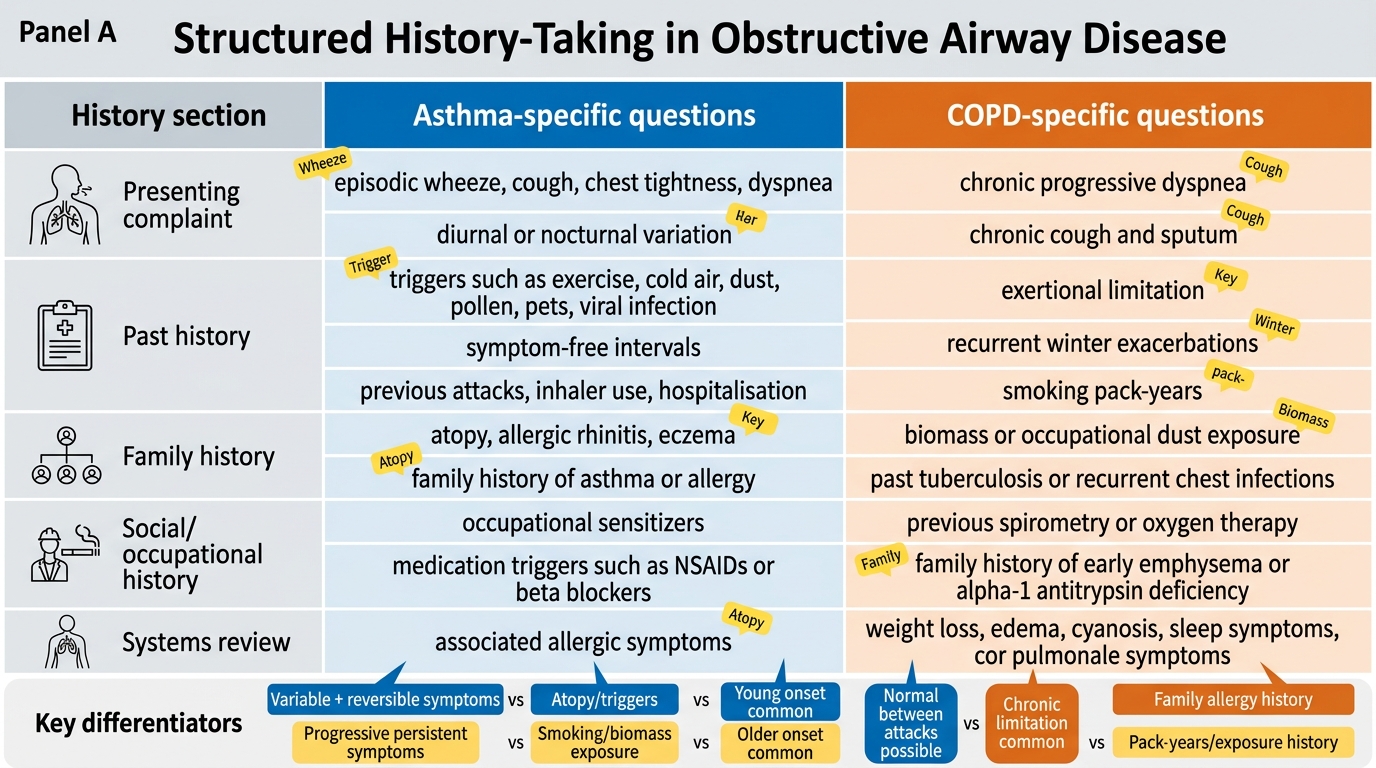
History-Taking Framework for Asthma and COPD
Governing Principles of Respiratory Examination
The governing principles of the respiratory examination in obstructive airway disease are systematic progression through inspection, palpation, percussion, and auscultation; bilateral comparison at each step; and integration of findings into a coherent clinical hypothesis at the end. The examination must achieve several specific objectives simultaneously: confirm the presence and pattern of airway obstruction, assess its severity, identify signs of acute distress or impending respiratory failure, and detect complications or alternative diagnoses (consolidation, effusion, pneumothorax, cardiac failure).
A critical conceptual principle is that examination findings in stable obstructive airway disease may be minimal or absent. Mild asthma between attacks and mild COPD on a good day may have entirely normal auscultation. The examination becomes more informative in moderate-severe disease or during an acute exacerbation. This does not diminish its importance — a normal examination in a symptomatic patient is itself diagnostic information (supporting asthma with full inter-attack recovery, for example) — but it does mean that the examination must be interpreted in context with the history, and that a normal chest auscultation alone does not exclude significant obstructive airway disease.
A second governing principle: always assess the whole patient before the chest. The bedside inspection from the end of the bed — general appearance, posture (forward-leaning orthopnoeic position in severe COPD or asthma), use of accessory muscles, lip pursing, oxygen delivery device in use, presence of nebuliser or spacer — can provide the severity assessment before you pick up your stethoscope. The initial vital signs (respiratory rate, pulse rate, blood pressure, temperature, SpO₂ on pulse oximetry) must be formally measured and recorded as part of the examination for any patient presenting with breathlessness.
The MRC dyspnoea scale should be assigned based on history during the examination encounter:
- Grade 1: breathless only on strenuous exertion
- Grade 2: short of breath when hurrying on level ground or walking up a slight hill
- Grade 3: walks slower than most people of same age on level ground, or stops after 15 minutes walking on own pace
- Grade 4: stops for breath after walking about 100 metres or after a few minutes on level ground
- Grade 5: too breathless to leave the house, or breathless when dressing/undressing
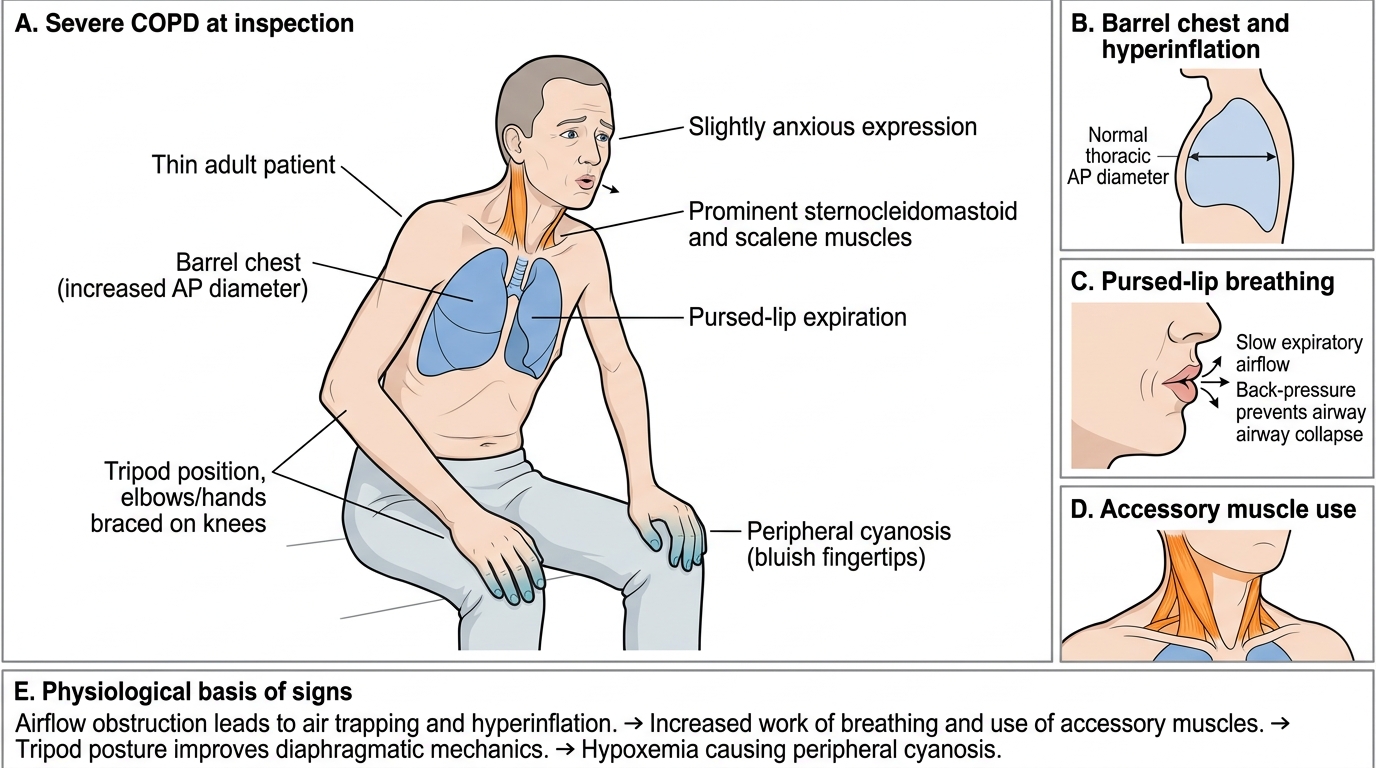
Inspection Signs of Severe COPD
Systematic Examination: Technique and Findings
The systematic respiratory examination proceeds through a reproducible sequence — inspection, palpation, percussion, and auscultation — applied bilaterally and comparatively at each step. In obstructive airway disease, this sequence carries two simultaneous purposes: characterising the nature and severity of the obstruction (is this a moderate exacerbation or near-fatal disease?), and identifying concurrent complications that may alter management completely, such as pneumothorax, consolidation, or pleural effusion. The examination must not be rushed or abbreviated — findings in one zone must be verified in the contralateral zone before moving on, and both anterior and posterior chest surfaces must be examined systematically. Auscultation findings must always be interpreted alongside percussion, since dullness beneath an area of reduced air entry distinguishes effusion from collapse, while hyper-resonance distinguishes pneumothorax from hyperinflation. What follows is a step-by-step description of technique, expected findings in obstructive airway disease, and the specific signs that identify key complications and diagnoses beyond OAD.
Provided image
Inspection (from the end of the bed):
- General appearance: cyanosis (central — blue discolouration of tongue and mucous membranes — indicates significant hypoxaemia; peripheral cyanosis at fingertips may be circulatory); respiratory distress (use of accessory muscles — sternocleidomastoid, scalene — indicates severe obstruction); inability to complete sentences in one breath; orthopnoeic posture (leaning forward, bracing arms on knees — reduces accessory muscle recruitment burden in severe COPD)
- Respiratory rate: count for a full 60 seconds, ideally while appearing to take the pulse to avoid the patient altering their rate. Tachypnoea (>20/min at rest in adults) indicates significant respiratory compromise. In acute asthma, RR >25/min is a marker of moderate-severe attack.
- Chest shape: barrel chest (increased AP diameter, horizontal ribs, prominent costal cartilages) is a sign of severe emphysema with air trapping and hyperinflation; Harrison's sulcus (a permanent groove along the lower costal margin from chronic diaphragm tug in childhood severe asthma)
- Breathing pattern: pursed-lip breathing (COPD patients spontaneously adopt this to apply intrinsic PEEP, keeping small airways open during expiration and improving gas exchange); prolonged expiratory phase
- Finger clubbing: NOT a feature of asthma or uncomplicated COPD — its presence suggests bronchiectasis, lung cancer, mesothelioma, cryptogenic fibrosing alveolitis, or cyanotic heart disease
- Peripheral oedema: ankle oedema in advanced COPD suggests cor pulmonale (right heart failure from pulmonary hypertension)
Tracheal position (palpation):
Place two fingers lightly in the suprasternal notch. A central trachea is normal. Tracheal deviation away from the affected side = large pleural effusion or tension pneumothorax (displacement by space-occupying process). Tracheal deviation toward the affected side = lung collapse or fibrosis. In obstructive airway disease, the trachea is central unless there is a complicating process.
Chest expansion (palpation):
Place hands flat on the lower chest with thumbs meeting in the midline. Instruct deep inspiration and observe thumb movement. Normally, thumbs move symmetrically outward by ≥5 cm. Reduced expansion on both sides in emphysema (hyperinflated, flat diaphragm, reduced tidal volume). Asymmetric reduction suggests ipsilateral consolidation, effusion, or collapse.
Percussion:
- Technique: place the middle finger of the non-dominant hand firmly against the chest wall (acting as a pleximeter); strike the middle phalanx with the tip of the middle finger of the dominant hand (plexor) with a sharp wrist-flick motion. Use the same force and technique at all sites for valid comparison.
- Normal: resonant throughout — a hollow, drum-like note
- Emphysema/hyperinflation: hyper-resonance bilaterally — more resonant than normal, due to air trapping
- Pneumothorax: unilateral hyper-resonance with absent breath sounds
- Consolidation or collapse: dullness — a flat, thud-like note
- Pleural effusion: stony dullness — markedly dull, non-resonant, with a horizontal upper border (shifting on positional change)
- Liver dullness: normally dull in the right lower zone from the 6th intercostal space; in hyperinflated COPD, liver dullness is displaced downward, reflecting pushed-down diaphragm
Auscultation:
- Instruct the patient to breathe through an open mouth, slightly deeper than normal, but not forced
- Systematically compare: upper, mid, lower zones anteriorly; upper, mid, lower zones posteriorly; lateral zones
- Breath sounds in obstructive airway disease: vesicular but with prolonged expiratory phase — in obstruction the expiratory flow is limited, so expiration takes longer (I:E ratio shifts from normal 1:2 toward 1:3 or longer)
- Wheeze (rhonchi): the primary added sound of airway obstruction. Expiratory wheeze from airway narrowing during forced expiration is most common; biphasic wheeze (inspiratory and expiratory) occurs with severe obstruction; polyphonic wheeze (multiple pitches simultaneously) indicates diffuse small-airway narrowing as in asthma; monophonic wheeze (single pitch, localised) suggests a fixed partial obstruction (foreign body, tumour — must not be mistaken for asthma)
- Reduced air entry bilaterally in severe obstruction — in very severe asthma, the wheeze may be absent ("silent chest") because air movement is insufficient to generate sound — a silent chest in a breathless patient is a medical emergency, not a sign of improvement
- Crackles: not typical of uncomplicated asthma or COPD — their presence should raise the possibility of coexisting pneumonia, pulmonary oedema, or bronchiectasis
- Vocal resonance/vocal fremitus: reduced over an effusion, increased over consolidation
Measuring respiratory rate, effort tolerance, and oxygen saturation:
Formal documentation requires: respiratory rate (counted over 60 seconds), oxygen saturation (SpO₂ on pulse oximetry — note if on supplemental oxygen and at what flow rate), and a 6-minute walk test (6MWT) or corridor walk assessment for effort tolerance (measures exercise capacity and desaturation during activity — important for LTOT assessment in COPD).
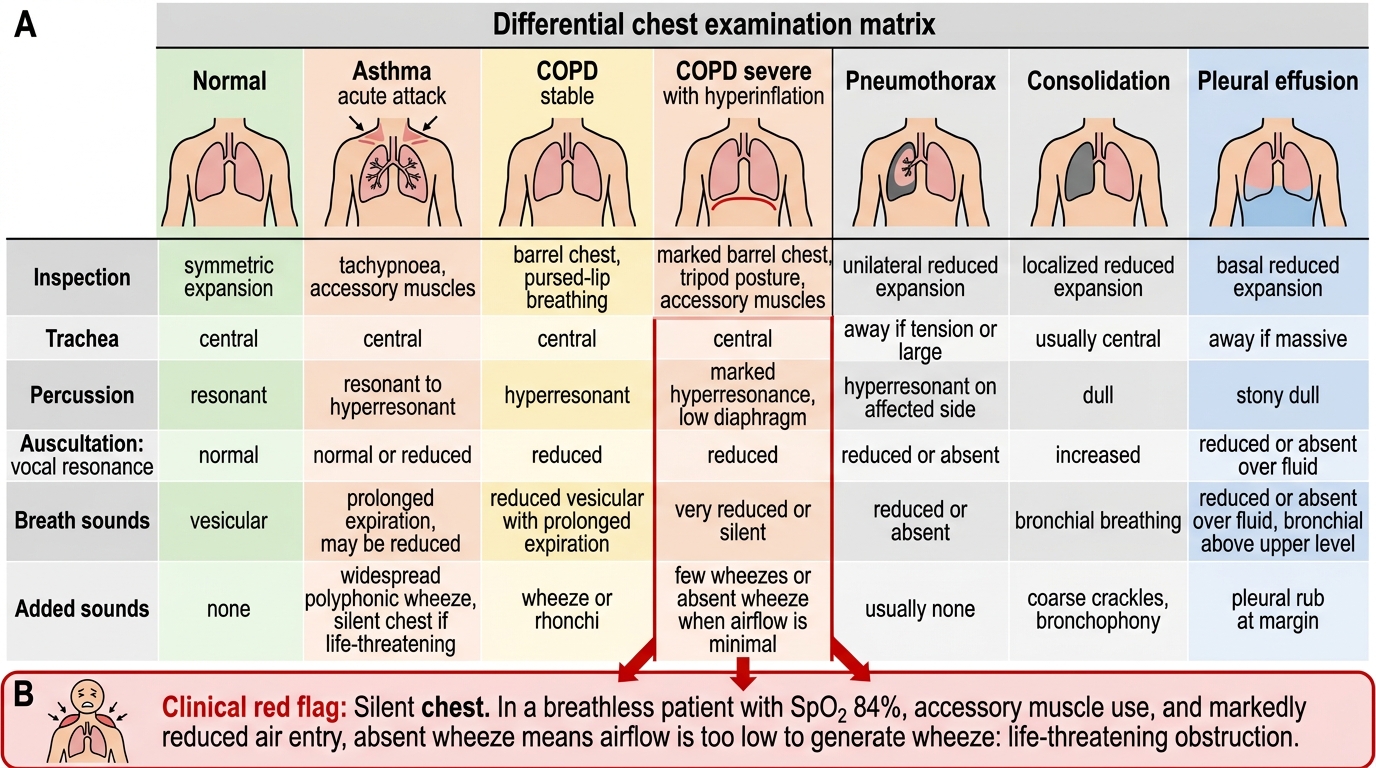
Chest Examination Findings in Obstructive and Pleural Lung Disease
SELF-CHECK
A 68-year-old COPD patient has an acute exacerbation. On examination his RR is 28/min, SpO₂ 84% on room air, he cannot complete sentences, and uses accessory muscles. On auscultation you hear NO wheeze, just dramatically reduced air entry bilaterally. What does the absent wheeze indicate?
A. The patient's obstruction has resolved — no wheeze means no bronchospasm
B. The patient has pneumothorax — absent breath sounds bilaterally
C. Silent chest — air entry is so severely reduced that wheeze cannot be generated; this is a sign of life-threatening obstruction
D. The patient has pulmonary oedema, not COPD — wheeze would be present if this were airway obstruction
Reveal Answer
Answer: C. Silent chest — air entry is so severely reduced that wheeze cannot be generated; this is a sign of life-threatening obstruction
A 'silent chest' in a breathless, distressed patient with accessory muscle use and SpO₂ 84% is a medical emergency. Wheeze requires sufficient airflow velocity through narrowed airways to generate the oscillating sound. When obstruction is so severe that almost no air moves, there is insufficient flow to produce wheeze — the chest becomes 'silent'. This is not improvement; it is impending respiratory arrest. The clinical context (accessory muscle use, tachypnoea, severe hypoxaemia, inability to speak) distinguishes this from pneumothorax (unilateral hyper-resonance, tracheal deviation) or cardiac failure.