Page 3 of 22
IM28.1-7 | Obstructive Airway Disease Foundations — SDL Guide (Part 3)
Principles of Management: A Foundational Overview
Management of obstructive airway disease is built on the recognition that asthma and COPD, while sharing the physiological endpoint of airflow limitation, require fundamentally different therapeutic strategies — one aimed at restoring normal airway function episodically and maintaining long-term control, the other aimed at slowing an inexorable but modifiable decline. Understanding the broad management principles at a foundational level establishes the conceptual scaffolding on which detailed pharmacological and procedural knowledge is built in subsequent modules. Three principles apply universally to both diseases: (1) identify and eliminate or reduce the causative or precipitating exposure; (2) achieve and maintain the best attainable lung function with the least medication burden; and (3) prevent exacerbations and their complications, since each exacerbation drives accelerated lung function loss and increased mortality.
Provided image
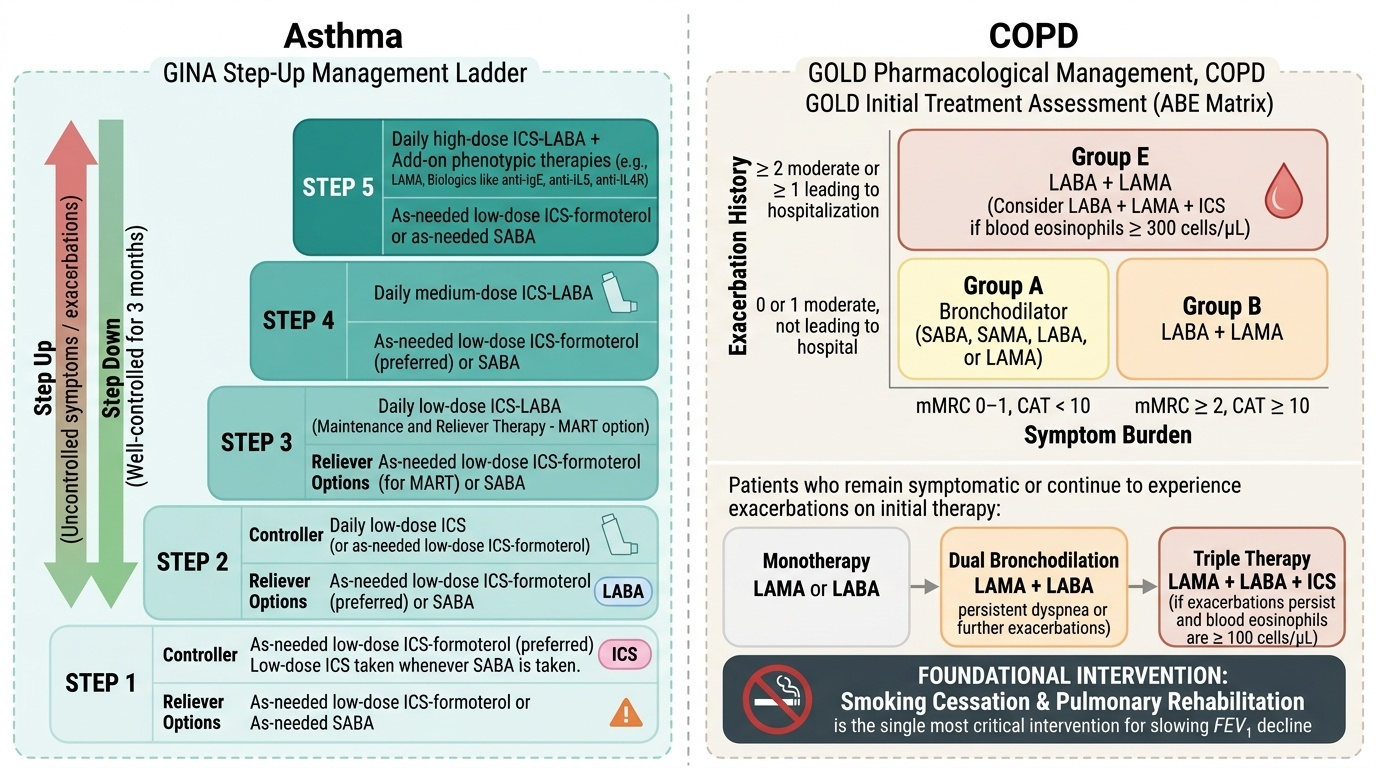
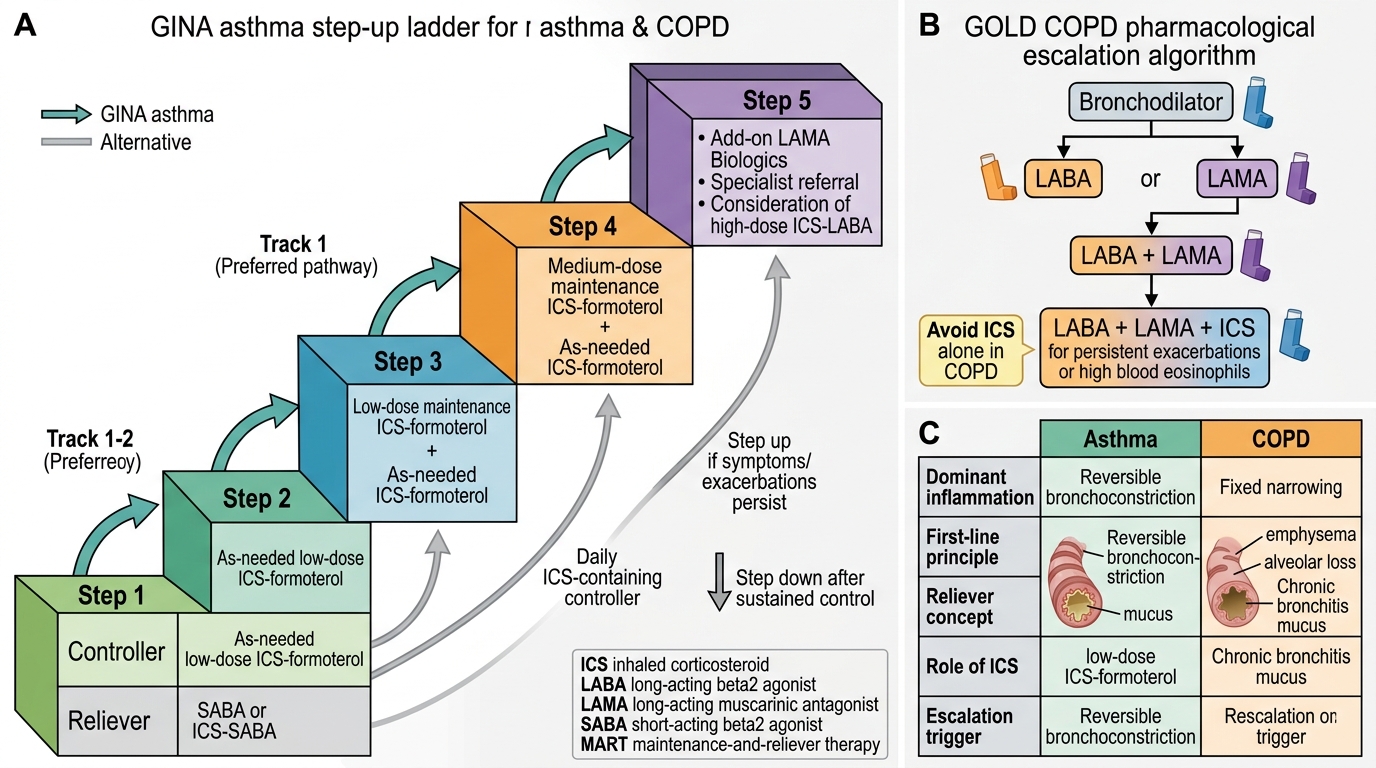
For asthma, the management framework is the GINA step-up/step-down approach based on symptom control. The backbone of stable asthma management is inhaled corticosteroids (ICS) — which address the underlying eosinophilic airway inflammation rather than just relieving bronchospasm. Short-acting beta₂-agonists (SABA) — primarily salbutamol — remain the reliever of choice for acute symptoms, though GINA 2023 has moved SABA-only relief out of first-line position, advocating instead ICS-formoterol as the preferred reliever for most patients to ensure anti-inflammatory coverage at every reliever use. Trigger avoidance is non-pharmacological but often the highest-yield intervention — house dust mite mitigation, smoking cessation, avoidance of aspirin/NSAIDs in AERD. Acute exacerbations are managed with high-dose SABA, systemic corticosteroids, and controlled oxygen, with early recognition of the need for escalation to hospital or intensive care.
For COPD, smoking cessation is the single most important intervention — it is the only measure proven to slow the rate of FEV1 decline and alter disease trajectory. Pharmacological therapy provides symptomatic benefit (reduced dyspnoea, improved exercise tolerance, reduced exacerbations) but does not reverse or halt lung function decline. The pharmacological backbone of stable COPD is long-acting bronchodilators — long-acting beta₂-agonists (LABA) such as salmeterol or indacaterol, and long-acting muscarinic antagonists (LAMA) such as tiotropium or glycopyrronium. Combined LABA/LAMA inhalers are now preferred over either alone for most symptomatic patients. ICS is added in patients with frequent exacerbations, elevated blood eosinophils, or features of asthma-COPD overlap. Long-term oxygen therapy (LTOT) — ≥15 hours per day — is indicated in patients with resting PaO₂ ≤55 mmHg (or ≤60 mmHg with cor pulmonale or polycythaemia) and is the only pharmacological intervention proven to improve survival in severe COPD. Pulmonary rehabilitation significantly improves dyspnoea and quality of life. Vaccinations — influenza (annual) and pneumococcal — reduce the risk of infective exacerbations.
Acute exacerbations of COPD (AECOPD) are managed with controlled oxygen (SpO₂ 88–92%), short-acting bronchodilators (salbutamol + ipratropium nebulised), systemic corticosteroids (prednisolone 30–40 mg/day × 5 days), antibiotics when there is clinical evidence of bacterial infection (purulent sputum, positive Anthonisen criteria), and non-invasive ventilation (NIV) for acute hypercapnic respiratory failure (pH < 7.35, PaCO₂ elevated — first-line over invasive mechanical ventilation for COPD exacerbations where NIV is appropriate).
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Asthma and COPD Pharmacological Step-Up Management
Self-Assessment: Integrating OAD Foundations
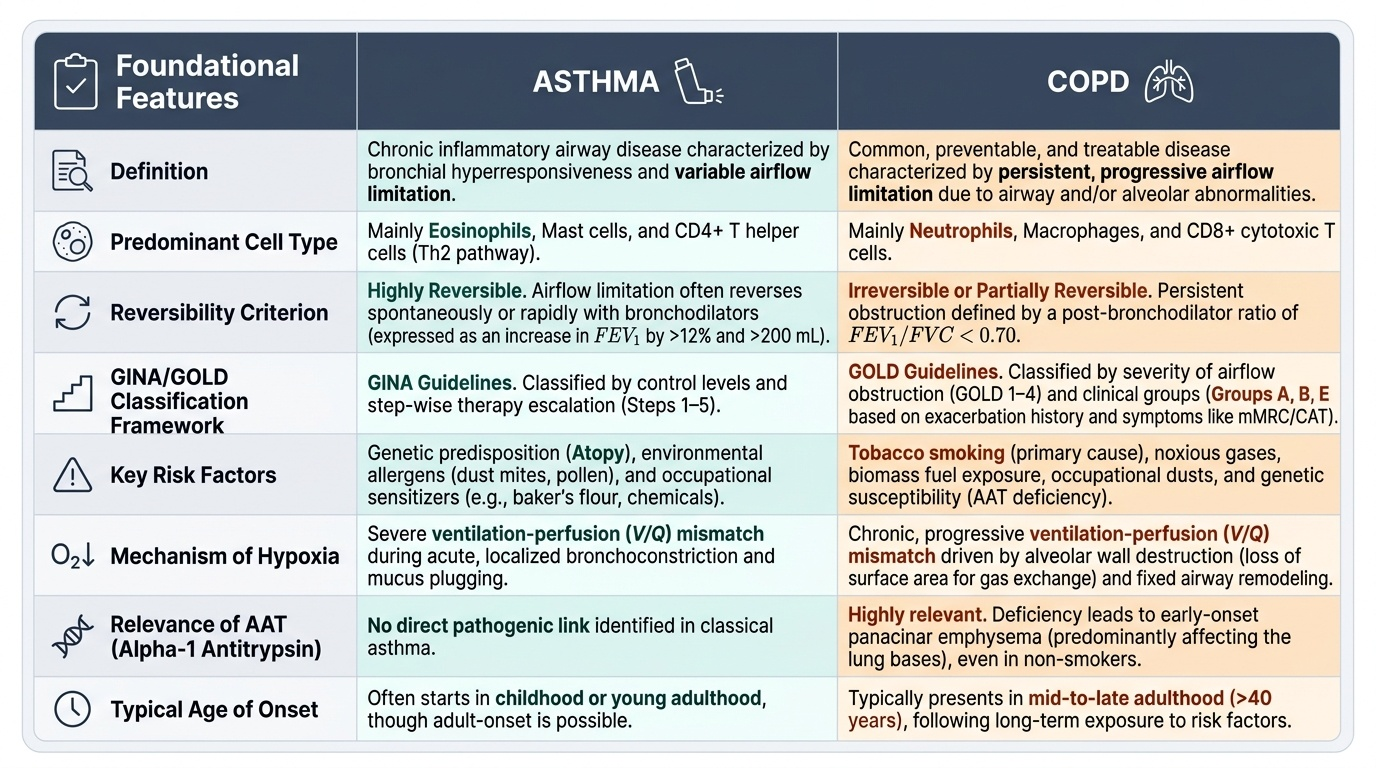
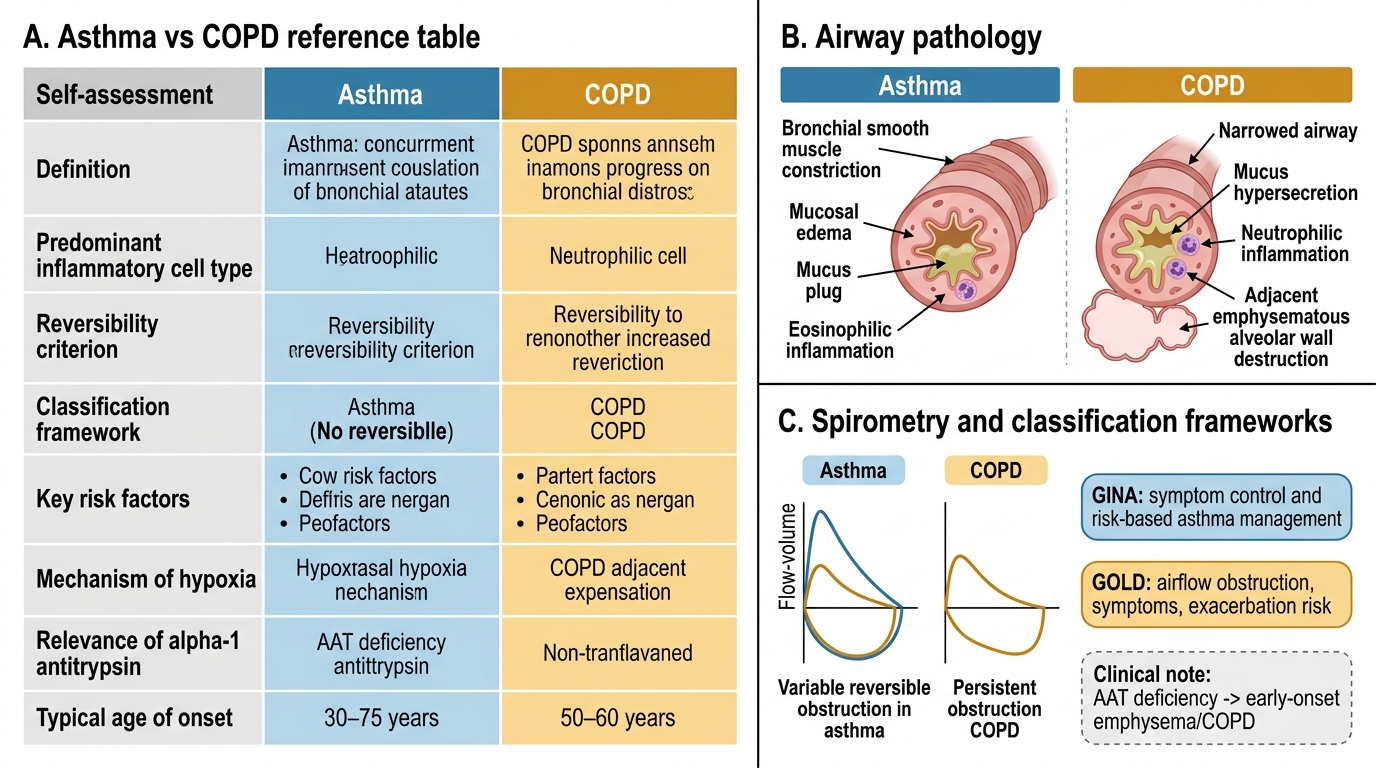
You have now covered the complete foundational framework for obstructive airway disease — the definitions and GINA/GOLD classification systems, the global and Indian epidemiological burden, the multi-factorial risk factors, the mechanisms of acute exacerbation, the pathophysiology of hypoxia and hypercapnia with their implications for oxygen therapy, the genetics of alpha-1 antitrypsin deficiency, and the range of allergic and non-allergic environmental triggers. Use the scenarios below to test your ability to apply these concepts in an integrated manner — the skill that NMC competencies IM28.1–28.7 demand.
Provided image
Scenario A: A 45-year-old female non-smoker with no occupational dust exposure presents with dyspnoea on exertion and recurrent respiratory infections since her 30s. Spirometry shows an obstructive pattern with FEV1 52% predicted. CT chest shows predominantly basal emphysema. What single investigation is most important to establish the aetiology of her emphysema?
Analysis: Emphysema at age 45 in a non-smoker, with basal predominance and early onset — this is the classical presentation of alpha-1 antitrypsin (AAT) deficiency. Panacinar emphysema (as opposed to centri-acinar in tobacco-COPD) predominantly affects the lung bases. The investigation is serum AAT level followed by phenotyping (PiZZ). Augmentation therapy and intensive smoking-cessation (even secondary smoke) advice are relevant once diagnosed.
Scenario B: A 30-year-old baker presents to the occupational health clinic with chest tightness and wheeze that are consistently worse on working days and resolve over weekends. He has no atopy. Spirometry is normal on the day of testing (a Monday morning, after a 2-day break). What is the likely diagnosis and what investigation would confirm it?
Analysis: The work-related pattern (worse on working days, better on weekends) is the cardinal feature of occupational asthma. Flour dust is a well-recognised sensitising agent. Normal spirometry at rest does not exclude it — peak flow monitoring (serial PEFR measurements at work and at home over 2–4 weeks) and specific bronchial provocation challenge with the suspected allergen (wheat flour extract) would confirm the diagnosis. Management requires workplace modification or relocation.
Scenario C: An elderly COPD patient on 4 L/min nasal cannula oxygen in hospital becomes increasingly drowsy over 2 hours. His earlier SpO₂ was 78%; it is now 97%. ABG shows PaCO₂ 85 mmHg and pH 7.25. What is the error and what should be done?
Analysis: This is CO₂ narcosis from uncontrolled high-flow oxygen in a chronic CO₂ retainer whose hypoxic drive has been abolished by raising the SpO₂ too high. In a known chronic CO₂ retainer, the safe SpO₂ target is 88–92% — not 97%. The oxygen should be reduced to a controlled FiO₂ (24–28% via Venturi mask) to maintain SpO₂ at 88–92%, and NIV (non-invasive ventilation) should be initiated urgently to correct the acute hypercapnic respiratory failure.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
Asthma vs COPD: Foundational Features