Page 5 of 20
IM29.{8-10,12-14,21,25} | Professional Conduct and Documentation — SDL Guide (Part 2)
Risk Management and Medical Error Reduction: A Systems Approach
Risk management (IM29.21) in healthcare is the systematic identification, assessment, and mitigation of conditions that could lead to patient harm. The foundational conceptual shift in patient safety thinking — from individual blame to systems analysis — was crystallised in the landmark 1999 report 'To Err is Human' from the US Institute of Medicine, which estimated that up to 98,000 patients died annually in US hospitals from preventable medical errors, and argued that the majority of these errors were system failures, not individual failures. This insight transformed medical error reduction from a disciplinary exercise into an engineering and quality improvement discipline.
The Swiss Cheese Model developed by James Reason provides the most widely used framework for understanding how medical errors reach patients. In this model, safety systems are represented as slices of Swiss cheese, each with holes (vulnerabilities). A single layer rarely has a hole in exactly the right place to allow an error through. But when multiple layers are misaligned — when the medication check fails at the same moment the nurse is distracted and the patient has not been educated about their drugs — the holes align and a harm event occurs. The implication for clinical practice is that individual vigilance is necessary but not sufficient: the goal is to add layers (checklists, double-checks, standardised protocols, read-backs) so that no single failure propagates to the patient.
The categories of medical error most relevant to the final-year student in medicine include:
- Medication errors: prescribing errors (wrong drug, dose, route, or indication), dispensing errors (pharmacy-level), and administration errors (wrong patient, wrong time). India's adoption of generic prescribing under the Jan Aushadhi Scheme and NMC prescribing guidelines reduces one class of error (trade-name confusion) but creates another (generic name look-alike/sound-alike confusion — e.g. metformin vs metronidazole). High-alert medications — anticoagulants (heparin, warfarin, low-molecular-weight heparin), insulin, concentrated electrolytes (KCl concentrate), and opioids — require double-checking protocols and clear documentation of indication and monitoring plan.
- Diagnostic errors: premature closure (stopping at the first plausible diagnosis before ruling out serious alternatives), anchoring bias (over-weighting the initial impression), and failure to follow up investigation results.
- Procedure errors: wrong-site procedures, inadequate consent, inadequate aseptic technique.
- Communication failures: incomplete handover, failure to communicate critical laboratory values, illegible prescriptions.
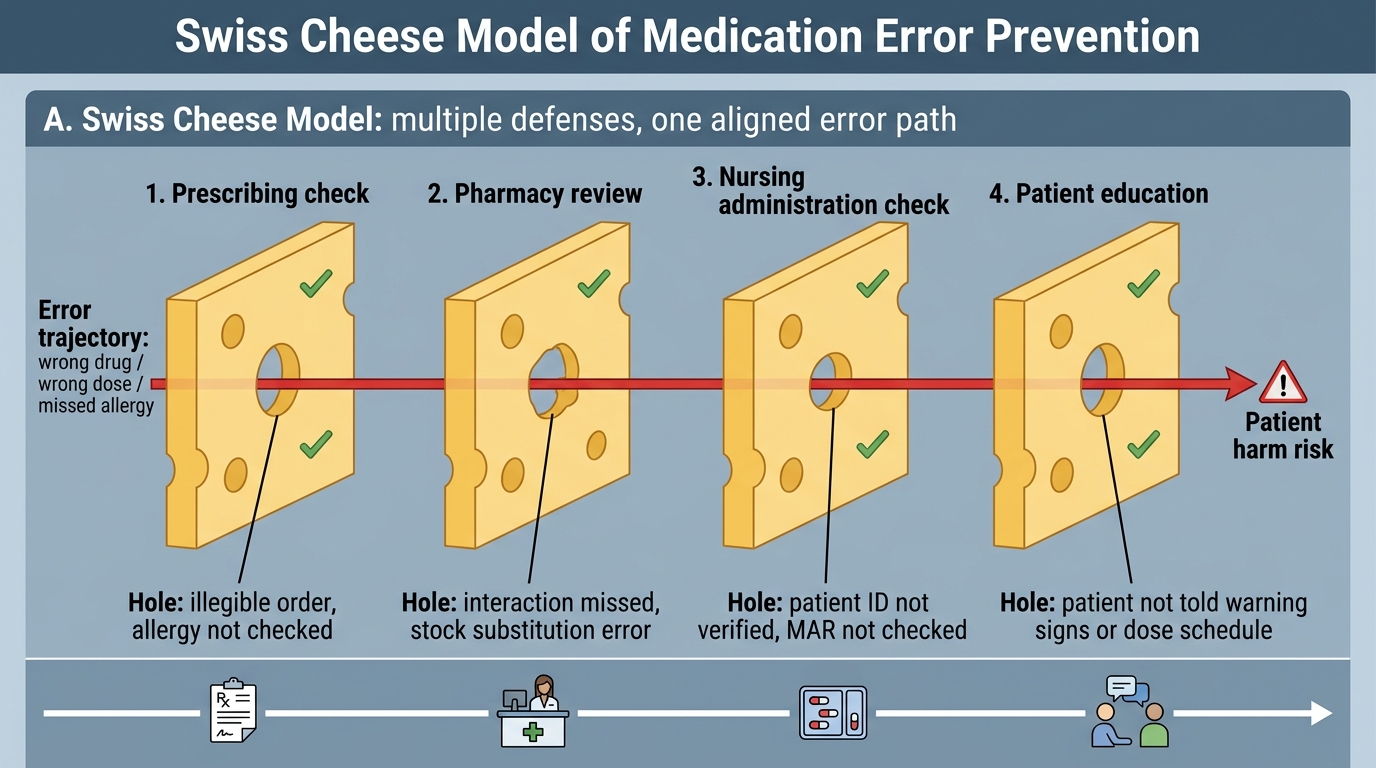
Swiss Cheese Model of Medication Error Prevention
Key error reduction practices for the clinical student and junior doctor:
| Practice | Error type addressed | Evidence base |
|---|---|---|
| SBAR handover | Communication failure | WHO Patient Safety Curriculum 2011 |
| Medication reconciliation on admission | Prescribing/omission error | NABH standards |
| Two-patient identifiers before procedure | Wrong-patient error | Joint Commission/NABH |
| Pre-procedure checklist (surgical safety checklist adapted) | Wrong-site, inadequate consent | Haynes et al., NEJM 2009 |
| Read-back for verbal medication orders | Verbal order error | NMC/NABH |
| Incident reporting without blame | Latent system failures | WHO; Indian NHM patient safety framework |
The culture of open disclosure and incident reporting is the most difficult systemic change to operationalise in Indian healthcare, where a blame-and-shame response to errors remains common. NABH standards (National Accreditation Board for Hospitals) require that all hospitals maintain an incident reporting system and that adverse events be reviewed through root cause analysis (RCA) rather than individual punishment alone. The final-year student's role is to understand this culture, to report errors and near-misses through the available channel, and not to participate in concealment — which, as the Bolam principle and subsequent Indian case law have established, can amplify legal liability for all involved.
The three elements of medical negligence as consistently applied by Indian courts (based on Jacob Mathew v State of Punjab, 2005 Supreme Court ruling) are: (1) a duty of care existed between the physician and patient; (2) that duty was breached — the physician's conduct fell below the standard of the ordinary skilled practitioner in that specialty (Bolam test as modified by Indian jurisprudence); and (3) the breach caused the patient's harm. Documentation deficiencies do not by themselves constitute negligence — but they create an evidentiary vacuum in which a claim of negligence becomes extremely difficult to refute.
SELF-CHECK
During a busy evening shift, a senior resident asks you verbally to prescribe 'the usual dose of KCl for this hypokalaemic patient' and moves on. You administer 40 mmol KCl by IV push without dilution, which causes a cardiac arrest. Which risk management principle, if applied, would have been most likely to prevent this adverse event?
A. Incident reporting after the event to prevent recurrence
B. Verbal medication orders for high-alert medications should be confirmed in writing or by read-back before administration, and concentrated KCl should never be given undiluted IV push
C. Grooming standards — a properly identified doctor would have been consulted
D. The SBAR handover at the shift change should have flagged the hypokalaemia
Reveal Answer
Answer: B. Verbal medication orders for high-alert medications should be confirmed in writing or by read-back before administration, and concentrated KCl should never be given undiluted IV push
Concentrated potassium chloride (KCl) is a high-alert medication — it is on virtually all high-alert medication lists because undiluted IV push KCl is invariably fatal (causes cardiac arrest by hyperkalemia-induced VF/asystole). The 'usual dose' verbal order without specifying concentration, route, and rate is an incomplete and dangerous order. The risk management principles that would have prevented this: (1) never administer a verbal order for a high-alert medication without written confirmation or authorised read-back; (2) KCl must always be diluted (maximum 40 mmol in 500 mL or 1000 mL, administered at a rate ≤20 mmol/hour via infusion pump); (3) concentrated KCl solutions should not be stored in clinical areas at all — NABH and WHO guidelines recommend removing them from ward stock. Incident reporting (option A) is important but corrective, not preventive for this event. SBAR (option D) is relevant to handover but not to this specific error mechanism.
SELF-CHECK
You are a final-year student on the evening ward round. You observe that a consultant has documented an examination finding in the case record that you are fairly certain was not performed — the patient was never turned for a rectal examination that is now recorded as 'normal DRE.' What is the most professionally appropriate response?
A. Say nothing — the consultant is senior and you may have misremembered the round
B. Immediately report to the hospital administration
C. Document your own observation in a separate note and speak privately to the registrar or senior registrar to raise your concern
D. Cross out the consultant's entry and initial it with 'not performed'
Reveal Answer
Answer: C. Document your own observation in a separate note and speak privately to the registrar or senior registrar to raise your concern
The ethical obligations here involve both non-maleficence (a falsely documented examination may mislead future clinicians) and professional responsibility. Saying nothing (option A) normalises falsification of records, which constitutes fraud and can cause patient harm. Immediately escalating to administration (option B) bypasses appropriate professional channels. Crossing out the consultant's entry yourself (option D) alters a medical record — itself a serious offence. The appropriate action is to document your own observations factually (what you observed on the round) and raise the concern through the proper professional channel — the registrar or supervisor above the consultant — in a private, non-confrontational way. If the concern is not addressed through that channel, it may be escalated to the head of the department or the institution's patient safety officer. The NMC Act 2020 protects 'whistleblowers' in good faith professional misconduct concerns; it does not require students to remain silent about potential patient safety risks.
Self-Assessment: Professional Conduct Scenarios
You have now covered the foundations of professional conduct — documentation standards, teamwork, privacy, confidentiality, risk management, altruism, and professional presence. The self-assessment below applies these through scenario-based reasoning that replicates the OSCE-style evaluation used in final-year examinations for IM29 competencies.
For each scenario, identify which competency (IM29.8–IM29.25) is being tested, describe the correct professional response, and explain the reasoning — including the ethical principle and relevant regulatory framework where applicable.
Scenario A — Documentation under pressure:
It is 11 PM at the end of a 12-hour shift. You have 14 patients to hand over and eight case notes still to write. A colleague offers to write three of the notes for you since they were on the ward all day. You know this is technically incorrect but you are exhausted. What are the professional obligations here, and what is the risk?
Analysis: This tests IM29.13 (documentation) and IM29.12 (responsibility and work ethics). The professional obligation is that the clinician who performed the assessment and made the clinical decision must author that note — or at minimum review, correct, and countersign a note written under their guidance. A colleague writing notes for patients they did not assess is a misrepresentation of the record, which may constitute fraud and creates a false medico-legal document. The risk is that the note may not accurately reflect what was found or decided, creating both patient safety risk and legal liability. The correct approach: triage — write the most complex or high-risk patient notes yourself first; have a colleague write skeleton notes for stable patients under your immediate supervision and review-and-countersign each one before handing over.
Scenario B — Confidentiality in the digital age:
A colleague photographs a rare skin finding on a patient's foot for a teaching case presentation. The patient's face is not in the photograph. He sends the image to the departmental WhatsApp group with the patient's age and diagnosis. Has confidentiality been breached, and what should have been done instead?
Analysis: This tests IM29.10 (confidentiality) and IM29.9 (privacy). Confidentiality has been breached — not because the face is visible, but because the combination of clinical details (age, diagnosis, unusual finding) may be sufficient to identify the patient in a small community or institutional setting, and no consent was obtained for photographic documentation or digital distribution. The DPDPA 2023 classifies health data as sensitive personal data; transmission via unsecured WhatsApp is a violation regardless of whether the face is visible. The correct procedure: obtain explicit written consent for clinical photography; use a de-identified, institution-approved channel for teaching case sharing; store on the institution's clinical teaching database rather than personal devices or open group chats.
Scenario C — Altruism and the limits of professional duty:
A patient with chronic obstructive pulmonary disease is readmitted for the fourth time this year in exacerbation. He is socially isolated, homeless, and unable to afford his inhalers. Your hospital social worker is unavailable and the patient will likely be re-admitted within weeks after discharge. Extending his admission beyond clinical necessity is not justifiable. What does altruism (IM29.25) require of you here, within the system constraints you face?
Analysis: Altruism does not require the physician to provide unlimited personal resources or to circumvent institutional systems. It requires active advocacy within those systems: initiating a formal social work referral even if the current social worker is unavailable (ensuring the referral is documented and followed up); identifying whether the patient qualifies for Ayushman Bharat PM-JAY or any state scheme covering inhaler costs; documenting the social determinants in the discharge summary so that the next clinician understands the complete picture; and connecting the patient with a community health worker or NGO if one is available through the district health system. Altruism, in the context of a resource-constrained public hospital, is operationalised as systematic advocacy and documentation of unmet social need — not heroic individual action.
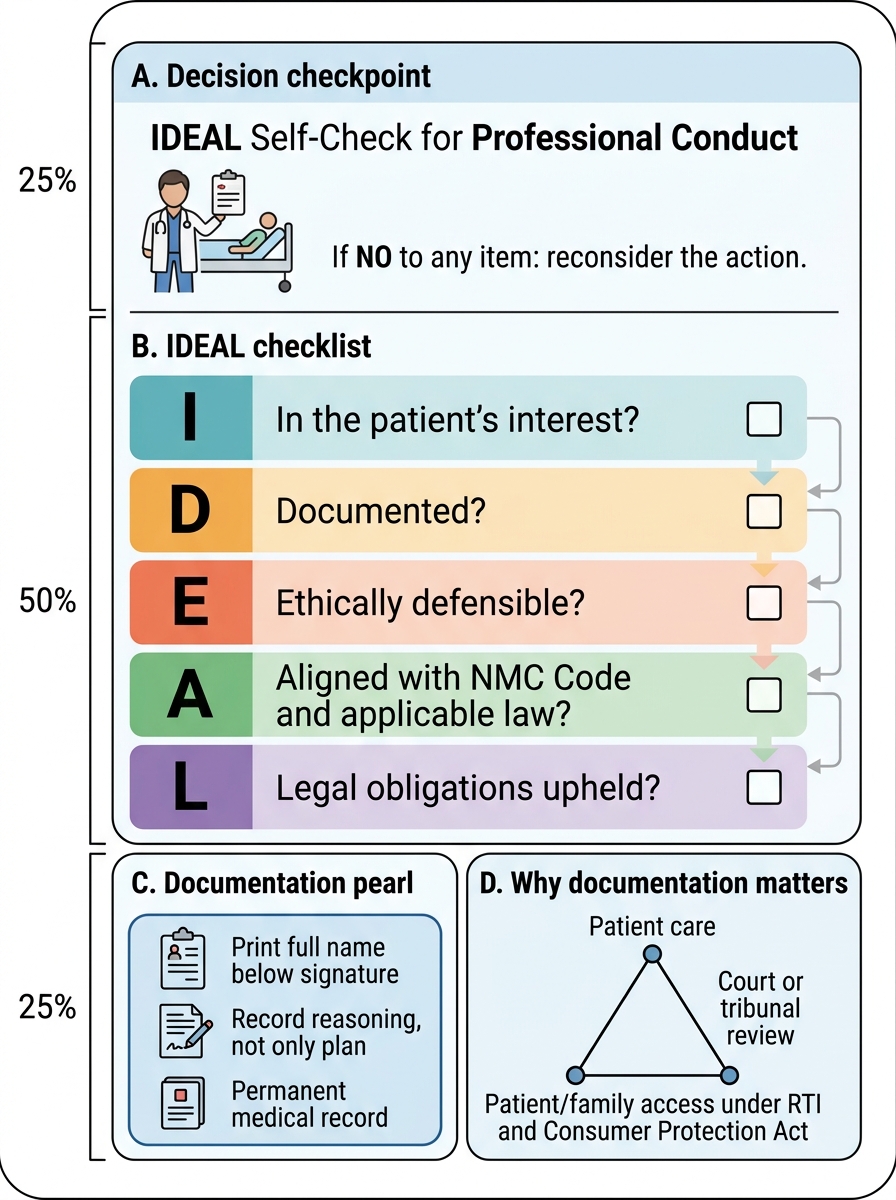
IDEAL Self-Check for Professional Conduct
A useful self-check framework for professional conduct decisions is IDEAL: Is this action In the patient's interest? Is it Documented? Is it Ethically defensible? Is it Aligned with the NMC Code and applicable law? Does it uphold my Legal obligations? If 'no' to any of these, the action requires reconsideration.
CLINICAL PEARL
Documentation is not a bureaucratic chore — it is a clinical act. Every line you write in a case note becomes a permanent part of the patient's medical record, available to every clinician who subsequently treats that patient, to any court or disciplinary tribunal that reviews that care, and — under the Right to Information Act and Consumer Protection Act — potentially to the patient or their family. The two most common documentation errors among junior doctors in India are:
- Illegible signatures without name identification — legally worthless and clinically dangerous; always print your full name below your signature.
- Documenting the plan but not the reasoning — write why you are doing what you are doing, especially when you deviate from a standard protocol. 'Decision to hold antibiotics — clinical picture consistent with viral URTI, no criteria met for bacterial infection per clinical scoring' is infinitely more defensible than 'IV antibiotics deferred.'
A second pearl on altruism in practice: the most altruistic thing you can do for a patient is often the least glamorous — ensuring their discharge summary is sent to their primary care physician, ensuring their follow-up appointment is actually booked, and taking five extra minutes to ensure they understand their discharge medication. Altruism is not dramatic; it is systematic.