Page 10 of 20
IM29.{16-20,22} | Professional Limits Priorities and Networks — SDL Guide
Learning Objectives
- Demonstrate awareness of clinical and competency limits and seek appropriate help and consultations (IM29.16)
- Apply strategies to balance personal and professional priorities without compromising patient care (IM29.17)
- Demonstrate effective time management in a clinical environment (IM29.18)
- Form and function within appropriate professional networks including specialist referral, peer communities, and inter-professional teams (IM29.19)
- Identify pathways for career advancement in Indian medicine and demonstrate pursuit of professional development (IM29.20)
- Demonstrate ability to work in a mentoring relationship with junior colleagues (IM29.22)
INSTRUCTIONS
Professional sustainability — the ability to function effectively over a full career — requires knowing your limits, managing your time, building networks, and caring for junior colleagues. These are not soft skills; they are the structural competencies that determine whether the medicine you practise remains safe, the patients you care for remain well-served, and the colleagues you work with develop into the clinicians they are capable of becoming.
References
- NMC Code of Professional Conduct, Etiquette and Ethics Regulations 2002 (amended 2023) (guideline)
- Harrison's Principles of Internal Medicine, 21st ed., Chapter 4 — Ethical Issues in Clinical Medicine (textbook)
- API Textbook of Medicine, 10th ed. — Professional Development in Medicine (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr. Meera is in her second year of postgraduate internal medicine training. She has been on call for 36 hours. She has not eaten since the previous morning. She is managing 22 patients, four of whom are critically unwell. At 4 AM she is asked to do a lumbar puncture on a febrile patient with suspected meningitis. She has performed five lumbar punctures under supervision; she has never done one independently. She reaches for the tray and starts to position the patient. She does not call her senior registrar. She does not tell the patient she is performing the procedure for the first time alone. The procedure goes badly. Later, in the debrief, she says: 'I didn't want to bother anyone. I didn't want to look like I couldn't cope.' There are three professional failures in this scenario — a failure to recognise personal limits, a failure to seek appropriate help, and a failure of supervision. Each one of them was preventable. This module is about the professional skills that would have prevented them.
WHY THIS MATTERS
The NMC 2024 curriculum places the competencies of IM29.16–IM29.22 — limits, priorities, time management, networks, career advancement, and mentoring — at the SH (Skill/Habit) level for final-year students. This means the examination assesses whether you can demonstrate these behaviours in practice, not merely describe them. The professional relevance extends beyond examinations: burnout rates in Indian junior doctors are among the highest globally, with a 2021 study in the Indian Journal of Medical Ethics reporting burnout in over 60% of residents in tertiary care settings — driven precisely by the inability to manage limits, set priorities, and access support networks. A physician who enters practice without these professional competencies is at risk not only of harming patients but of self-harm through professional burnout, moral injury, and career attrition. These competencies are therefore simultaneously about patient safety, professional wellbeing, and the sustainability of the healthcare system.
RECALL
Before proceeding, activate your prior knowledge. From your ethics modules, recall the principle of beneficence — the duty to act in the patient's best interest. Think about what it means when a clinician, through exhaustion or pride, provides substandard care by trying to do something beyond their current competence. From your community medicine and public health training, recall the concept of human resources for health — the recognition that doctors and nurses are themselves resources that can be depleted, burned out, and lost from the system if they are not sustained. From your clinical rotations, think about the doctors you have admired most — the ones patients trust and juniors want to emulate. Now think about what professional habits made them effective: were they the ones who tried to do everything alone, or the ones who knew when to ask, who to refer, and how to use their team? The professional skills in this module are the architecture of that effectiveness.
Recognising and Acting on Clinical Limits
Awareness of limitations (IM29.16) is one of the most professionally demanding competencies in the NMC curriculum because it requires a combination of accurate self-assessment, intellectual humility, and the willingness to seek help in a professional culture that frequently equates asking for assistance with incompetence. The evidence from patient safety research unequivocally supports the opposite view: seeking help at the limit of competence is the behaviour of a safe, trustworthy clinician; proceeding beyond competence without consultation is a leading mechanism of preventable adverse events.
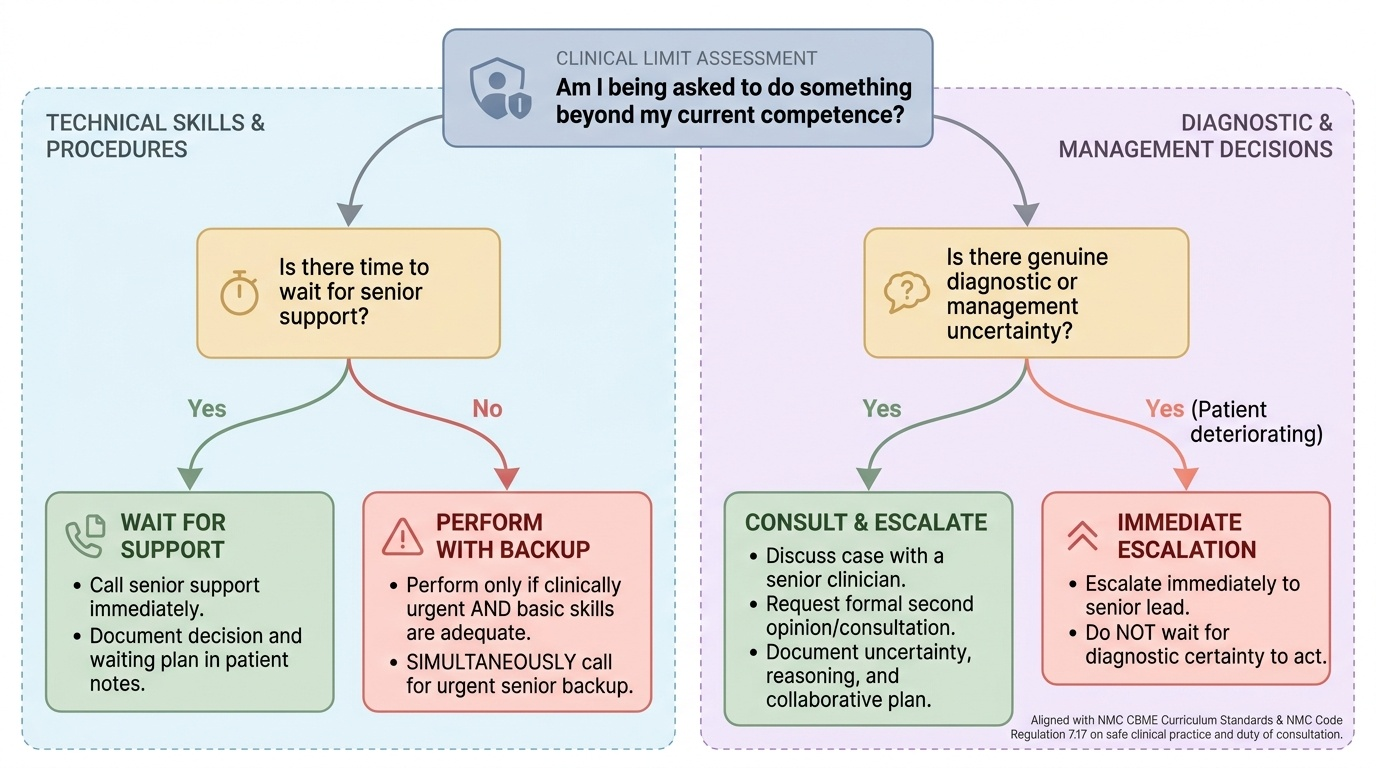
Provided image
The concept of clinical limits operates at several levels. At the level of technical skill, every procedure has a defined competency threshold — a minimum number of supervised performances, a specific set of anatomical conditions required, and a safety standard for independent practice. The NMC CBME curriculum specifies competency levels (Observe, Assist, Perform under supervision, Perform independently) for all clinical skills. Performing a procedure at a lower competency level without supervision, under the pressure of clinical necessity or professional pride, is a patient safety risk. The correct action when confronted with a procedure at the edge of your competence is: perform if clinically urgent and you have adequate basic skill, simultaneously calling for senior backup; do not perform if there is time to wait for more experienced support and the risk to the patient from the procedure is material.
At the level of diagnostic and management uncertainty, every clinician — from medical student to senior consultant — encounters situations in which the correct diagnosis or the optimal management plan is genuinely uncertain. Recognising this uncertainty — rather than projecting false confidence — is the hallmark of the safe, reflective clinician. The NMC Code (Regulation 7.17) explicitly states that the physician should seek a consultation or second opinion when the case is beyond their competence, and that the duty of consultation overrides any financial or institutional pressure to manage the case independently. In practice, this means: when in doubt, ask; when asked, be honest about the degree of your uncertainty; when uncertain about a diagnosis in a patient who is deteriorating, escalate rather than wait for certainty to arrive.
At the level of personal functioning, limits include the recognition that severe fatigue, emotional distress, physical illness, or substance use impairs clinical performance. The physician who operates in these states without acknowledging the impairment and seeking relief is not only putting patients at risk but is also breaching the professional duty of self-care that the NMC Code requires. The management of an impaired physician — whether the impairment is in a peer, a junior colleague, or yourself — is addressed in detail in the companion SDL on impaired physicians (IM29.24).
Balancing Personal and Professional Priorities and Managing Time
Balancing personal and professional priorities (IM29.17) and time management (IM29.18) are inseparable competencies that address the operational reality of clinical practice: the demand for physician time is always greater than the supply, and a physician who does not actively manage this mismatch will either provide inadequate care, burn out, or both. The evidence is clear — physician burnout leads to increased rates of medical errors, decreased patient satisfaction, higher rates of patient abandonment, and earlier career exit. A study in the Lancet (2019) found that physicians with higher burnout scores had odds ratios of 2.2–2.9 for medical errors compared with low-burnout peers. The clinical imperative for personal sustainability is therefore inseparable from the imperative for patient safety.
Time management in clinical medicine is not the same as efficiency in completing tasks — it is the discipline of allocating finite clinical time to activities in proportion to their clinical urgency and importance. The Eisenhower Matrix, adapted for clinical settings, provides a useful framework: tasks fall into four quadrants based on urgency and importance — high urgency/high importance (attend to immediately: a patient in cardiac arrest, a critically deteriorating ward patient, a consent conversation before an urgent procedure); low urgency/high importance (schedule deliberately: CME, reflective practice, research, supervision of juniors, documentation review); high urgency/low importance (delegate where possible: routine paperwork, administrative tasks, non-urgent prescription refills); and low urgency/low importance (minimise or eliminate: unnecessary meetings, redundant administrative processes).
The specific time management challenge for junior doctors in the Indian healthcare context is task overload in an unstructured environment — the morning round generates 20 tasks for the intern that have no prioritisation signal. The professional response is to triage at the start of each clinical period: identify the two or three most clinically urgent tasks (the most unwell patients, the investigations with time-sensitive results, the consents that must precede planned procedures), complete these first, and then work through the remaining tasks in order of clinical urgency. Tasks that cannot be completed within the shift must be handed over explicitly via SBAR — not left with a verbal 'the notes are on the desk' that no one reads.
Balancing personal priorities requires the recognition that the physician is a person with valid personal needs — for rest, nutrition, family relationships, physical health, and emotional support — and that neglecting these needs in the service of clinical work is not heroism but professional unsustainability. The World Medical Association and NMC guidelines both acknowledge that working conditions that systematically prevent physicians from meeting their basic personal needs constitute a professional and ethical problem for healthcare institutions, not merely for individual clinicians. At the individual level, the practical behaviours that operationalise this balance include: asserting a right to handover at the agreed end of a shift (within the limits of clinical safety); using leave entitlements; accessing institutional employee assistance or occupational health services when personal distress is affecting clinical function; and being willing to discuss workload concerns with supervisors before they become crises.
A practical daily time management structure for a junior doctor on a busy inpatient ward:
| Time | Activity |
|---|---|
| Before morning round | Review overnight events, urgent bloods, investigate results for own patients |
| Morning round | Active participation; write tasks in priority order as they are generated |
| Post-round (first 90 min) | Complete the two most urgent tasks for each critically ill patient |
| Midday | Briefly triage remaining task list; identify and delegate low-urgency tasks |
| Before shift end | Complete documentation; write SBAR handover for incomplete tasks |
| Transition to next team | Verbal + written SBAR handover; confirm critical investigations are flagged |
SELF-CHECK
As an intern on a 22-patient general medicine ward, you are asked to do the following at 9 AM after the morning round: (1) prescribe paracetamol for a patient with mild headache; (2) review urgent post-dialysis potassium result for a patient with CKD Stage 5; (3) complete paperwork for discharge of a clinically stable patient; (4) write up the history of a new admission from last night. According to clinical prioritisation principles, what is the MOST appropriate order?
A. 1, 2, 3, 4 — in the order received
B. 2, 4, 1, 3 — by clinical urgency and importance
C. 3, 1, 4, 2 — complete quick tasks first to clear the list
D. 4, 2, 1, 3 — admissions always take priority
Reveal Answer
Answer: B. 2, 4, 1, 3 — by clinical urgency and importance
Clinical prioritisation requires triage by urgency and importance. Post-dialysis potassium in a CKD Stage 5 patient is highest urgency and highest importance — dyskaelemia in CKD can cause fatal arrhythmia and the result is immediately actionable (task 2). Writing up the history of a new admission (task 4) is important because it starts the clinical record and is needed before investigations or management can be properly ordered — higher clinical priority than comfort measures or paperwork. Prescribing paracetamol for mild headache (task 1) is urgent only if the patient is in distress, but is clinically low-stakes. Discharge paperwork (task 3) for a clinically stable patient is low clinical urgency and can be delegated or done after higher-priority tasks. Option C (quick tasks first) is a common, dangerous cognitive trap — completing administratively easy tasks produces a false sense of progress while genuinely urgent clinical tasks wait.
Professional Networks, Career Advancement, and Mentoring
Professional networks (IM29.19) in medicine are the structured and semi-structured relationships through which clinicians exchange knowledge, support each other's development, manage clinical complexity through referral and consultation, and collectively advance the standards of the profession. Building and using an appropriate professional network is a clinical skill with direct patient care implications: the physician who has no functional referral network for complex cases will either attempt to manage cases beyond their scope or lose patients to delay and fragmentation of care.
Professional networks in Indian medicine operate at several levels. At the intra-institutional level, the network includes ward teams, specialty consultants, allied health professionals (physiotherapy, speech therapy, dietetics, social work, clinical psychology), and the institutional patient safety and ethics committees. At the local professional level, it includes the district medical association, specialty society chapters (API, CSI, RSSDI, etc.), postgraduate teaching hospital connections, and peer networks from medical school. At the national level, it includes national specialty society membership, journal clubs, CME event participation, and research collaborations. At the inter-professional level, it includes relationships with nurses, pharmacists, laboratory scientists, and community health workers — the colleagues whose expertise and observations are essential to safe, complete clinical care.
The most immediately relevant professional network skill for the final-year student is referral competency — the ability to identify when a patient requires specialist review, to communicate the referral clearly and completely, and to follow up appropriately. A good referral note includes: the referring physician's assessment of the problem, the specific question asked of the specialist, the relevant clinical information (not the entire case note), the urgency classification, and the contact details for follow-up communication. A poor referral — 'Please see and advise' with no clinical context — is a communication failure that burdens the receiving specialist, delays appropriate care, and may result in the wrong question being answered.
Career advancement (IM29.20) for the Indian medical graduate follows structured pathways that require deliberate planning. The principal postgraduate pathway is the National Board of Examinations (NBE) and university-based MD/MS/DNB programmes, entry to which is through NEET-PG. Superspecialty fellowship is via DM/MCh (through NEET-SS) or NBE fellowship programmes. Non-clinical career pathways include public health (MD Community Medicine, Masters in Public Health, WHO fellowship programmes), health administration, medical education, clinical research, and medical writing. The NMC and Medical Council of India (MCI) legacy regulations specify continuing education requirements for career advancement; state medical services and central government health services have structured promotion tracks. For the final-year student, career planning involves: early identification of specialty interest, targeted postgraduate examination preparation (NEET-PG, which tests basic sciences through to final-year clinical medicine), awareness of the postgraduate training landscape, and cultivation of mentoring relationships in their area of interest.
Mentoring (IM29.22) is a professional relationship in which a more experienced clinician supports the professional development of a less experienced one — through guidance, career advice, supervised learning, and modelling of professional standards. The NMC 2024 curriculum requires final-year students to demonstrate the ability to work in a mentoring relationship with junior colleagues — meaning they are expected to begin the transition from mentee to mentor at the earliest stage of seniority, even as interns and early residents. The practical behaviours of an effective mentor include: making time for the mentee's questions, providing constructive and specific feedback on observed performance, sharing your own experiences of uncertainty and error in a way that normalises learning from mistakes, advocating for the mentee's development needs within the institutional system, and maintaining appropriate professional boundaries in the relationship.
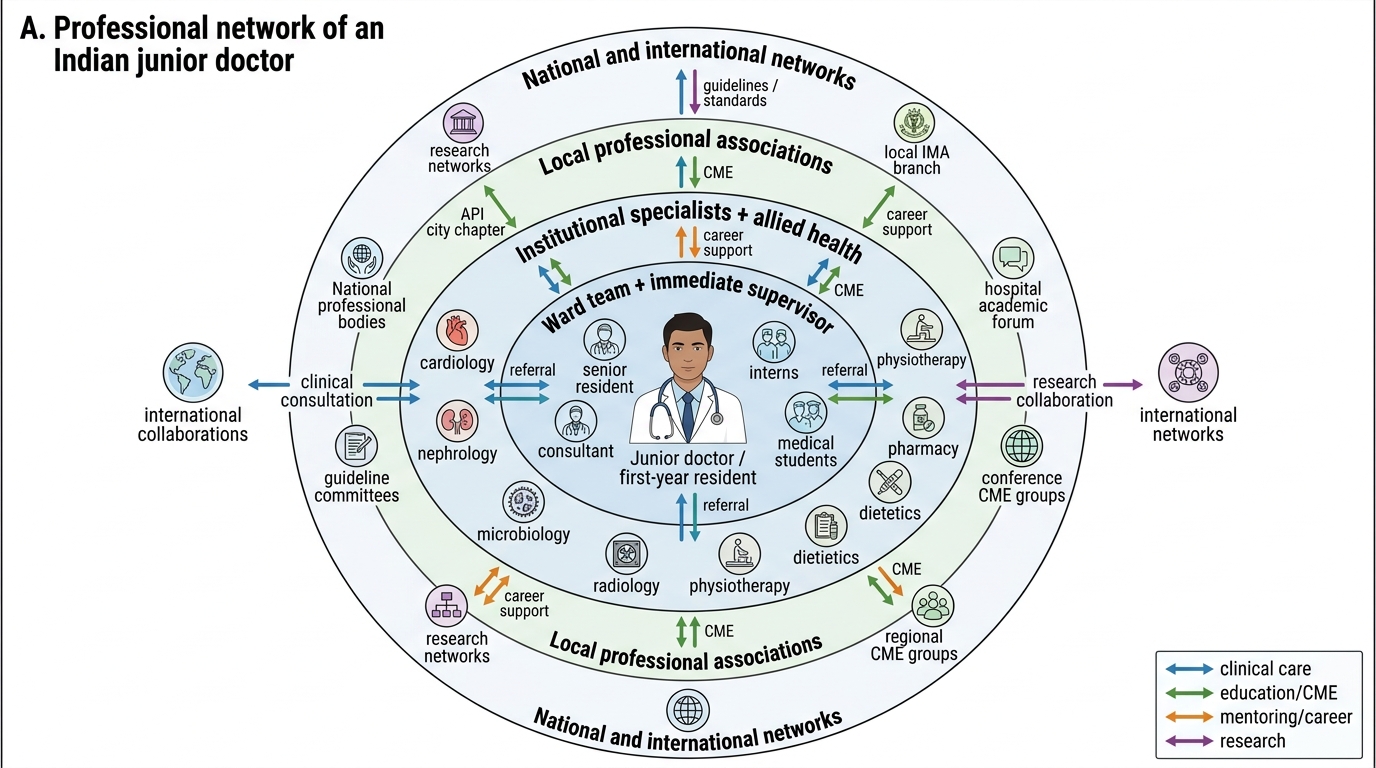
Professional Network of a Junior Doctor
SELF-CHECK
You are a first-year resident in internal medicine. A medical student on your ward asks you to explain the pathophysiology of type 2 diabetes after rounds. You are fatigued and have 15 tasks remaining. Which response BEST demonstrates the mentoring competency (IM29.22) within the constraints of your professional workload?
A. Tell the student you are too busy today and they should ask a textbook
B. Immediately spend 45 minutes on a comprehensive pathophysiology lecture despite your task list
C. Spend 5–10 minutes on the key concept, directing them to a specific resource for self-directed follow-up, and offer to discuss it further at a dedicated teaching time
D. Refer the student to the consultant for all teaching questions
Reveal Answer
Answer: C. Spend 5–10 minutes on the key concept, directing them to a specific resource for self-directed follow-up, and offer to discuss it further at a dedicated teaching time
Effective mentoring does not require abandoning all other professional obligations. The competent mentor balances the teaching opportunity with realistic time management — 5–10 minutes on the key concept is meaningful and respectful of the student's question, while directing them to a specific self-directed resource (not just 'read a textbook' but 'read Harrison's chapter 20 on T2DM pathophysiology') operationalises the lifelong learning model. Offering a follow-up time respects both the student's development and your own workload. Option A abdicates the mentoring responsibility entirely. Option B fails the time management competency (IM29.18) — 45 minutes for a non-urgent teaching interaction while 15 clinical tasks wait is poor prioritisation. Option D transfers the teaching relationship upward, which is appropriate for complex questions but not for a foundational pathophysiology query that a first-year resident should be able to address.