Page 6 of 20
IM3.4-6 | Pneumonia Clinical Evaluation — SDL Guide (Part 2)
Applying Examination Findings: Complications and Severity
Physical examination in pneumonia does not end with confirming the diagnosis — it must actively seek complications, because the presence of a complication fundamentally changes management. The three most clinically important complications to identify at the bedside are parapneumonic effusion/empyema, septic shock, and respiratory failure. Each has characteristic examination findings that alert the clinician before investigations confirm them.
Parapneumonic effusion: A new or enlarging effusion developing alongside a pneumonic consolidation is the most common complication. Clinically, as the effusion develops, the initial bronchial breathing and dullness of consolidation evolve toward reduced/absent breath sounds and a more stony, shifting dullness that extends beyond the original consolidation. Shifting dullness — dullness that moves with patient position — is specific to free-flowing effusion. An effusion that becomes loculated (as in early empyema) will have fixed dullness that does not shift. The detection of a new effusion on serial examination in a patient receiving antibiotics for pneumonia, particularly if fever persists, should prompt urgent pleural aspiration — because an empyema requires drainage and will not resolve with antibiotics alone. The key differentiating examination finding between simple effusion and empyema is clinical: fever persisting beyond 72 hours of appropriate antibiotics with a persistent or enlarging effusion is empyema until proven otherwise; the diagnosis is confirmed by pleural fluid analysis (pH <7.2, glucose <2.2 mmol/L, LDH >1000 IU/L, and/or positive culture).
Septic shock: In severe pneumonia, the systemic inflammatory response may exceed the capacity of the cardiovascular system, producing septic (distributive) shock — characterised by vasodilation, hypotension (systolic <90 mmHg), tachycardia (>100/min), and evidence of end-organ hypoperfusion. Examination findings: warm, flushed peripheries (early septic shock — vasodilation), poor capillary refill time >2 seconds, altered mental status (confusion, agitation), mottled or cool peripheries (late septic shock, onset of hypoperfusion). The sepsis 3 definition requires a suspected infection plus a change in SOFA score ≥2, with septic shock defined as MAP <65 mmHg despite fluid resuscitation plus a lactate >2 mmol/L. Identifying these signs on examination triggers immediate resuscitation: IV access, fluid bolus, blood cultures, urgent antibiotics, and monitoring for vasopressor requirement.
Respiratory failure: Progressive respiratory failure is the most immediately life-threatening complication. Examination signs: tachypnoea (≥30/min), use of accessory muscles, intercostal recession, pursed-lip breathing, inability to complete sentences, central cyanosis, paradoxical abdominal movement (a late sign of diaphragmatic fatigue). SpO2 on room air is the most sensitive single parameter — <90% demands supplemental oxygen and urgent assessment; <88% on high-flow oxygen signals impending need for mechanical ventilatory support. In patients with COPD, be alert to hypercapnic respiratory failure (type 2) — high-flow oxygen in COPD can suppress hypoxic drive and worsen CO2 retention; target SpO2 88–92% in confirmed COPD, not the >94% target for non-COPD patients.
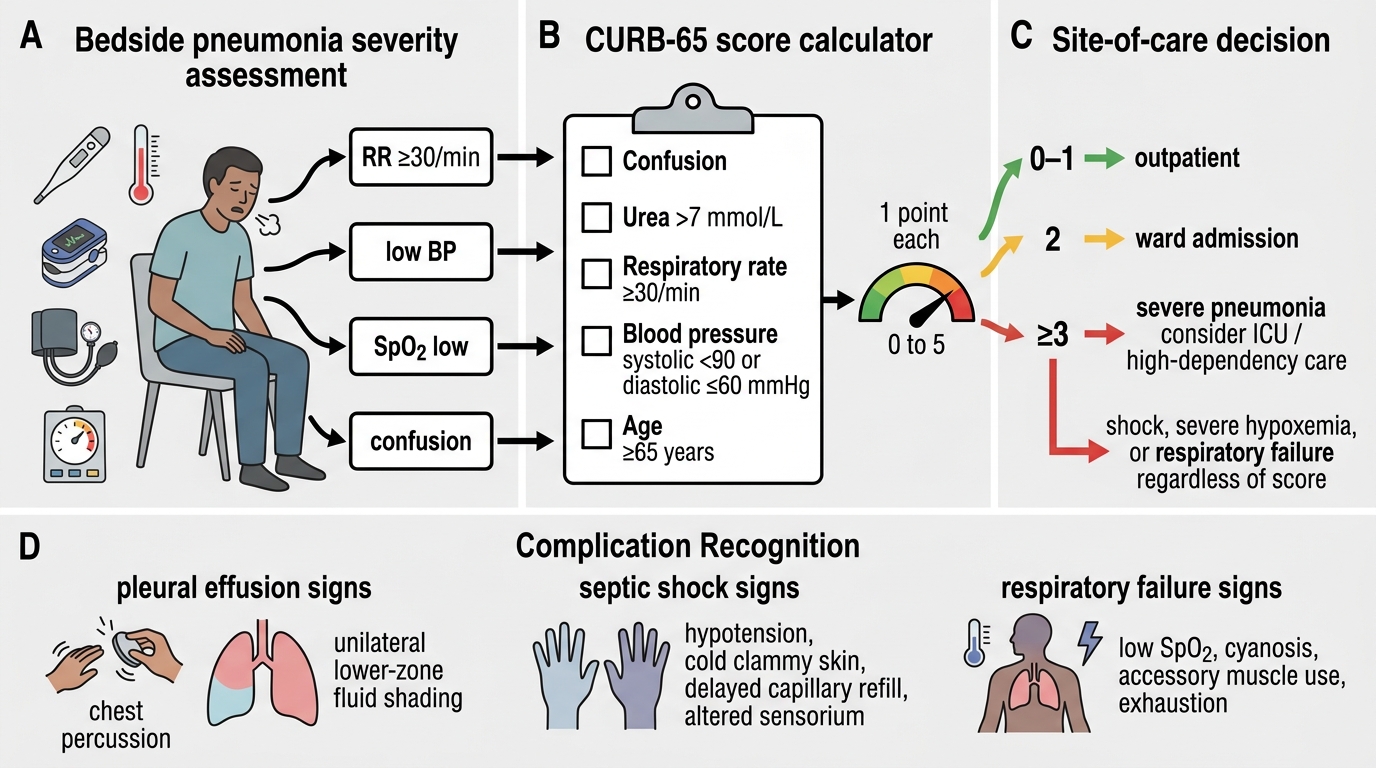
Pneumonia Severity Assessment Bedside Flowchart
Differential Diagnosis: Constructing and Prioritising the List
Constructing a differential diagnosis in pneumonia is not a formality — it is the cognitive process that prevents clinical errors and ensures the investigation plan is broad enough to catch alternative diagnoses that may have very different management implications. A clinician who anchors too early on 'pneumonia' and does not actively consider the differential will miss pulmonary tuberculosis (always relevant in India), malignancy with post-obstructive pneumonia, pulmonary embolism presenting with an infarction shadow, or acute pulmonary oedema misread as bilateral pneumonia. The ability to generate, document, and prioritise a differential from clinical features — as required by NMC IM3.6 — is what separates a diagnostically complete evaluation from a premature diagnostic closure.
The primary differential diagnoses for a patient presenting with fever, cough, breathlessness, and a new pulmonary opacity include: (1) Pneumonia — the most common; confirmed by the combination of fever, cough, focal consolidation, and clinical/investigation response to antibiotics; (2) Pulmonary tuberculosis — critically important in India; subacute onset over weeks, prominent constitutional features (weight loss, night sweats, anorexia), upper lobe predilection, absence of antibiotic response, haemoptysis, known contacts; any doubt demands early sputum AFB smear/GeneXpert and Mantoux testing; (3) Bronchogenic carcinoma with post-obstructive pneumonia — consider in a smoker over 40 with recurrent pneumonia in the same segment, a central hilar mass on CXR, or a collapse-consolidation pattern; the underlying tumour obstructs a bronchus, and the distal lung collapses and becomes infected; (4) Acute pulmonary oedema — mimics bilateral pneumonia with breathlessness and bilateral infiltrates; distinguished by clinical context (known heart failure, recent MI, elevated JVP, peripheral oedema, an S3 gallop, bilateral basal fine crackles rather than bronchial breathing, prompt response to diuresis rather than antibiotics); (5) Pulmonary embolism with pulmonary infarction — the classical 'Hampton's hump' (wedge-shaped pleural-based opacity) on CXR, with pleuritic pain, haemoptysis, risk factors for DVT (recent surgery, immobility, malignancy, oral contraceptive use), and tachycardia out of proportion to fever; Wells score calculation guides the investigation strategy; (6) Cryptogenic organising pneumonia (COP) — a non-infectious inflammatory lung disease presenting as recurrent 'pneumonia' not responding to repeated antibiotic courses, typically in women in their 50s; CXR shows migratory consolidation; requires bronchoscopic biopsy and responds to steroids, not antibiotics.
Prioritising the differential: In the Indian context, TB must always be in the top 3 for any patient with subacute onset, weight loss, or risk factors (close contact, HIV, undernutrition, overcrowded housing, prior TB). A patient presenting with lobar consolidation, acute onset, and positive pneumococcal urinary antigen has pneumonia as the leading diagnosis with near certainty, and investigation resources can be focused accordingly. A patient with a 6-week history of right upper lobe opacity, haemoptysis, and weight loss — even in the presence of fever — has TB as the leading diagnosis until three negative sputum smears/GeneXpert results are documented. The differential is not a static list; it should be actively revised at 48–72 hours of treatment: failure to improve clinically on appropriate antibiotics is the strongest prompt to widen the differential and reconsider TB, malignancy, or an alternative non-infectious diagnosis.
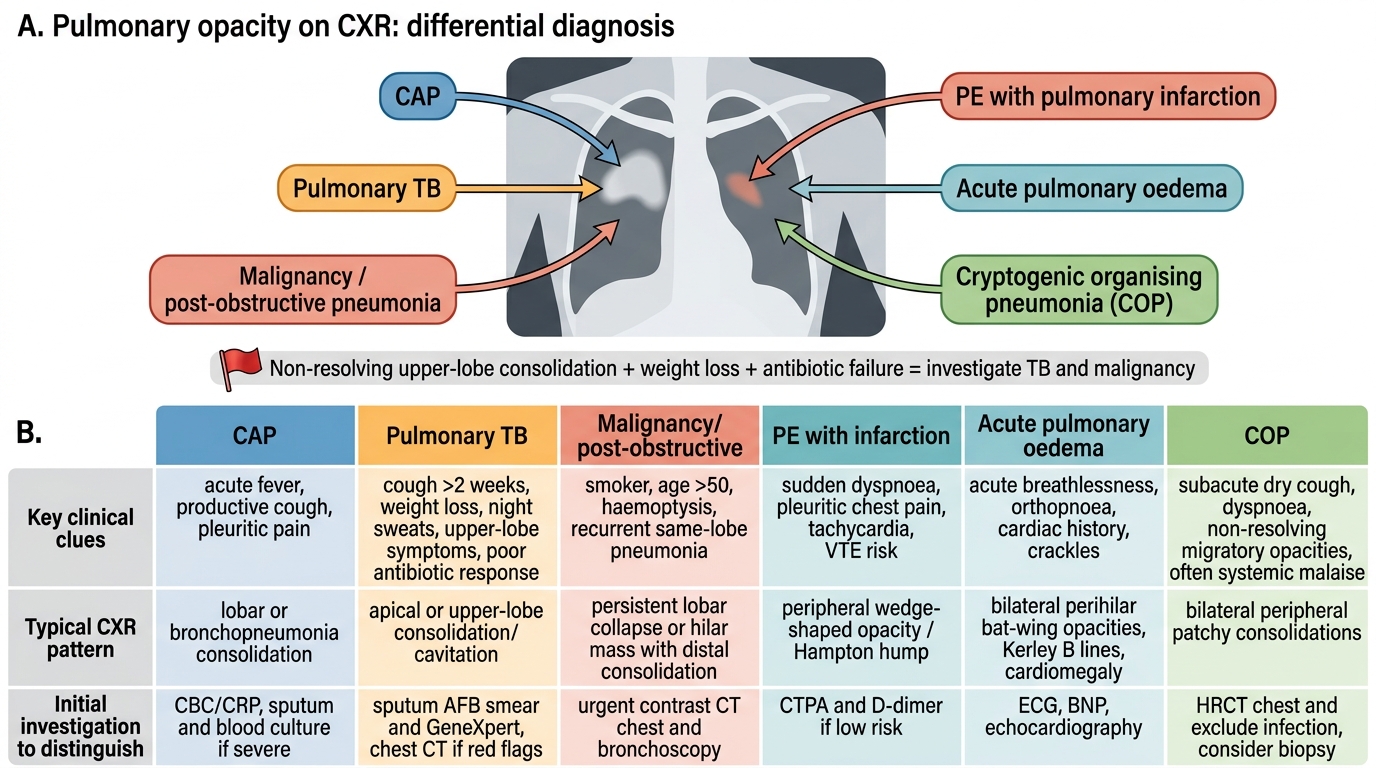
Differential Diagnosis of Pulmonary Opacity on CXR
SELF-CHECK
A 52-year-old male smoker presents with a 6-week history of low-grade fever, productive cough, weight loss of 4 kg, and right upper lobe consolidation on CXR. He has been given two courses of antibiotics by his general practitioner with no improvement. What is the MOST appropriate next step?
A. Change antibiotics to a respiratory fluoroquinolone for atypical pathogens
B. Admit for IV antibiotics and repeat CXR in 48 hours
C. Send three consecutive sputum samples for AFB smear/GeneXpert and obtain urgent chest CT
D. Perform a pleural aspiration to rule out empyema
Reveal Answer
Answer: C. Send three consecutive sputum samples for AFB smear/GeneXpert and obtain urgent chest CT
This presentation has multiple 'red flags' for pulmonary tuberculosis: subacute onset over 6 weeks (not the acute bacterial CAP course), upper lobe location (TB preferentially affects the apices and posterior segments of upper lobes due to high oxygen tension), significant weight loss (constitutional features of TB), failure to respond to two antibiotic courses, and an Indian patient (India carries the highest TB burden globally). In India, any patient with ≥2 weeks of cough with systemic features and no antibiotic response MUST be investigated for TB as a priority. Changing antibiotics without TB investigation is dangerous — fluoroquinolones have anti-TB activity and can mask TB while selecting for fluoroquinolone resistance in Mycobacterium tuberculosis. The correct next step is AFB smear/GeneXpert (NTEP protocol) + CT chest.
Self-Assessment: Applying Clinical Evaluation Skills
The three competencies covered in this module — history-taking (IM3.4), physical examination (IM3.5), and differential diagnosis generation (IM3.6) — must function together as a single integrated clinical reasoning process. These three skills are not performed in sequence; an experienced clinician is forming a differential diagnosis during the history, refining it during the examination, and revising it again in light of investigations. What distinguishes a skilled clinician from a novice is not just knowledge of individual physical signs but the capacity to synthesise findings from all sources into a probabilistic clinical judgment. The NMC competency framework at the SH (Skills and Handling) level requires that you can actually perform these skills at the bedside, document them accurately in the case record, and present your findings and reasoning to a supervisor in a structured format. The following cases test your ability to elicit and interpret the relevant clinical data, document the physical examination findings, and generate a prioritised differential. For each scenario, identify the key history points, expected physical examination findings, and the top three differential diagnoses in order of probability.
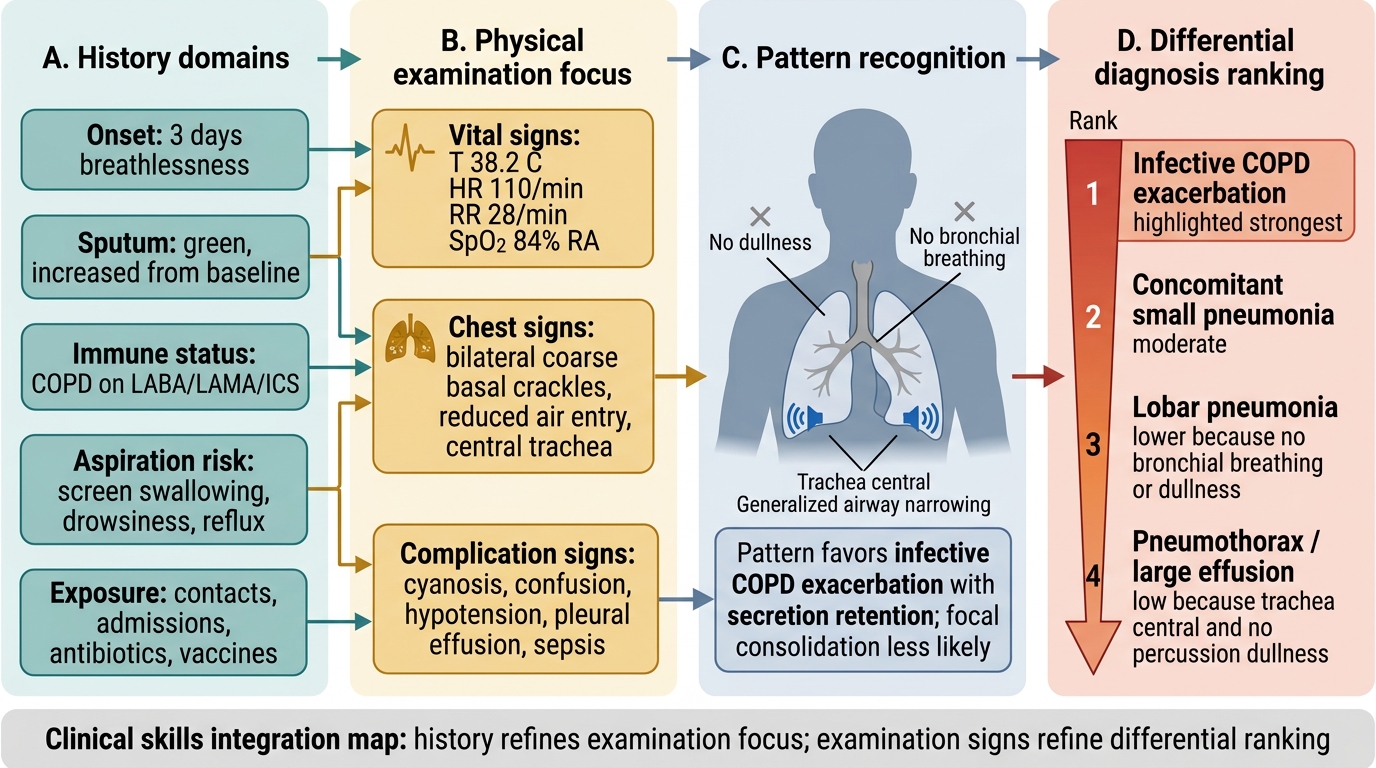
Clinical Skills Integration Map for Suspected Pneumonia in COPD
Scenario A: A 72-year-old woman with known COPD (on LABA/LAMA/ICS) is brought to the emergency department by her family. She has been increasingly breathless for 3 days, with a productive cough (green sputum). She had a similar episode 8 months ago requiring hospitalisation. Vital signs: temp 38.2°C, HR 110/min, RR 28/min, BP 110/70 mmHg, SpO2 84% on room air. She is oriented but anxious. Examination: bilateral coarse crackles at the bases, reduced air entry bilaterally, trachea central, no dullness on percussion, no bronchial breathing.
Key history focus: Duration and change from baseline COPD, prior hospitalisations, sputum change (a change from baseline sputum volume and colour is the hallmark of COPD exacerbation with infective precipitant), vaccination status, prior antibiotic use.
Physical examination interpretation: Tachycardia, tachypnoea, hypoxia (SpO2 84%). Bilateral coarse crackles without bronchial breathing or dullness — this pattern is more consistent with a COPD exacerbation with secretion retention and small airway disease than with lobar consolidation. The absence of bronchial breathing reduces the likelihood of a focal pneumonia, though a concomitant small pneumonia may be present and not clinically detectable.
Differential (prioritised): (1) Acute exacerbation of COPD with infective precipitant (H. influenzae, S. pneumoniae most likely); (2) Community-acquired pneumonia superimposed on COPD; (3) Left ventricular failure as a concomitant diagnosis (common in elderly COPD patients with cardiovascular comorbidity). CXR is mandatory to distinguish these.
Scenario B: A 34-year-old call centre employee presents with 12 days of dry cough, headache, and low-grade fever (37.9°C). He has taken two courses of amoxicillin with no improvement. Vital signs: HR 88/min, RR 18/min, BP 120/80 mmHg, SpO2 96% on room air. He is oriented. Examination: mild bilateral fine crackles on auscultation, no bronchial breathing, no dullness.
Key history focus: Occupational exposure to cooling systems or hotel stays (Legionella), animal contact, nature of cough (dry = atypical), extrapulmonary symptoms (ear pain = bullous myringitis in Mycoplasma, GI symptoms = Legionella), similar illness in household contacts (Mycoplasma spreads within households).
Physical examination interpretation: Near-normal examination despite 12 days of illness — a 'walking pneumonia' picture. Failure to respond to two courses of amoxicillin (a standard CAP beta-lactam) is the key clue: atypical pathogens (Mycoplasma, Chlamydophila) are intrinsically resistant to penicillins because they lack a cell wall.
Differential (prioritised): (1) Mycoplasma pneumoniae (atypical CAP — gradual onset, dry cough, penicillin non-response, ambulatory); (2) Chlamydophila pneumoniae (similar picture, often with pharyngitis); (3) Early pulmonary TB (India: must always consider if subacute course). CXR will show bilateral patchy infiltrates in Mycoplasma. Macrolide treatment (azithromycin) is appropriate empirically.
SELF-CHECK
In a 68-year-old man with a confirmed right lower lobe pneumonia, your examination reveals dull percussion at the right base with reduced breath sounds and absent vocal resonance at that level. Compared to two days ago when you noted bronchial breathing, this change most likely indicates:
A. Resolution of the pneumonia with clearing of the consolidation
B. Development of a right-sided parapneumonic pleural effusion
C. Progression to lung abscess formation
D. Contralateral spread of infection
Reveal Answer
Answer: B. Development of a right-sided parapneumonic pleural effusion
The shift from bronchial breathing with increased vocal resonance (consolidation signs) to dull percussion with REDUCED/absent breath sounds and absent vocal resonance signals fluid accumulation in the pleural space — a parapneumonic effusion developing alongside the consolidation. Resolution of pneumonia would produce return of normal vesicular breathing and resonant percussion, not dull percussion with absent sounds. Lung abscess produces cavitation but the consolidation signs and breath sounds remain; the cavity itself may produce amphoric breathing. Contralateral spread would add new findings on the left, not change existing right-sided signs. This evolution of findings is a common OSCE and clinical scenario — it tests the specific differential between consolidation and effusion signs.
CLINICAL PEARL
The respiratory rate is the most underused and most powerful vital sign in pneumonia. Studies consistently show that tachypnoea (RR ≥25–30/min) is the earliest and most sensitive marker of severity — more so than fever, white cell count, or even SpO2 in early deterioration. Yet in clinical practice, respiratory rate is the vital sign most commonly estimated rather than actually counted, with most practitioners using 'tachypnoeic' as an unquantified descriptor. Count it for a full 30 seconds and double the result — this takes 30 seconds and directly determines the CURB-65 score, which determines site of care. A patient with RR 32/min scores a CURB-65 point regardless of all other parameters, and that point may push a score from 2 to 3, changing the management from 'consider admission' to 'admit and assess for ICU.' For the TB differential: in India, the habit of always asking 'could this be TB?' before adding a second course of antibiotics is not overcaution — it is the single most important diagnostic habit in respiratory medicine practice on the subcontinent.