Page 8 of 20
IM3.7-14 | Pneumonia Diagnostic Testing — SDL Guide
Learning Objectives
- Order and interpret the standard diagnostic investigations for pneumonia including CBC, chest X-ray PA view, Mantoux test, sputum Gram stain and culture, and blood cultures, understanding the quality criteria that determine result validity
- Demonstrate correct technique for arterial blood gas collection (modified Allen's test, radial artery approach) and interpret ABG reports including type 1 and type 2 respiratory failure patterns
- Demonstrate correct technique for pleural fluid aspiration and interpret pleural fluid analysis results using Light's criteria and pH to decide between observation and drainage
- Apply PITC (provider-initiated HIV testing) in the pneumonia workup and understand how HIV status alters the diagnostic and management approach
- Identify the clinical indications for advanced investigations including HRCT, viral PCR, urinary antigen tests, BAL, and specialised serology
INSTRUCTIONS
This module develops the procedural and interpretive diagnostic skills essential for the full workup of pneumonia, from bedside specimen collection to advanced investigation selection. These competencies bridge the clinical assessment from the previous module to the management decisions in the next — understanding what the investigation tells you and what its limitations are is as important as the technical ability to perform it.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 121 — Pneumonia (textbook)
- API Textbook of Medicine, 10th ed. — Respiratory Investigations and Procedures (textbook)
- BTS Guidelines on Pleural Disease: Thoracentesis and Pleural Fluid Analysis, 2010 (updated 2023) (guideline)
- NACO Guidelines for Provider-Initiated HIV Testing and Counselling (PITC), 2016 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old woman is brought to the emergency department with a 3-day history of fever and productive cough. The emergency physician orders a chest X-ray and a full blood count. The CXR report comes back: 'Right lower lobe consolidation — clinical correlation advised.' The white cell count is 18,000/mm³ with neutrophilia. The physician starts amoxicillin and admits the patient to the ward. On day 2, she is worse: fever persists at 39.2°C, respiratory rate is 34/min, and SpO2 has dropped to 88% on 4 L/min oxygen. The ward doctor wonders — should she have had blood cultures? An ABG? A sputum culture before antibiotics were started? Could this be a resistant organism that would have been caught with earlier, broader diagnostic testing? This is the diagnostic dilemma at the heart of pneumonia management: which tests, in which order, with which urgency, and how to interpret each result. The answer changes depending on severity, setting, immune status, and clinical suspicion. Ordering tests without knowing how to interpret them is as dangerous as not ordering them at all — because a misread ABG that misses respiratory failure, or a blood culture incorrectly labelled as contaminated, can delay life-saving decisions.
WHY THIS MATTERS
The NMC competencies IM3.7 through IM3.14 cover the full diagnostic toolkit for pneumonia at the skills (SH) and knowledge-applied (KH) levels: ordering and interpreting the complete blood count, chest X-ray, Mantoux test, sputum Gram stain and culture, pleural fluid examination, HIV testing, and arterial blood gas (ABG); performing the technique of ABG collection and pleural aspiration on a mannequin; interpreting ABG reports and blood culture reports; and knowing the indications for advanced testing (HRCT, viral cultures, PCR, and specialised assays). In Indian clinical practice, every one of these investigations will be encountered daily — and the ability to perform a pleural aspiration safely, interpret an ABG correctly under time pressure, and understand when a blood culture result represents true infection versus contamination are the skills that determine patient outcomes. These competencies also prepare you for the MCI/NMC practical and viva assessments where procedural technique and result interpretation are directly tested.
RECALL
Recall the physiology of gas exchange from your first-year studies. In the alveolus, oxygen moves from alveolar gas into pulmonary capillary blood down a partial pressure gradient; carbon dioxide moves in the opposite direction. Normal arterial values: PaO2 80–100 mmHg, PaCO2 35–45 mmHg, pH 7.35–7.45, HCO3 22–26 mEq/L, SaO2 ≥95%. In pneumonia, consolidated alveoli are perfused but not ventilated — this is a ventilation-perfusion (V/Q) mismatch, specifically a low-V/Q unit, which is the primary cause of hypoxaemia. The first compensatory response to hypoxaemia is hyperventilation, which reduces PaCO2 (producing a low PaCO2 — a respiratory alkalosis). Only in severe pneumonia with respiratory muscle fatigue or airway obstruction does PaCO2 rise (type 2 respiratory failure). Recall also the principles of bacteriological culture media: blood agar for most bacteria, MacConkey agar to differentiate Gram-negative enteropathogens; BCYE (buffered charcoal yeast extract) specifically for Legionella. The Gram stain distinguishes Gram-positive (blue/purple — thick cell wall, peptidoglycan layer) from Gram-negative (red/pink — thin cell wall, lipopolysaccharide outer membrane) organisms, and identifies cocci versus rods.
Clinical Indication: Selecting the Right Diagnostic Tests
The diagnostic evaluation of pneumonia is stratified by clinical severity and setting — not every patient requires every investigation, and ordering the full panel for every patient with a mild outpatient CAP is both resource-wasteful and can generate confusing spurious results. The guiding principle is that investigations should answer clinical questions that cannot be answered by history and examination alone, and each test ordered should have a specific downstream management implication. In a patient with low-severity CAP (CURB-65 0–1) and a typical pneumococcal presentation, a CXR and CBC may be sufficient to confirm the diagnosis and begin outpatient oral antibiotics; proceeding to blood cultures, ABG, and pleural aspiration in this setting adds cost without clinical benefit. Conversely, in a patient with CURB-65 ≥3, haemoptysis, suspected immunodeficiency, or failure to improve on initial antibiotics, an extensive diagnostic workup is not optional — it is mandatory.
The tiered approach to diagnostic investigation in pneumonia follows three tiers: (1) Minimum workup for all hospitalised patients — CBC with differential, CXR PA view, blood urea/creatinine/electrolytes (for CURB-65 urea point and AKI assessment), liver function tests (for Legionella, drug toxicity), blood cultures ×2 before antibiotics, sputum Gram stain and culture before antibiotics, pulse oximetry/SpO2. (2) Additional investigations for moderate-severe CAP (CURB-65 ≥3) or suspected specific pathogen — arterial blood gas (ABG) for SpO2 <94% or tachypnoea ≥30/min; pleural aspiration if effusion >10 mm on lateral decubitus view; Legionella urinary antigen (all hospitalised moderate-severe CAP); pneumococcal urinary antigen; HIV test; procalcitonin and CRP (for antibiotic stewardship). (3) Specialised testing for specific clinical scenarios — HRCT for suspected atypical pneumonia, early IPA, COP, or CXR-normal severe hypoxaemia; Mantoux/tuberculin skin test and GeneXpert/AFB smear for TB; specific viral PCR (influenza, SARS-CoV-2, RSV) in epidemic settings; bronchoalveolar lavage (BAL) for immunocompromised patients with diffuse infiltrates; serology for Mycoplasma (cold agglutinins, Mycoplasma IgM), Legionella (serogroup antibodies), and Chlamydophila.
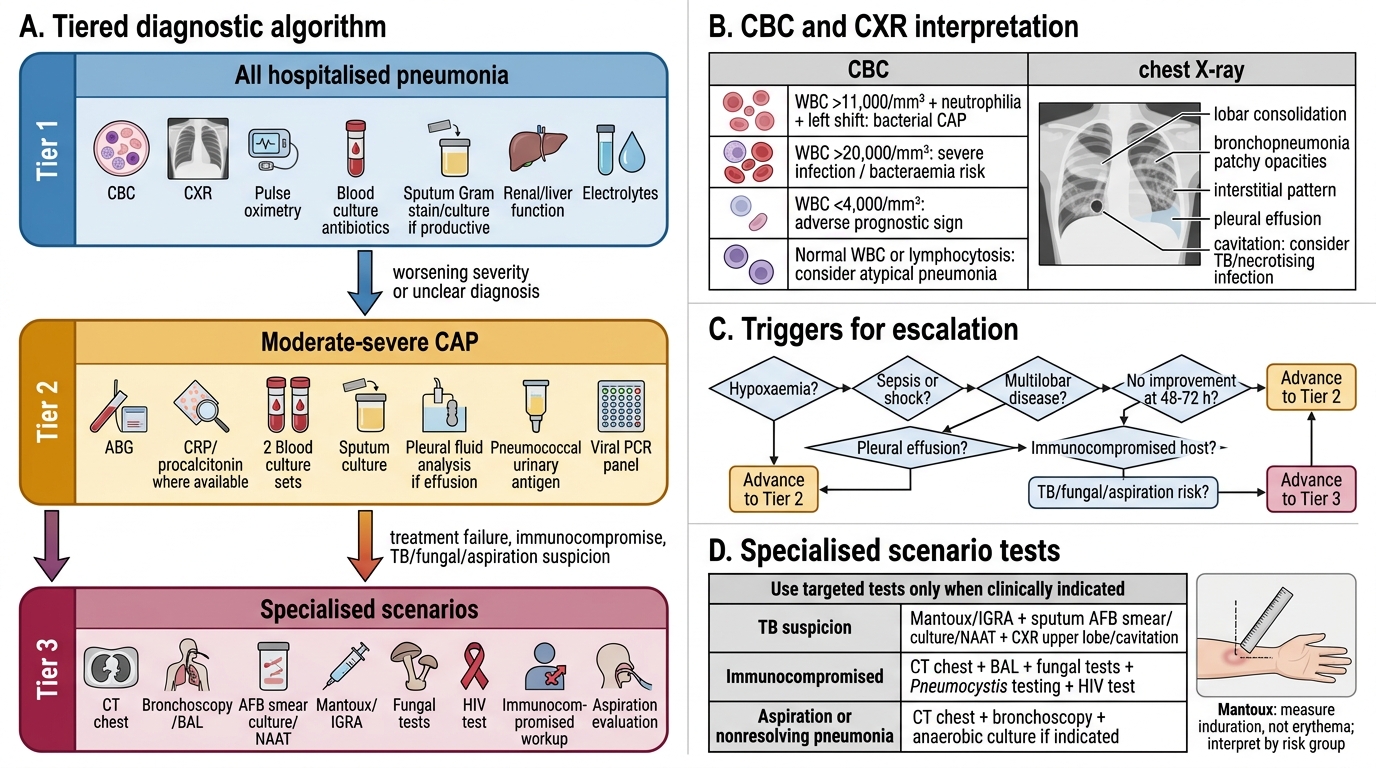
Tiered Diagnostic Algorithm for Hospitalised Pneumonia
CBC, CXR, and Mantoux: Interpretation
The complete blood count and chest X-ray are the two most universally obtained investigations in pneumonia, and the ability to interpret both correctly — not just identify 'consolidation' on CXR or 'high WBC' on CBC — is the foundational diagnostic skill required by IM3.7.
Complete blood count (CBC) interpretation in pneumonia: A leucocytosis (white cell count >11,000/mm³) with a neutrophilia and left shift (increase in band forms, immature neutrophils) strongly supports bacterial infection. The degree of leucocytosis provides a rough severity marker: a WBC >20,000/mm³ with marked left shift is associated with higher severity and bacteraemia risk. Leucopenia (WBC <4,000/mm³) is an adverse prognostic sign — it reflects overwhelming sepsis, impaired bone marrow response, or an underlying haematological condition (lymphoma, aplasia); in the elderly and in immunocompromised patients, leucopenia may be the presenting feature of serious pneumococcal bacteraemia. In atypical pneumonia (Mycoplasma), the WBC may be relatively normal (not the severe leucocytosis of bacterial CAP) and a lymphocytosis may be present. The presence of anaemia (haematocrit low, haemoglobin low) raises the concern for Mycoplasma haemolytic anaemia (cold agglutinin-mediated) or chronic underlying disease; thrombocytopaenia with purpura or petechiae suggests a more severe sepsis with disseminated intravascular coagulation (DIC). The platelet count should always be reviewed in the context of the WBC and clinical severity.
Chest X-ray interpretation in pneumonia: The CXR remains the standard confirmatory test for pneumonia — a new pulmonary infiltrate or consolidation in the appropriate clinical context confirms the diagnosis. The PA (posterior-anterior) view is preferred: the patient stands with their chest against the plate and the X-ray beam passes from posterior to anterior, minimising cardiac magnification. For bedside/ICU patients, an AP (anterior-posterior) view is obtained — this magnifies the cardiac silhouette and mediastinum, which must be noted when interpreting apparent cardiomegaly. Key CXR findings in pneumonia: (a) Air bronchogram sign — radiolucent bronchi visible within a dense consolidation, indicating that the bronchi are patent and air-filled while the surrounding alveoli are fluid-filled; this sign confirms that the opacity is truly an alveolar (airspace) process rather than atelectasis or a mass; it is the most reliable CXR sign of consolidation; (b) Lobar consolidation — homogeneous dense opacity filling a lobe or major segment, with well-defined margins demarcated by the fissure; classic pneumococcal pattern; (c) Bronchopneumonia pattern — bilateral, patchy, peribronchial infiltrates, poorly defined; typical of H. influenzae, S. aureus, and VAP; (d) Perihilar bilateral ground-glass — bilateral hazy opacities radiating from the hila; typical pattern of PCP and pulmonary oedema (differentiated by clinical context); (e) Bulging fissure sign — downward bowing of the horizontal fissure from the large, gelatinous lobar exudate; classic Klebsiella sign; (f) Cavitation/abscess — thick-walled cavity, often with an air-fluid level; aspiration pneumonia with anaerobes or Klebsiella; (g) Bilateral fluffy infiltrates — bilateral extensive alveolar filling; severe HAP/VAP, ARDS pattern.
Mantoux (tuberculin skin test) in the context of pneumonia: The Mantoux test involves intradermal injection of 2 tuberculin units (2 TU) of Purified Protein Derivative (PPD) into the volar forearm and reading the induration (not erythema) diameter at 48–72 hours. A positive result is defined as: ≥10 mm induration in immunocompetent adults in endemic areas (India); ≥5 mm in HIV-positive patients, recent TB contacts, or immunocompromised individuals; ≥15 mm in low-risk populations. The Mantoux does NOT diagnose active TB — it indicates sensitisation to tuberculin proteins, which can result from prior BCG vaccination, latent TB infection, or active TB disease. In the context of a pneumonia workup, a positive Mantoux supports TB in the differential and warrants sputum AFB smear/GeneXpert. A negative Mantoux in a severely immunocompromised patient does NOT exclude TB — anergy (inability to mount a delayed hypersensitivity response due to profound immunosuppression) can produce a false-negative result.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
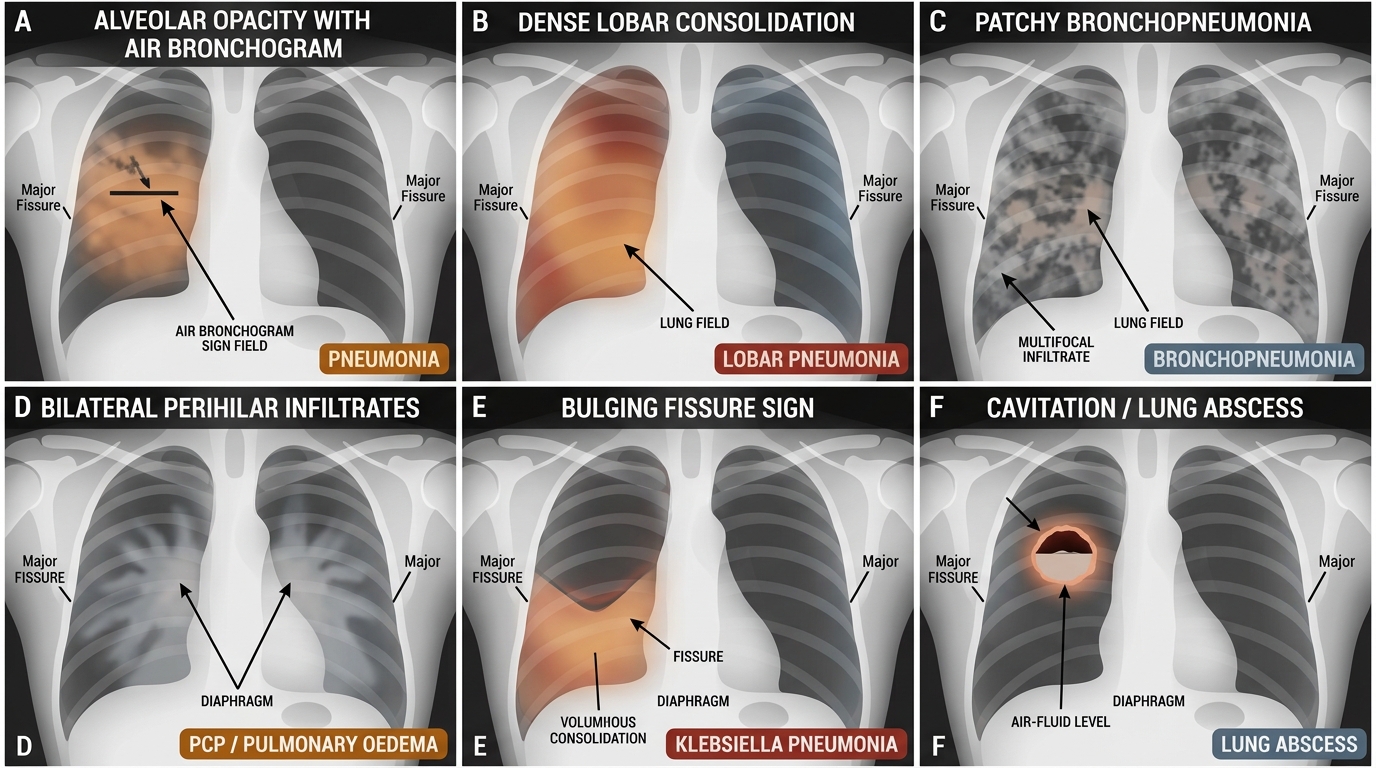
Chest X-ray Patterns in Pneumonia
Sputum Gram Stain, Culture, and Blood Culture: Principles and Interpretation
Microbiological investigation is the cornerstone of pneumonia diagnosis beyond the bedside, enabling pathogen identification and sensitivity testing that allows transition from empirical to directed, narrow-spectrum therapy. The three key microbiological investigations are sputum Gram stain and culture, and blood cultures — all of which must be obtained BEFORE the first antibiotic dose. This is not merely good practice but a clinical imperative: even a few minutes of antibiotic exposure can suppress bacterial growth in culture, particularly for fastidious organisms like pneumococcus, and dramatically reduce the diagnostic yield. In a severely ill patient where antibiotics must be started immediately, the two blood culture sets should be drawn before the first dose is given — this adds at most 5 minutes and does not delay treatment meaningfully.
Sputum Gram stain and culture: The diagnostic value of sputum bacteriology depends entirely on the quality of the specimen. A good-quality sputum specimen is defined as: ≥25 polymorphonuclear leucocytes (PMNs) per low-power field (10× objective) and <10 squamous epithelial cells per low-power field — indicating that the specimen comes from the lower respiratory tract, not saliva. A specimen with >10 squamous epithelial cells per LPF is a salivary specimen and should be rejected and recollected; reporting bacteriology from a salivary specimen gives false-positive results for colonising organisms and misleads antibiotic selection. In a good-quality specimen, the Gram stain result has high predictive value: (a) abundant Gram-positive diplococci (lancet-shaped pairs) = Streptococcus pneumoniae (sensitivity 60–70%, specificity >90% for pneumococcal pneumonia when paired with culture); (b) Gram-negative coccobacilli = Haemophilus influenzae; (c) Gram-positive cocci in clusters = Staphylococcus aureus; (d) large Gram-negative rods with a mucoid capsule = Klebsiella pneumoniae; (e) a mixed flora with both Gram-positive and Gram-negative organisms including long rod-shaped forms = anaerobic mixed infection (aspiration pneumonia); (f) no organisms visible despite multiple PMNs = suggests atypical pathogen (Mycoplasma, Legionella, Chlamydophila do not appear on standard Gram stain) or prior antibiotic treatment. Culture results take 24–48 hours, with sensitivity and resistance testing (antibiogram) available at 48–72 hours. The culture result should prompt de-escalation — if pneumococcus is confirmed as susceptible to penicillin, broaden-spectrum antibiotics should be narrowed to amoxicillin.
Blood culture technique (IM3.12) and interpretation (IM3.13): Blood cultures are the gold standard for diagnosing bacteraemia complicating pneumonia and for identifying the causative organism with full sensitivity testing. Bacteraemia is present in 20–30% of hospitalised pneumococcal CAP and carries prognostic significance. The correct technique: clean the skin with 2% chlorhexidine (or 70% isopropyl alcohol) and allow to dry completely; collect two sets (aerobic and anaerobic bottles each time) from two separate venepuncture sites (typically both arms) — the purpose of two sets from separate sites is to reduce the rate of false-positive results from skin contamination; each set contains one aerobic and one anaerobic bottle; the volume of blood per bottle should be 8–10 mL in adults. Interpretation: a positive blood culture is classified as true bacteraemia if the same organism grows in both sets from separate sites, if the organism is a primary pathogen (S. pneumoniae, K. pneumoniae, S. aureus, E. coli always represent true bacteraemia regardless of a single bottle), or if the culture grows an organism consistent with the clinical picture and the Gram stain. A positive culture for a typical contaminant (coagulase-negative Staphylococci — CNS, Corynebacterium species, Bacillus species, Propionibacterium) in a single bottle from a single site is likely a skin contaminant and should not drive antibiotic changes unless the patient is immunocompromised or has a prosthetic device (where CNS bacteraemia is clinically relevant). True S. aureus bacteraemia always requires treatment — S. aureus is never a contaminant.
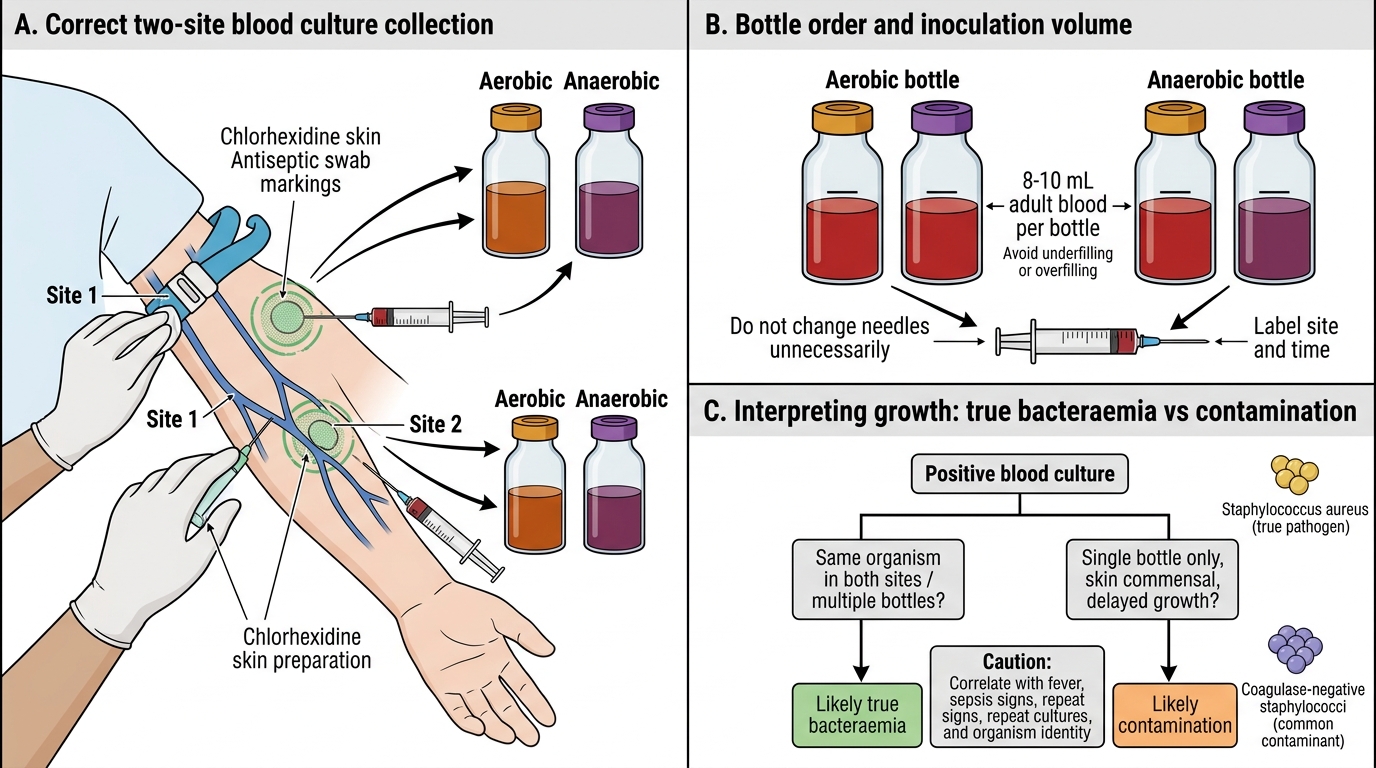
Blood Culture Collection and Interpretation
SELF-CHECK
A sputum sample from a 60-year-old man with suspected CAP is examined under the microscope. The low-power field shows 8 polymorphonuclear leucocytes and 15 squamous epithelial cells per low-power field. The Gram stain shows mixed flora. What is the correct action?
A. Report the result as polymicrobial infection and start broad-spectrum antibiotics
B. Identify the dominant Gram-positive organism and treat accordingly
C. Reject the specimen and ask the patient to produce a new deep cough specimen from the lower respiratory tract
D. Send the same specimen for AFB smear to rule out TB
Reveal Answer
Answer: C. Reject the specimen and ask the patient to produce a new deep cough specimen from the lower respiratory tract
A specimen with >10 squamous epithelial cells per LPF is a salivary (mouth-derived) specimen — it reflects oral flora colonising the mouth, not lower respiratory tract pathogens. Reporting bacteriology from a salivary specimen leads to incorrect antibiotic selection based on oral commensals. The correct action is to reject the specimen and request a new one from a deep cough after mouth-rinsing. An acceptable sputum specimen requires ≥25 PMNs and <10 squamous epithelial cells per LPF. A different specimen (BAL or induced sputum) may be needed if the patient cannot produce a good-quality spontaneous specimen.