Page 1 of 20
IM3.1-3 | Pneumonia Foundations — SDL Guide
Learning Objectives
- Define and distinguish community-acquired, hospital-acquired (nosocomial), and aspiration pneumonia using standard criteria
- Describe the microbiological aetiology of each pneumonia syndrome, including typical and atypical pathogens in CAP and the Gram-negative/MDR pathogen profile of HAP/VAP
- Explain how the host's immune status (HIV, neutropenia, diabetes, transplant) modifies the pathogen spectrum and clinical approach
- Describe the pathogenesis and four-stage pathological sequence of lobar pneumonia and the natural history of resolution
- Enumerate the local and systemic complications of pneumonia and recognise clinical features that signal their development
INSTRUCTIONS
This module lays the conceptual and microbiological foundation for all subsequent pneumonia clinical skills. You will learn to classify the three pneumonia syndromes, identify the likely pathogen based on acquisition setting and host factors, and understand the pathogenesis and complications that shape clinical management. This knowledge underpins the rational empirical antibiotic choices you will be making from day one of clinical practice.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 121 — Pneumonia (textbook)
- API Textbook of Medicine, 10th ed. — Respiratory Medicine section: Pneumonia (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 17 — Respiratory Disease (textbook)
- BTS/NICE Guidelines on Community-Acquired Pneumonia in Adults (updated 2019) (guideline)
- IDSA/ATS Consensus Guidelines for Community-Acquired Pneumonia (2019 update) (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM in the emergency department. A 68-year-old retired schoolteacher, Mr. Krishnamurthy, is brought in by his son. He has had a fever for four days, a productive cough with rust-coloured sputum for the past two days, and now he cannot complete a sentence without stopping to breathe. His SpO2 on room air is 84%. His respiratory rate is 32 per minute. His chest X-ray shows a dense right lower lobe consolidation — a classic lobar pneumonia pattern. His son, wringing his hands in the waiting area, asks: 'How did this happen so fast? Two days ago he was gardening.' Now consider a very different scenario: a 44-year-old man with type 2 diabetes is admitted to the orthopaedic ward for an elective knee replacement. He receives prophylactic antibiotics, is ventilated for 18 hours post-operatively, and by day 5 develops fever, purulent secretions from his endotracheal tube, and a new patchy infiltrate on chest X-ray. Same diagnosis label — pneumonia — but a completely different pathogen landscape, different host vulnerabilities, and a different treatment logic. Pneumonia is not one disease. It is a syndrome whose character is shaped entirely by three questions: where was it acquired, who is the host, and what organism has taken advantage of both?
WHY THIS MATTERS
Pneumonia is the single most common cause of infection-related death worldwide and a leading cause of hospitalisation across all age groups in India. According to the Indian Council of Medical Research and the Global Burden of Disease data, lower respiratory tract infections including pneumonia account for over 400,000 deaths annually in India, with children under five and adults over 65 bearing the greatest burden. For the final-year MBBS student and the junior doctor entering clinical practice, pneumonia is not a theoretical exercise — it is a presentation you will encounter in every posting, in every season, and in every age group. The NMC competencies IM3.1 through IM3.3 establish the conceptual and microbiological foundation that all subsequent clinical skills (IM3.4–IM3.22) build upon. Understanding the distinction between community-acquired, nosocomial, and aspiration pneumonia — and grasping the aetiology based on host immune status and clinical setting — is the cognitive scaffolding that allows you to make rational empirical antibiotic choices before culture results return, and to anticipate complications before they declare themselves clinically.
RECALL
Before proceeding, activate your foundation knowledge from your earlier respiratory and microbiology studies. The lower respiratory tract — from the trachea to the alveoli — is normally sterile; the upper respiratory tract, oral cavity, and pharynx harbour commensal flora including streptococci, haemophili, and anaerobes. The lung's defence mechanisms include: (1) the mucociliary escalator — ciliated epithelium and mucus that trap and expel inhaled particles; (2) alveolar macrophages — the resident phagocytes that handle microorganisms reaching the alveoli under normal aspiration loads; (3) immunoglobulins (particularly IgA in secretions and IgG in alveolar lining fluid); and (4) the cough reflex — the most powerful mechanical defence. Recall from pharmacology that beta-lactam antibiotics inhibit cell-wall synthesis (bactericidal), macrolides inhibit the 50S ribosome (bacteriostatic), fluoroquinolones inhibit DNA gyrase (bactericidal), and aminoglycosides inhibit the 30S ribosome. These mechanisms govern empirical antibiotic selection by organism type. Also recall the concept of normal respiratory flora — organisms such as Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis may colonise the nasopharynx without causing disease; pneumonia results when host defences fail or an organism's virulence overwhelms intact defences.
Defining the Three Pneumonia Syndromes
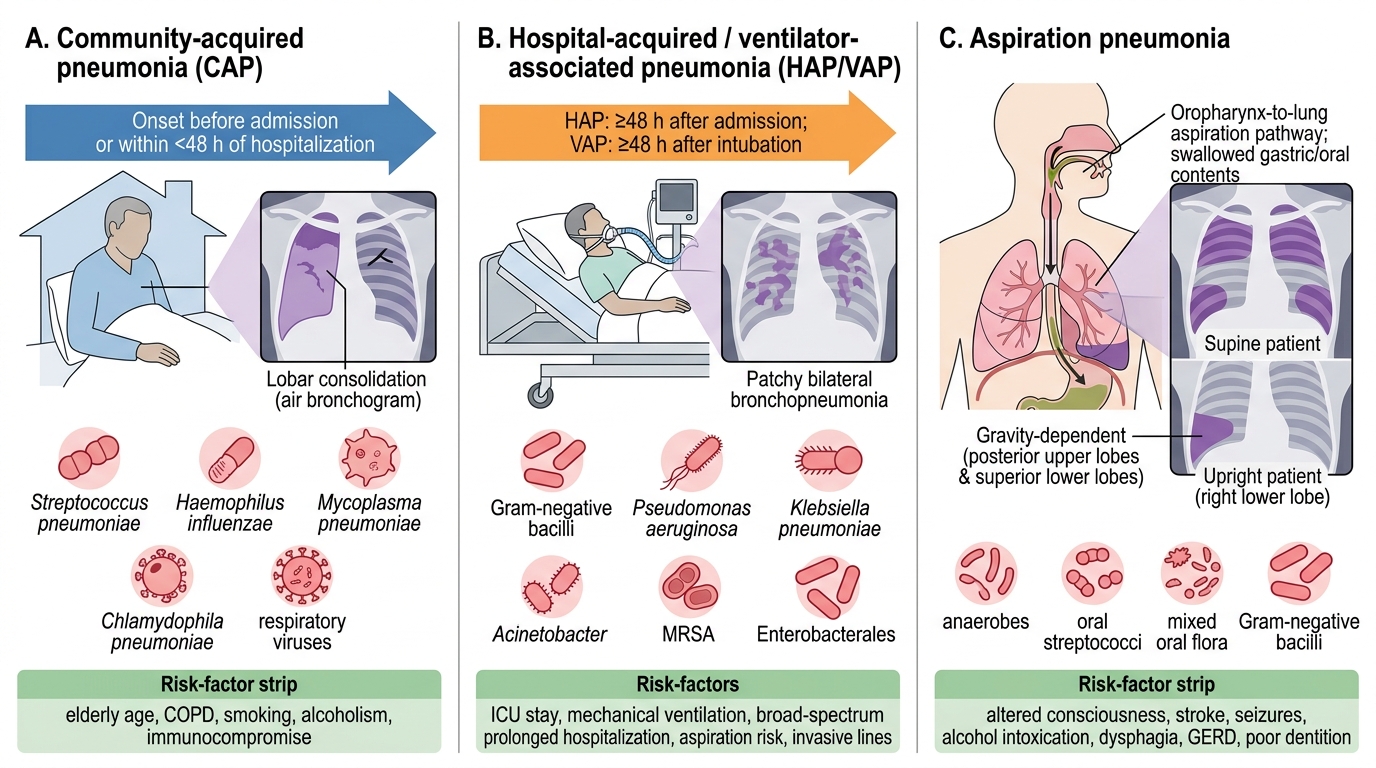
The clinical and microbiological diversity of pneumonia is best managed by first establishing which syndrome is present, because the syndrome determines the likely pathogen and therefore the empirical treatment strategy. Three syndromes are clinically and epidemiologically distinct: community-acquired pneumonia (CAP), nosocomial (hospital-acquired) pneumonia (HAP), and aspiration pneumonia. These are not merely administrative categories — they reflect fundamentally different host exposures, different microbial communities, and different patterns of antibiotic resistance, all of which must be factored into the initial management decision made before any culture result is available.
Community-acquired pneumonia (CAP) is defined as an acute lower respiratory tract infection acquired outside of a hospital setting or within the first 48 hours of hospitalisation in a patient who has not been hospitalised or resident in a nursing or long-term care facility for ≥90 days prior to admission. The 48-hour boundary is somewhat arbitrary but clinically useful — it separates patients who were already carrying a hospital-environment microbial flora at the time of admission from those who acquired their infection in the community. CAP affects immunocompetent and immunocompromised individuals alike, though the pathogen spectrum differs substantially between these two groups. In immunocompetent adults in India, the overwhelming majority of CAP is caused by a limited number of organisms, allowing a rational empirical approach.
Nosocomial pneumonia (hospital-acquired pneumonia, HAP) is defined as pneumonia that develops ≥48 hours after hospital admission and was not incubating at the time of admission. A critically important subcategory is ventilator-associated pneumonia (VAP), defined as pneumonia arising ≥48–72 hours after endotracheal intubation. HAP and VAP constitute the most common hospital-acquired infections in intensive care units, accounting for up to 25% of all ICU infections and carrying a crude mortality of 20–50% depending on the organism and the severity of illness. The key microbiological distinction from CAP is the dominance of Gram-negative bacilli (particularly Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, and Acinetobacter baumannii) and, in some settings, methicillin-resistant Staphylococcus aureus (MRSA) — organisms that are rare in CAP but routine in HAP/VAP, and which require different antibiotic classes altogether.
Aspiration pneumonia arises when oropharyngeal secretions, gastric contents, or foreign material is aspirated into the lower airways in sufficient quantity to overwhelm the normal mucociliary and macrophage defences. It is distinct from aspiration pneumonitis (Mendelson syndrome), which is a chemical injury from gastric acid aspiration without bacterial infection and typically resolves without antibiotics. True aspiration pneumonia involves bacterial infection, predominantly with anaerobes (from the oral flora, particularly in patients with poor dental hygiene) and mixed oral flora. The right lower lobe is most commonly affected when aspiration occurs in the upright position (because of the relatively vertical course of the right main bronchus), while the right upper lobe and left lower lobe are more affected when aspiration occurs in the recumbent patient. The clinical distinction from CAP may be subtle — a history of impaired consciousness, dysphagia, or gastro-oesophageal reflux is often the key clue.
CAP vs HAP/VAP vs Aspiration Pneumonia
Microbiology of CAP: Typical and Atypical Pathogens
The microbiology of community-acquired pneumonia is one of the most clinically important topics in Internal Medicine because it directly governs empirical antibiotic selection. The organisms causing CAP are conventionally divided into two broad groups — typical (classical) bacterial pathogens and atypical pathogens — based on historical clinical presentations and, more practically, on whether they can be visualised on Gram stain and cultured on standard bacteriological media. While the distinction is somewhat imperfect in clinical practice (many patients have mixed or atypical presentations regardless of the pathogen), the classification remains the most widely used framework for rationalising antibiotic choice.
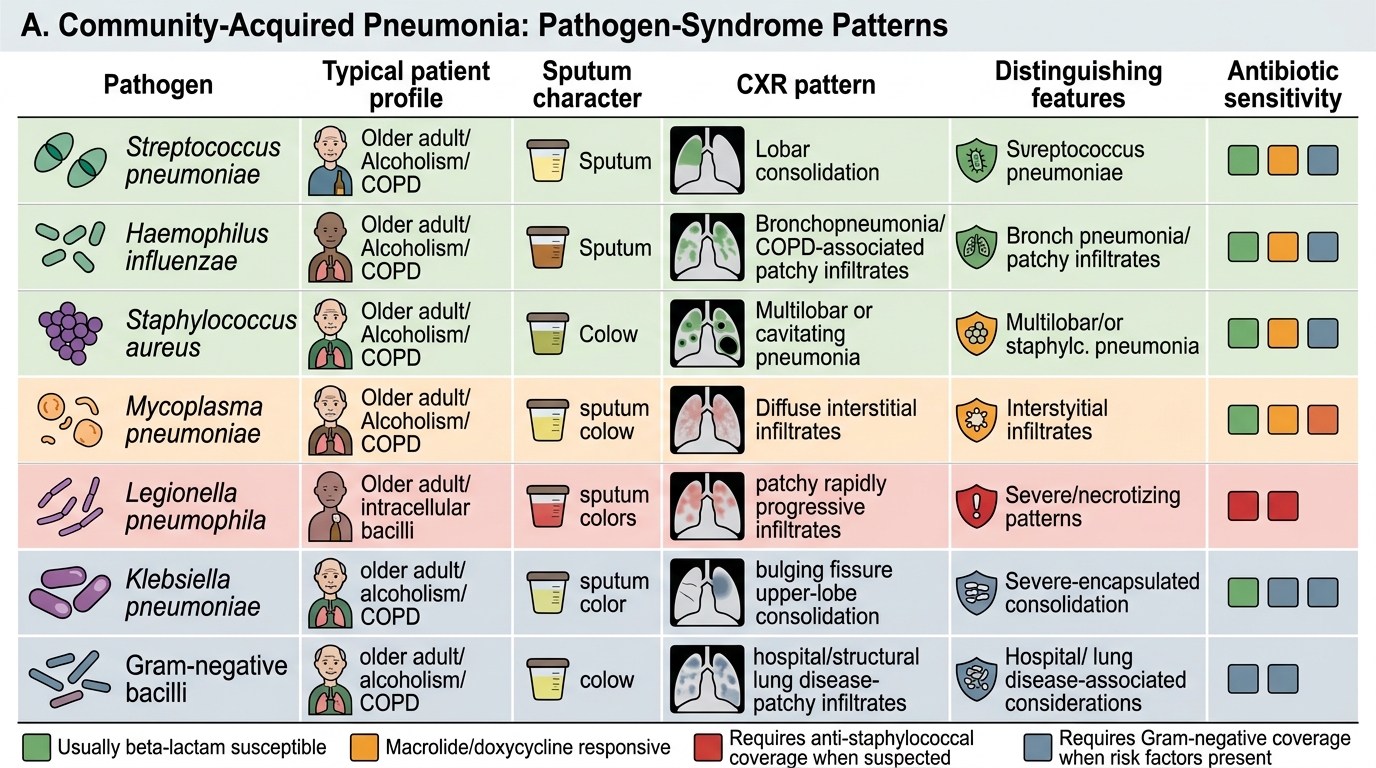
Streptococcus pneumoniae (the pneumococcus) is the single most common cause of CAP worldwide, accounting for 20–60% of cases requiring hospitalisation in most studies including Indian series. It produces the characteristic lobar pneumonia pattern on chest X-ray — dense, homogeneous consolidation filling an entire lobe or segment, with an air bronchogram sign — though this classical radiology is not invariably present. Clinically, pneumococcal CAP is typically acute in onset, with sudden-onset high fever (often with rigors), pleuritic chest pain, and rust-coloured (rusty) sputum produced by the lysis of red blood cells that extravasate into the alveoli along with the inflammatory exudate. The pneumococcus expresses a polysaccharide capsule that inhibits phagocytosis — the basis for the conjugate and polysaccharide pneumococcal vaccines. Complications include parapneumonic effusion, empyema, bacteraemia (present in 20–30% of hospitalised cases), and meningitis.
Haemophilus influenzae (non-typeable strains in adults with chronic lung disease; type b in unimmunised children) is the second most common cause of CAP, particularly in patients with COPD and other structural lung diseases where pre-existing mucociliary dysfunction and colonisation favour infection. The chest X-ray shows bronchopneumonia (patchy, bilateral, peribronchial infiltrates) rather than lobar consolidation. Staphylococcus aureus CAP is less common in adults except following influenza (where prior viral damage to the mucociliary escalator creates a portal for secondary bacterial invasion), in intravenous drug users, and in patients with necrotising pneumonia — where multiple cavities and pneumatoceles form rapidly, often with empyema and septicaemia.
The atypical pathogens — so named because they were originally identified in patients who did not respond to penicillin and had a clinical syndrome milder than expected — include Mycoplasma pneumoniae, Chlamydophila pneumoniae (formerly Chlamydia pneumoniae), and Legionella pneumophila. Mycoplasma is the most common atypical pathogen in younger adults and is characterised by a gradual onset, a predominantly dry (non-productive) cough, extrapulmonary features (bullous myringitis, cold agglutinins causing haemolytic anaemia, Stevens-Johnson syndrome in severe cases), and a relatively benign clinical course — the 'walking pneumonia' presentation, where the patient feels moderately unwell but remains ambulatory. Chlamydophila pneumoniae has a similar clinical profile to Mycoplasma, often with pharyngitis or laryngitis preceding the lower respiratory infection. Legionella pneumophila is the most dangerous atypical pathogen, producing Legionnaires' disease — a severe pneumonia with prominent extrapulmonary features (hyponatraemia, abnormal liver function, haematuria, altered consciousness) and a radiological pattern of bilateral patchy infiltrates that progress rapidly; it is associated with contaminated water sources (cooling towers, hospital water systems, air conditioning) and carries a mortality of 5–30% even with treatment. Legionella cannot be grown on standard bacteriological media — it requires specialised BCYE (buffered charcoal yeast extract) agar — and is often diagnosed by urinary antigen testing.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
CAP Pathogen-Syndrome Patterns
Microbiology of HAP, VAP, and Aspiration Pneumonia
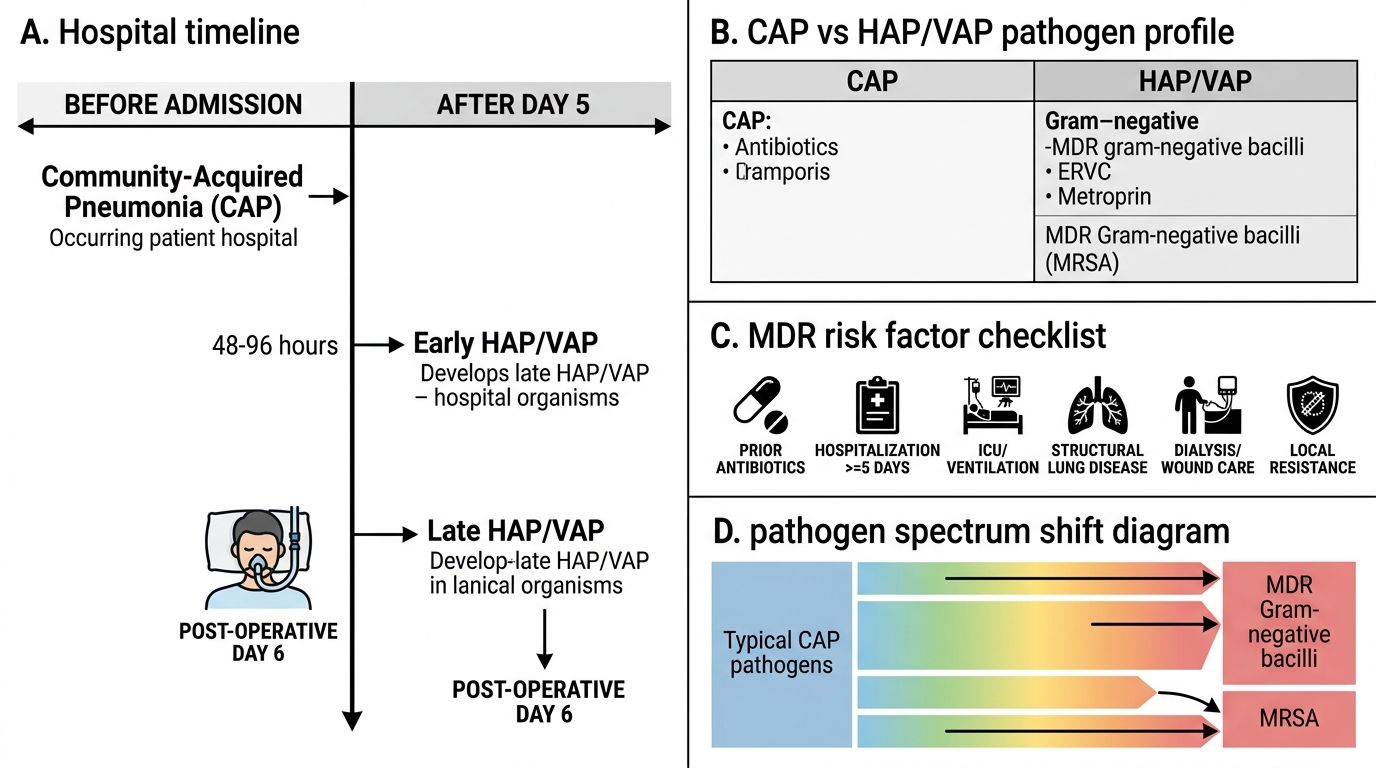
Hospital-acquired pneumonia and ventilator-associated pneumonia present the clinician with a fundamentally different microbiological landscape from CAP, shaped by three forces: the selection pressure of prior antibiotic use, the colonisation of the oropharynx with hospital-environment organisms during prolonged hospitalisation, and the impairment of normal host defences by the underlying illness and invasive procedures. Understanding this shift from community to hospital flora is essential for every clinician who works in any inpatient setting, because the empirical antibiotic choice that saves a life in CAP will fail to cover the pathogens responsible for HAP.
In patients who develop HAP or VAP ≥5 days after admission (late-onset HAP/VAP), or in patients with known risk factors for multidrug-resistant (MDR) organisms (prior antibiotic therapy within 90 days, hospitalisation ≥2 days within 90 days, residence in a nursing home, home infusion therapy, chronic dialysis, wound care), the responsible pathogens are predominantly Gram-negative bacilli: Pseudomonas aeruginosa, Klebsiella pneumoniae (including extended-spectrum beta-lactamase-producing and carbapenem-resistant strains), Acinetobacter baumannii, Escherichia coli, and Enterobacter species. Pseudomonas is particularly important because it has intrinsic resistance to many antibiotics and requires anti-pseudomonal agents (piperacillin-tazobactam, cefepime, carbapenem, or an aminoglycoside in combination). MRSA must be considered in patients from settings with high MRSA prevalence, those with recent skin or soft tissue MRSA infection, and those with severe HAP/VAP in regions where community MRSA is endemic; vancomycin or linezolid is required for confirmed or strongly suspected MRSA pneumonia.
Early-onset HAP/VAP (within 4 days of admission) in patients without risk factors for MDR organisms is more likely caused by organisms similar to those in CAP — S. pneumoniae, H. influenzae, methicillin-sensitive S. aureus (MSSA) — and can be treated with narrower-spectrum agents. However, early-onset HAP/VAP in a patient who has received antibiotics within the past 90 days should still be treated as potentially MDR.
Aspiration pneumonia microbiology reflects the oral flora of the aspirating patient. In community-dwelling patients with poor dental hygiene, anaerobes (Bacteroides species, Fusobacterium nucleatum, Peptostreptococcus species) predominate, often in a polymicrobial mix. The clinical presentation is often subacute, with a week or more of low-grade fever, productive cough, and weight loss, and the radiological pattern is a gravity-dependent infiltrate — classically the right lower lobe in upright aspiration (along the path of the right main bronchus, which is shorter and more vertical) or the posterior segments of the upper lobes and superior segments of the lower lobes in supine aspiration. In hospitalised patients who aspirate, oral flora is supplemented by hospital Gram-negative organisms, increasing the risk of a more virulent and antibiotic-resistant infection.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
CAP vs HAP/VAP Pathogen Profiles and MDR Risk
SELF-CHECK
A 52-year-old man is admitted for elective bowel surgery. On post-operative day 6, he develops fever, purulent endotracheal secretions, and a new right-sided infiltrate on chest X-ray. He received amoxicillin-clavulanate prophylaxis on day 0. Which pathogen is MOST likely responsible?
A. Streptococcus pneumoniae
B. Mycoplasma pneumoniae
C. Pseudomonas aeruginosa
D. Legionella pneumophila
Reveal Answer
Answer: C. Pseudomonas aeruginosa
This is late-onset ventilator-associated pneumonia (VAP) — developing ≥48–72 hours after intubation, on day 6, with prior antibiotic exposure (amoxicillin-clavulanate is a risk factor for MDR organisms by clearing susceptible flora and selecting resistant organisms). In late-onset HAP/VAP with prior antibiotic exposure, Gram-negative bacilli — especially Pseudomonas aeruginosa — are the predominant concern. S. pneumoniae and Mycoplasma are primarily CAP pathogens, not late-onset HAP/VAP pathogens. Legionella causes a severe CAP associated with water sources, not post-surgical HAP.