Page 3 of 20
IM3.1-3 | Pneumonia Foundations — SDL Guide (Part 3)
Management Principles: Empirical Antibiotics and Supportive Care
The management of pneumonia begins before the pathogen is known — the empirical antibiotic choice is the most consequential immediate decision. The guiding principle is to choose an antibiotic that covers the most likely pathogens for the syndrome, the host, and the severity — while being as narrow-spectrum as evidence allows, to limit resistance selection and adverse effects. The empirical regimen is then reviewed at 48–72 hours when clinical response can be assessed and preliminary culture results may be available; at that point, either de-escalation (switching to a narrower agent if a susceptible pathogen is identified) or escalation (broadening cover if the patient has not improved) is appropriate.
For CAP managed as an outpatient (CURB-65 0–1): Oral amoxicillin (500 mg–1 g three times daily) is sufficient to cover pneumococcus and non-atypical pathogens in patients without risk factors for atypical infection. If atypical infection is likely (young patient, dry cough, walking pneumonia picture) or if the patient has a penicillin allergy, a macrolide (azithromycin or clarithromycin) is the preferred alternative, as it covers both typical streptococcal and atypical organisms. Respiratory fluoroquinolones (levofloxacin, moxifloxacin) cover both groups and are appropriate in patients with comorbidities (COPD, heart failure, immunosuppression) who require outpatient treatment.
For CAP requiring hospitalisation (CURB-65 2 or ≥3): The standard regimen is a beta-lactam plus a macrolide — intravenous co-amoxiclav (amoxicillin-clavulanate) or a third-generation cephalosporin (ceftriaxone) as the beta-lactam component, combined with azithromycin or clarithromycin as the macrolide component (to cover atypical pathogens). The rationale for dual therapy in hospitalised patients is that empirical monotherapy with a beta-lactam would leave atypical pathogens uncovered, and in severe CAP, untreated Legionella or Mycoplasma carries significant mortality. An alternative in penicillin-allergic patients or those with risk factors for resistant organisms is a respiratory fluoroquinolone monotherapy (levofloxacin or moxifloxacin), which has broad-spectrum activity covering all CAP pathogens including Legionella. For patients admitted to ICU with severe CAP, the regimen is typically IV ceftriaxone + IV azithromycin, or IV beta-lactam + IV fluoroquinolone; Legionella-specific coverage must be included in severe CAP requiring ICU admission.
For HAP/VAP: The initial empirical regimen must cover Gram-negative MDR organisms and MRSA. A typical regimen includes an anti-pseudomonal beta-lactam (piperacillin-tazobactam, cefepime, or a carbapenem in high-risk settings or carbapenem-resistant organism prevalence areas) ± an aminoglycoside or anti-pseudomonal fluoroquinolone for double Gram-negative cover. Vancomycin or linezolid is added when MRSA risk is present (prior MRSA colonisation/infection, high institutional MRSA prevalence, necrotising or cavitating pneumonia). De-escalation at 48–72 hours based on culture results is strongly encouraged to limit the ecological impact of broad-spectrum treatment.
Supportive therapy is an essential and often underappreciated component of pneumonia management. Supplemental oxygen should be titrated to maintain SpO2 ≥94% (≥88% in COPD patients to avoid hypercapnic respiratory failure — target lower). The mode of oxygen delivery escalates with severity: simple face mask for mild hypoxia; Venturi mask for more precise FiO2 in COPD; high-flow nasal cannula (HFNC) for moderate-severe hypoxaemic respiratory failure; non-invasive ventilation (NIV, BiPAP) for hypercapnic respiratory failure in COPD or immunocompromised patients where intubation risk is high; invasive mechanical ventilation for severe ARDS or failure of non-invasive support (SpO2 <88% on HFNC or NIV, worsening acidosis, altered consciousness). Intravenous fluids for hydration and haemodynamic support; vasopressors (noradrenaline first-line) for septic shock not responding to fluid resuscitation. The duration of antibiotic treatment: 5 days for non-severe CAP with clinical response; 7 days for severe CAP; 7–14 days for HAP/VAP (shorter with de-escalation if culture-negative or susceptible pathogen confirmed).
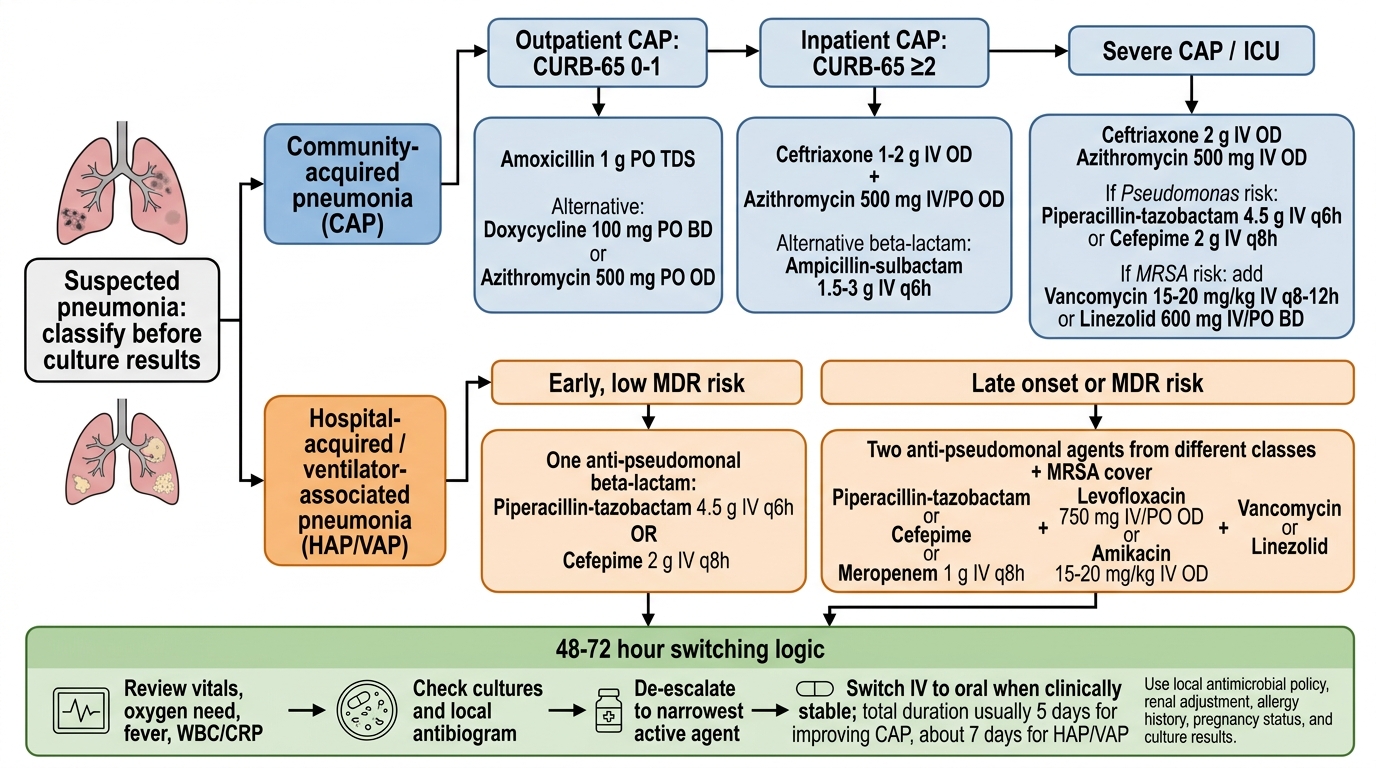
Empirical Antibiotic Algorithm for Pneumonia
Self-Assessment: Applying the Foundation Framework
Having established the three pneumonia syndromes, their microbiology, the pathogenesis and complication sequence, and the modifications imposed by host immune status, you are now equipped to apply this foundational framework to clinical scenarios. The ability to classify a pneumonia correctly at the bedside — before any culture result returns — is the cognitive skill that translates knowledge into action, and this is what the NMC competency framework (IM3.1–IM3.3) demands at the KH (Knowledge-applied-to-clinical-scenarios) level. The following scenarios test your ability to integrate the classification, microbiology, and host factors in a clinically realistic manner. For each scenario, determine the pneumonia category, the most likely pathogen(s), and the key clinical feature that discriminates this from alternative diagnoses. The reference table below summarises the three pneumonia syndromes for self-check.
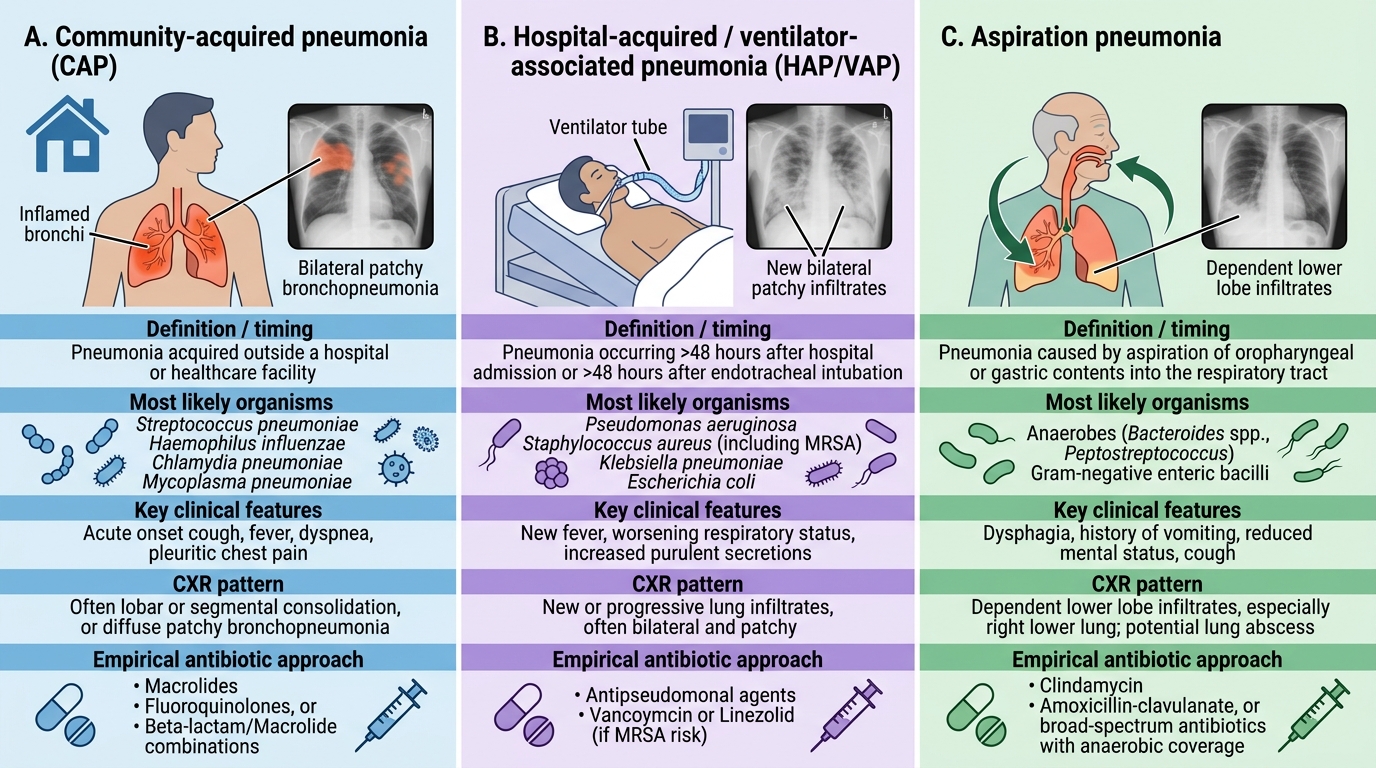
Pneumonia Syndromes: CAP vs HAP/VAP vs Aspiration
Scenario A: A 70-year-old retired civil servant with COPD (on inhaled steroids and LABA) presents with 4 days of worsening breathlessness, purulent yellow-green sputum, and fever. He was last admitted to hospital 8 months ago. SpO2 75% on room air. CXR: bilateral patchy infiltrates, no lobar consolidation.
Analysis: Acquired in the community (no hospitalisation within 90 days) = CAP. Underlying COPD = elevated risk for H. influenzae (second most common CAP pathogen in COPD patients due to pre-existing airway colonisation). Inhaled steroids = modest immunosuppression (increased risk of pneumonia from RCT data). The bilateral patchy pattern (bronchopneumonia pattern) is consistent with H. influenzae or atypical pathogen. Empirical treatment should cover H. influenzae (amoxicillin-clavulanate or a respiratory fluoroquinolone). CAP, likely H. influenzae or atypical pathogen.
Scenario B: A 55-year-old man with poorly controlled type 2 diabetes is admitted with sudden-onset right-lower-lobe consolidation, haemoptysis, and viscous blood-tinged sputum. He is febrile at 39.5°C. His chest X-ray shows a bulging horizontal fissure.
Analysis: Acquired in the community, diabetic host = classic Klebsiella pneumoniae CAP profile. The currant-jelly (blood-tinged, viscous) sputum and bulging fissure (from the large gelatinous exudate expanding the lobe) are pathognomonic clinical features of Klebsiella pneumonia. This has a high propensity for abscess formation and is associated with high morbidity in diabetics. Empirical treatment should include a third-generation cephalosporin or carbapenem, given the high-risk host.
Scenario C: A 62-year-old woman undergoes right hemicolectomy under general anaesthesia. She has chronic periodontal disease. On post-operative day 3, she develops fever and a right upper lobe opacity with an early air-fluid level visible on the PA chest X-ray.
Analysis: Pneumonia developed within 48 hours of admission in a patient likely colonised with oral flora pre-operatively. The gravity-dependent right upper lobe involvement (posterior segment) in a supine intubated patient, combined with periodontal disease, is classic aspiration pneumonia with an early abscess forming. Causative organisms: oral anaerobes (Bacteroides, Fusobacterium, Peptostreptococcus) ± aspiration of oral Gram-negative organisms. Treatment: amoxicillin-clavulanate (covers anaerobes and oral Gram-negatives) or clindamycin plus a fluoroquinolone in penicillin-allergic patients.
SELF-CHECK
Pneumonia developing 72 hours after intubation and mechanical ventilation is classified as:
A. Community-acquired pneumonia
B. Hospital-acquired pneumonia (HAP)
C. Ventilator-associated pneumonia (VAP)
D. Aspiration pneumonia
Reveal Answer
Answer: C. Ventilator-associated pneumonia (VAP)
Ventilator-associated pneumonia (VAP) is specifically defined as pneumonia developing ≥48–72 hours after endotracheal intubation. HAP refers to pneumonia ≥48 hours after hospital admission in non-ventilated patients. CAP requires acquisition outside the hospital or within the first 48 hours. While aspiration is often the mechanism of VAP (aspiration of oropharyngeal secretions around the endotracheal tube cuff), the correct classification when ventilated is VAP — a subtype of HAP with its own pathogen profile and management implications.
CLINICAL PEARL
The most dangerous pitfall in pneumonia management is treating every pneumonia with the same antibiotic regimen. The classification — CAP, HAP/VAP, or aspiration — is not a formality; it determines the entire empirical antibiotic strategy. CAP empirical therapy targets pneumococcus, H. influenzae, and atypical organisms (beta-lactam ± macrolide, or respiratory fluoroquinolone). HAP/VAP empirical therapy must cover Pseudomonas and other Gram-negative MDR organisms (anti-pseudomonal beta-lactam ± aminoglycoside or fluoroquinolone, ± vancomycin/linezolid if MRSA risk). Aspiration pneumonia targets anaerobes and oral flora (amoxicillin-clavulanate or clindamycin-based regimen). Starting a penicillin G alone for what is actually Pseudomonas HAP will result in clinical deterioration within 24–48 hours. Conversely, using broad-spectrum carbapenems for straightforward CAP in a healthy adult contributes to antibiotic resistance without improving outcomes. The three-question framework — where acquired, who is the host, what immune status — applied in the first clinical contact, is the safeguard against both failure and overtreatment.