Page 11 of 21
IM4.{13,15-17} | Febrile Syndrome Investigations — SDL Guide
Learning Objectives
- Order and interpret diagnostic tests for febrile syndromes based on the differential diagnosis, including CBC with differential, peripheral smear, urinalysis, chest X-ray and imaging, blood and urine cultures, sputum AFB, CSF analysis, body fluid analysis, stool examination, serology, FNAC, and bone marrow examination
- Observe and assist in the performance of a bone marrow aspiration and biopsy in a simulated environment, understanding the indications, technique, and interpretation of findings
- Enumerate the indications for imaging in the diagnosis of febrile syndromes
- Interpret a Mantoux (PPD) test in a given patient, including measurement, interpretation by reaction size, and adjustment for immune status
INSTRUCTIONS
Investigations in fever are powerful only when ordered on a targeted hypothesis — a shotgun panel generates false positives, delays diagnosis, and wastes resources. This module teaches you how to select, perform, and interpret investigations for febrile syndromes systematically, with emphasis on the peripheral blood smear, bone marrow, Mantoux test, and imaging indications.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 10–11 — Fever investigations (textbook)
- API Textbook of Medicine, 10th ed., Ch. 4 — Investigation of fever (textbook)
- NTEP (National Tuberculosis Elimination Programme) Operational Guidelines 2022 — Mantoux and IGRA use (guideline)
- Dacie and Lewis Practical Haematology, 12th ed., Ch. 5 — Bone marrow aspiration (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A peripheral blood smear reported as 'occasional ring forms seen, query malaria' is on your desk. The patient is a 32-year-old woman from Odisha, day 6 of fever, now confused with a serum creatinine of 2.8 mg/dL. The smear is the most important piece of paper in front of you — it tells you the species (ring form morphology, gametocyte shape), the parasite density (percentage of red cells infected), and the presence of features that define severity. Getting this interpretation right determines whether she receives oral chloroquine and goes home, or IV artesunate and goes to the intensive care unit. This single investigation, if interpreted with skill, can save her life. The broader principle — that every investigation in a febrile patient must be ordered with a specific question in mind and interpreted with specific knowledge of what each finding means clinically — is the foundation of this module.
WHY THIS MATTERS
The investigation of febrile syndromes is the most frequently performed set of clinical tasks in Indian general medicine wards. Every intern on every night call will be asked to interpret a CBC in a febrile patient, read a blood smear report, explain a Mantoux result, decide whether a chest X-ray finding is relevant, and justify an imaging request. The NMC competencies IM4.13, IM4.15, IM4.16, and IM4.17 span the full investigation skill set — from first-line blood tests to invasive bone marrow biopsy to radiological investigations. This module gives you the interpretive framework to use these investigations confidently and accurately.
RECALL
Recall the broad diagnostic categories of febrile illness: infectious (bacterial, viral, parasitic, fungal), inflammatory/autoimmune, malignant, and miscellaneous. Each category generates a characteristic pattern on routine investigations. Bacterial infection produces a leucocytosis with neutrophilia and elevated CRP; viral infection tends to produce a relative lymphocytosis, normal or low WBC, and mildly elevated CRP; malaria produces haemolytic anaemia, thrombocytopaenia, and the pathognomonic finding of intraerythrocytic parasites on blood smear; lymphoma and other malignancies may produce cytopenia (marrow infiltration), elevated LDH, and abnormal cells on peripheral smear; TB classically produces a normal or low WBC (lymphopenia) with a very high ESR. Also recall that the Mantoux (tuberculin skin test) measures delayed-type (Type IV) hypersensitivity to purified protein derivative (PPD) of Mycobacterium tuberculosis — it detects immunological sensitisation, not active infection, and is affected by BCG vaccination, malnutrition, and immunosuppression.
Clinical Indication for Investigations in Febrile Syndromes
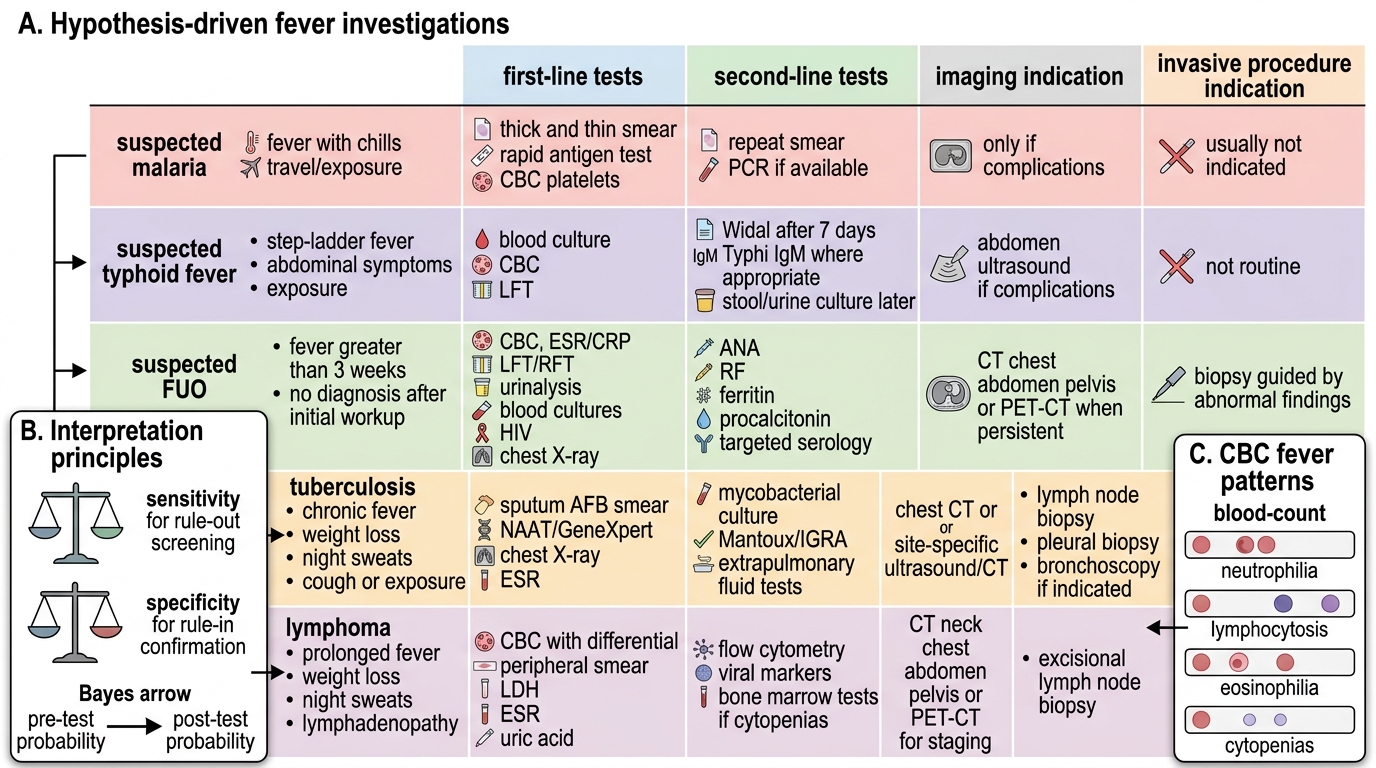
The cardinal principle governing investigation of febrile syndromes is that every test must be ordered to answer a specific diagnostic question generated by the clinical assessment — not as a reflex. Indiscriminate ordering of comprehensive panels generates false positives (a weakly positive Widal test in a patient with typhoid-free probability is misleading), wastes resources in resource-limited settings, and delays the diagnosis by flooding the clinician with irrelevant data. This governing principle — hypothesis-driven investigation — distinguishes the competent clinician from the reflexive one.
The indications for specific investigations are derived from the ranked differential diagnosis generated by the clinical evaluation. If the differential after history and examination is (1) falciparum malaria, (2) enteric fever, (3) dengue, then the investigation panel should include: peripheral blood smear and malaria RDT (for malaria), blood cultures × 3 sets (for typhoid — highest yield in the first week), CBC with differential and dengue NS1/IgM (for dengue) — in that priority order. Adding a bone marrow biopsy to this panel would be inappropriate; adding IGRA for TB would be low-yield in this presentation. By contrast, in a patient with 6 weeks of fever, weight loss, and generalised lymphadenopathy where lymphoma is the lead hypothesis, blood culture and malaria smear are lower priority than lymph node biopsy, LDH, uric acid, CT chest/abdomen, and bone marrow biopsy.
The NMC competency IM4.16 requires enumeration of the indications for imaging in febrile syndromes. These are: (1) localising a focus of infection (chest X-ray for pneumonia/TB, ultrasound abdomen for amoebic liver abscess/pyelonephritis/splenomegaly characterisation/ascites, CT head for cerebral abscess/encephalitis); (2) characterising organomegaly or lymphadenopathy identified clinically (CT abdomen/pelvis or PET-CT for lymphoma staging); (3) identifying structural lesions relevant to the differential (echocardiography for infective endocarditis or cardiac myxoma); (4) guiding invasive procedures (ultrasound-guided liver abscess drainage, CT-guided lymph node biopsy); (5) monitoring response to treatment (serial chest X-rays in TB, serial CTs in pyogenic abscess). The clinical question determines the modality and the urgency.
Hypothesis-Driven Fever Investigation Matrix
Governing Principles: Investigation Interpretation Framework
The governing principles for interpreting investigations in febrile syndromes are built around two concepts: (1) sensitivity and specificity of the test in the clinical context — a highly sensitive test screens (high negative predictive value; negative result rules out the diagnosis); a highly specific test confirms (high positive predictive value; positive result rules in the diagnosis); and (2) pre-test probability — the post-test probability of a diagnosis after a test result depends heavily on how likely the diagnosis was before the test was ordered (Bayes' theorem). A weakly positive Widal test in a patient with 2 days of fever and no epidemiological risk for typhoid is far less clinically significant than the same result in a patient with step-ladder fever, relative bradycardia, and travel from North India.
The complete blood count (CBC) with differential in fever reveals four clinically important patterns: (a) leucocytosis with neutrophilia (WBC >11,000, neutrophils >75%) — indicates acute bacterial infection (pneumonia, pyelonephritis, bacterial meningitis, sepsis) or a physiological stress response; left shift (increase in band neutrophils >10% or presence of metamyelocytes on the smear) indicates active granulopoiesis driven by severe or acute bacterial infection; (b) leucopaenia (WBC <4,000) — indicates viral infection (typhoid characteristically, dengue, HIV, influenza), overwhelming bacterial infection (gram-negative sepsis causing bone marrow suppression), or hypersplenism; (c) relative lymphocytosis — viral infection, TB (relative lymphocytosis is common in TB even when the WBC is normal); (d) thrombocytopaenia (platelets <150,000) — dengue (immune-mediated platelet destruction; a falling platelet count in dengue is a warning sign by WHO 2009 criteria); malaria (P. falciparum); sepsis with DIC; kala-azar (hypersplenism); lymphoma (bone marrow infiltration). Eosinophilia (>500 eosinophils/mm³) in a febrile patient with tissue-invasion signs suggests parasitic infection (Toxocara, strongyloidosis, trichinella, visceral larva migrans), drug reaction, or Löffler syndrome (transient pulmonary infiltrates from migrating larvae).
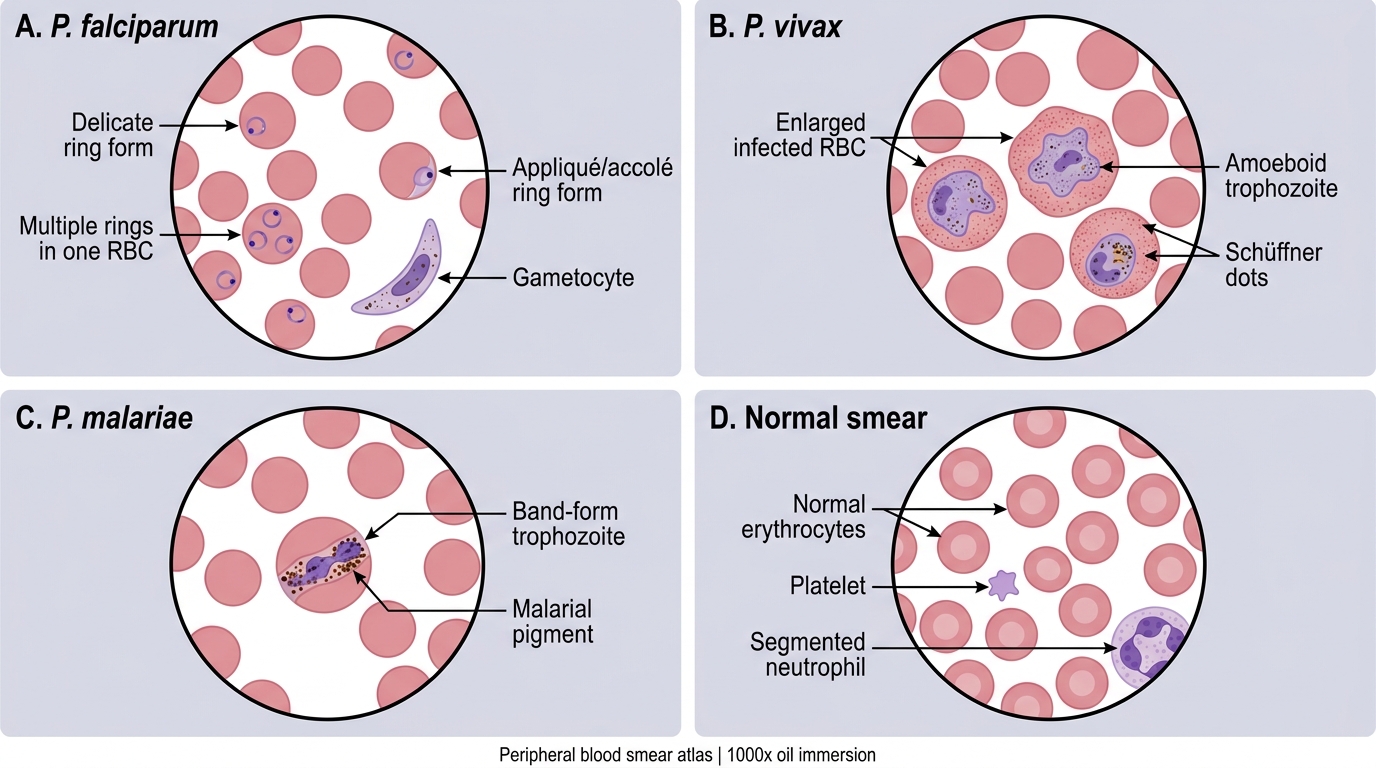
The peripheral blood smear in fever has specific diagnostic applications beyond its role in the CBC. For malaria diagnosis: thin and thick smear prepared from finger-prick blood; thick smear is more sensitive (concentrates parasites); thin smear provides morphological detail for species identification and density counting. Key species-specific features: P. vivax — large ring forms, amoeboid trophozoites, Schüffner dots on infected erythrocytes (which are enlarged), and characteristic gametocytes; P. falciparum — small ring forms with multiple rings per cell (2 or more per erythrocyte = high density characteristic of falciparum), appliqué (accolé) forms at the cell margin, and banana-shaped macrogametocytes (pathognomonic of P. falciparum — no other Plasmodium species has banana-shaped gametocytes); P. malariae — compact band-form (ribbon-form) trophozoites crossing the cell, rosette schizonts, infected erythrocytes NOT enlarged. Parasite density is expressed as percentage of infected red cells or parasites per microlitre; density ≥5% = hyperparasitaemia = one criterion for severe falciparum malaria (WHO criteria).
The quantitative buffy coat (QBC) technique for malaria uses acridine orange staining of the buffy coat layer in a capillary tube under UV fluorescence to detect fluorescent parasites; it is more sensitive than thick smear but less useful for species identification and density counting.
Peripheral Blood Smear Atlas of Malaria Species
Procedure: Key Investigations in Febrile Syndromes
This section covers the procedural and technical aspects of the key investigations that define clinical competency in febrile syndrome workup. For each investigation, the focus is on how to perform or obtain it correctly, the factors that affect quality, and the parameters to report.
Blood culture — technique for maximum yield: Three sets of blood cultures, each set consisting of one aerobic and one anaerobic bottle, drawn from different venepuncture sites at intervals of 20–30 minutes. The timing of collection relative to fever is less important than the total volume of blood collected — the single most important determinant of blood culture sensitivity is volume: 10 mL per bottle (20 mL per set, 60 mL total for 3 sets). Common errors that reduce yield: (1) inadequate skin decontamination (use chlorhexidine 2% or povidone-iodine + alcohol in two steps, allowing to dry before needle insertion); (2) insufficient blood volume (most common cause of false-negative cultures); (3) prior antibiotic administration (reduces sensitivity by 40–50% for common organisms). For Brucella and Bartonella, blood cultures should be held for 4–6 weeks with subcultures. For fungal endocarditis, Candida grows on standard media but Aspergillus does NOT grow on blood culture — serum galactomannan and beta-glucan are needed.
Urine culture — technique and interpretation: Midstream clean-catch specimen (or catheter specimen in immobile patients). Significant bacteriuria is defined as ≥10⁵ colony-forming units/mL of a single organism in a symptomatic patient (lower counts — ≥10³ in a catheterised patient — may also be significant). Urinalysis should include: specific gravity, pH, leucocyte esterase (positive = pyuria), nitrite (positive = gram-negative nitrate-reducing organisms), protein, glucose, and microscopy for leucocytes (>10/hpf = pyuria), bacteria, casts (leucocyte casts = pyelonephritis; granular casts = ATN).
Sputum AFB smear and culture for TB diagnosis: For pulmonary TB suspicion, collect two sputum specimens (early morning first specimen, and spot specimen) for ZN (Ziehl-Neelsen) smear microscopy and culture. Quality of the specimen matters — saliva rather than mucus has fewer bacilli and is less useful; the specimen should be mucopurulent, 5–10 mL, coughed deeply. Smear grading: negative (no AFB on full smear), scanty (1–9 AFB per 100 fields), 1+ (10–99 AFB per 100 fields), 2+ (1–10 per field), 3+ (>10 per field). Sensitivity of ZN smear for pulmonary TB is 45–70% in smear-positive TB (much lower in paucibacillary TB, extrapulmonary TB). NTEP now recommends CBNAAT (cartridge-based nucleic acid amplification test — Xpert MTB/RIF) as the primary diagnostic test for pulmonary and extrapulmonary TB — it detects M. tuberculosis DNA and simultaneously detects rifampicin resistance with a turnaround time of 2 hours.
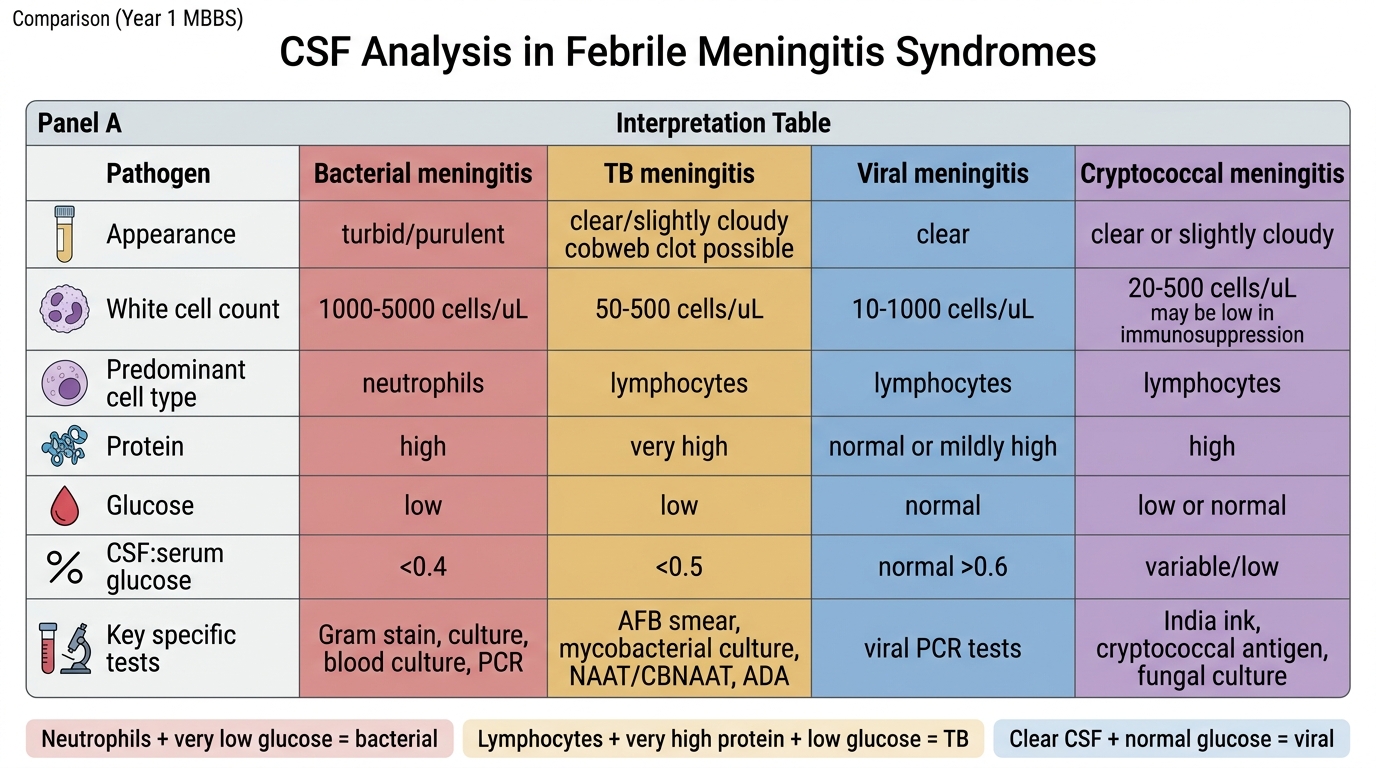
CSF analysis in febrile illness: Lumbar puncture is indicated when fever is accompanied by headache and signs of meningeal irritation (stiff neck, Kernig sign, Brudzinski sign) or altered consciousness, after fundoscopy has excluded papilloedema (which contraindicates LP until CT head is done to exclude a space-occupying lesion with raised ICP). CSF findings in the four main causes of acute meningitis:
- Bacterial meningitis: turbid CSF, WBC >1000 with >80% neutrophils, protein >100 mg/dL, glucose <40 mg/dL (CSF:serum glucose ratio <0.5), positive Gram stain in 50–70%, positive culture in 70–80%.
- Tuberculous meningitis: clear/xanthochromic CSF, WBC 100–500 with lymphocytic predominance, protein markedly elevated (100–500 mg/dL), glucose low (CSF:serum ratio <0.5), AFB smear positive in <20%, culture positive in 40–80% (gold standard), ADA (adenosine deaminase) elevated >10 U/L is supportive.
- Viral meningitis/encephalitis: clear CSF, WBC 10–500 with lymphocytic predominance, protein mildly elevated, glucose normal.
- Cryptococcal meningitis (in HIV patients): clear or turbid CSF, WBC variable (may be paradoxically low in severe immunosuppression), India ink preparation positive in 50–80%, cryptococcal antigen (CrAg) positive in >95%.
Pleural and body fluid analysis follows the Light criteria for exudate vs transudate: pleural protein >3 g/dL, pleural:serum protein ratio >0.5, pleural:serum LDH ratio >0.6 = exudate. Lymphocytic exudative pleural effusion with high ADA (>40 U/L) in a febrile patient with constitutional symptoms strongly suggests TB pleuritis — Abram's needle pleural biopsy for histology and culture adds sensitivity.
CSF Analysis in Febrile Meningitis Syndromes
SELF-CHECK
A peripheral blood smear from a 28-year-old with 5 days of fever, rigors, and a haemoglobin of 7.2 g/dL (from Odisha) shows: multiple small ring-form trophozoites within individual red blood cells, some erythrocytes containing 2–3 ring forms, and occasional elongated crescent-shaped forms. The red cells are NOT enlarged. What is the Plasmodium species, and what feature is pathognomonic?
A. P. vivax — pathognomonic feature: enlarged infected erythrocytes with Schüffner dots
B. P. malariae — pathognomonic feature: band-form trophozoites crossing the cell
C. P. falciparum — pathognomonic feature: banana-shaped (crescent) gametocytes
D. P. ovale — pathognomonic feature: oval-fimbriated infected erythrocytes
Reveal Answer
Answer: C. P. falciparum — pathognomonic feature: banana-shaped (crescent) gametocytes
The findings on the smear — small ring forms, multiple rings per erythrocyte (≥2 rings in one cell), infected erythrocytes NOT enlarged, and elongated crescent/banana-shaped forms — are characteristic of Plasmodium falciparum. The pathognomonic feature is the banana-shaped (crescent-shaped) macrogametocyte, which is specific to P. falciparum — no other Plasmodium species produces this gametocyte morphology. P. vivax infected erythrocytes are enlarged and show Schüffner dots; P. malariae shows band-form trophozoites and non-enlarged erythrocytes but NO banana gametocytes; P. ovale shows fimbriated oval erythrocytes.