Page 2 of 21
IM4.1-8 | Fever Foundations — SDL Guide (Part 2)
The Febrile Response in Special Populations
The febrile response is not uniform across all patients. Host immune status, age, comorbidities, and physiological state substantially modify both the magnitude of the febrile response and its reliability as a clinical indicator. Understanding these modifications is a core competency (IM4.1) because they determine when the absence of fever is as alarming as its presence, and when fever patterns must be interpreted differently from the standard adult norm.
Elderly patients (age >65 years) often mount a blunted or absent febrile response to serious infection. The reasons are multifactorial: reduced baseline hypothalamic sensitivity to prostaglandins, impaired cytokine production by aged macrophages, lower baseline body temperature (which means a temperature of 37.5°C may represent significant pyrexia in an elder whose baseline is 36.1°C), and concurrent antipyretic use for arthritis. This clinical trap is dangerous because an elderly patient with pneumococcal bacteraemia or urinary sepsis may present with confusion, falls, or functional decline without fever — and the temperature may read 37.8°C when a 25-year-old with the same infection would be at 40°C. Any acute deterioration in an elderly patient warrants sepsis evaluation regardless of the temperature reading.
Immunosuppressed patients — those receiving systemic corticosteroids (which suppress both cytokine production and PGE2 synthesis), chemotherapy, biological agents (TNF inhibitors, IL-6 inhibitors), or solid organ transplant immunosuppression — can also mount a blunted febrile response. TNF inhibitors such as infliximab and adalimumab suppress one of the key endogenous pyrogens directly. IL-6 receptor blockers (tocilizumab) prevent the hypothalamic signal and can completely ablate fever even in the setting of severe sepsis. In a patient on tocilizumab, a temperature of 37.8°C may indicate bacteraemia that would produce 40°C in an immunocompetent host; CRP and procalcitonin (which depend partly on IL-6) will also be suppressed, making laboratory diagnosis harder.
Neutropenic patients (absolute neutrophil count <500 cells/mm³, typically post-chemotherapy) require a different fever threshold: even a single temperature reading of 38.3°C (or two readings of 38°C one hour apart) in the context of neutropenia constitutes febrile neutropenia, a medical emergency requiring immediate broad-spectrum intravenous antibiotics within one hour. The risk of bacteraemia from gut flora translocation is markedly elevated when mucosal barriers are breached by chemotherapy, and delays of even a few hours measurably increase mortality.
Patients with HIV have a complex febrile landscape that changes with CD4 count. At CD4 >500 cells/mm³ the pattern resembles that of the immunocompetent host. As CD4 declines below 200 cells/mm³, opportunistic infections dominate: Pneumocystis jirovecii pneumonia (PJP), disseminated Mycobacterium avium complex (MAC), cryptococcal meningitis, CMV disease, and disseminated histoplasmosis in endemic areas. TB can occur at any CD4 count but disseminated TB becomes more likely at CD4 <200. An important India-specific consideration: because TB is so prevalent, TB-HIV co-infection accounts for a large proportion of prolonged fever in HIV-positive patients presenting to Indian hospitals, and NTEP guidelines mandate TB screening in all HIV-positive patients.
Travellers deserve special mention given India's internal mobility. A patient who has returned from Odisha to Chennai may have acquired falciparum malaria; a traveller from Bihar may have kala-azar; a pilgrim returning from the Kumbh Mela may have acquired enteric fever or cholera. Travel history must be documented in every febrile patient, with specific enquiry about forest exposure (malaria, scrub typhus), flood exposure (leptospirosis), and animal contact (brucellosis, rickettsial infections).
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
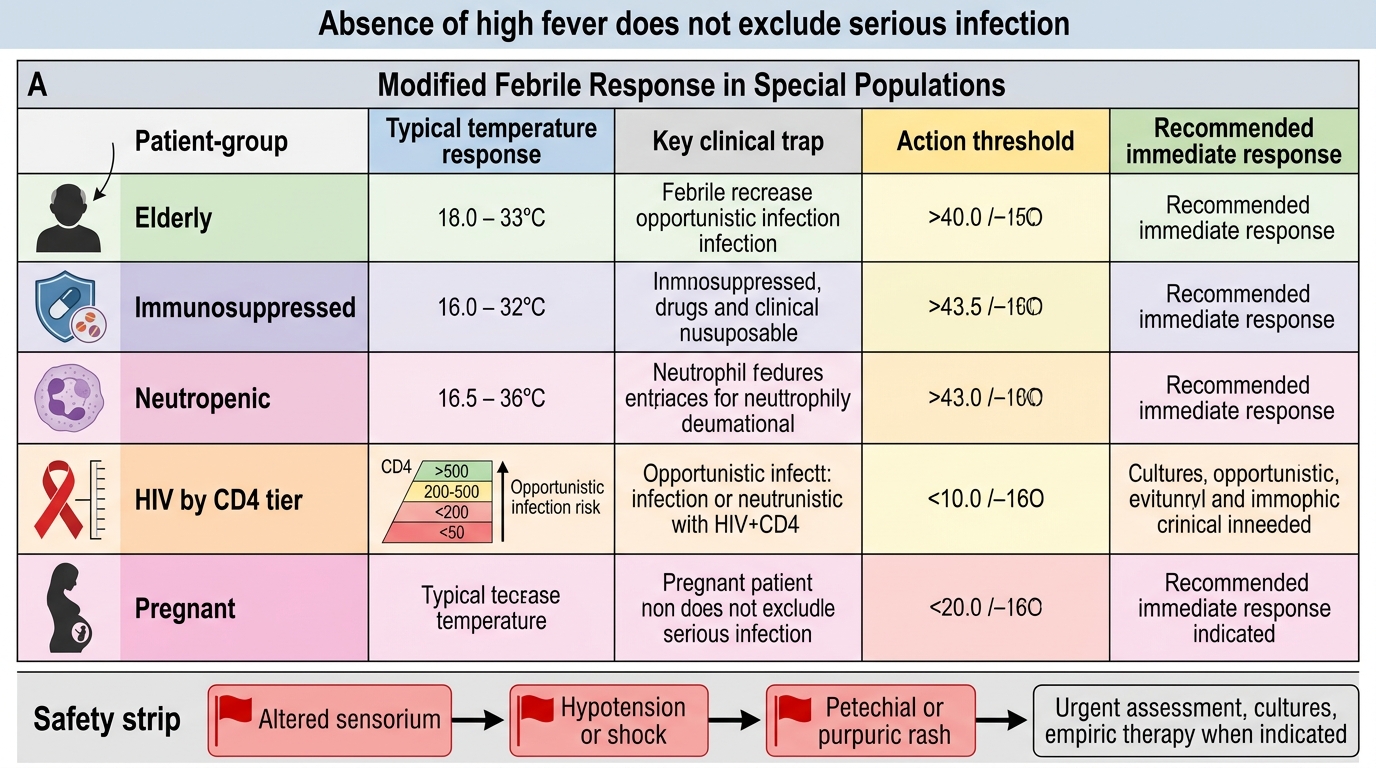
Modified Fever Response in Special Populations
Approach to the Patient with Acute Febrile Illness
The approach to a patient presenting with acute fever is a structured clinical exercise in which history, examination, and targeted investigation combine to generate a probability-ranked differential diagnosis. This approach, defined by NMC competency IM4.6, requires both a systematic framework and the ability to recognise immediately life-threatening presentations that warrant resuscitation before complete workup.
The first priority in any febrile patient is immediate danger-sign recognition — the identification of features indicating severe illness or imminent deterioration that requires urgent action. These danger signs are: altered sensorium or confusion (which, combined with fever, raises the differential of meningitis, cerebral malaria, encephalitis, severe sepsis, or heat stroke — all requiring urgent assessment); hypotension (systolic <90 mmHg or MAP <65 mmHg) or tachycardia disproportionate to fever; rash that is petechial or purpuric (suggests meningococcaemia, rickettsial disease, or dengue haemorrhagic fever); signs of bleeding (haematemesis, melaena, haemoptysis, petechiae — dengue, leptospirosis, viral haemorrhagic fever); seizures; respiratory distress (hypoxia); severe dehydration; and jaundice with encephalopathy (acute liver failure from viral hepatitis or leptospirosis). Any of these signs requires concurrent assessment and resuscitation rather than a sequential history-first approach.
For patients without immediate danger signs, a systematic history should be obtained with the following structured enquiry: (1) Fever characterisation — onset (sudden vs gradual), duration, temperature readings at home, pattern (continuous, remittent, intermittent, quotidian, tertian, quartan), response to antipyretics, rigor or chills pattern (whether rigors are frank shaking or just chills). (2) Associated symptoms — headache and neck stiffness (meningism), cough and sputum (respiratory focus), dysuria and frequency (urinary focus), abdominal pain and diarrhoea (enteric), jaundice (hepatobiliary), rash (viral, rickettsial, immune), joint pain and swelling (inflammatory or infectious arthritis), lymphadenopathy. (3) Epidemiological history — travel (domestic and international, forest exposure, flood exposure), occupation (agricultural worker, healthcare worker, abattoir worker, sewer worker), animal contacts (livestock, dogs — leptospirosis, brucellosis), sexual history (STIs, HIV), recent procedures (dental, surgical — endocarditis risk), vaccination status (typhoid, hepatitis A, hepatitis B). (4) Drug history — all current medications, herbal remedies (hepatotoxicity), recent antibiotics (may mask culture results or cause CDAD). (5) Comorbidities and immune status — diabetes (worse outcomes with skin and urinary infections, diabetic foot), HIV status, CKD, cirrhosis, malignancy, immunosuppressive therapy.
Examination should follow the pattern described for IM4.11 (covered in detail in the skills SDL): general inspection including skin and mucosal survey, lymph node survey, chest and abdominal examination with special attention to liver and spleen size, and a neurological screen including fundoscopy for papilloedema in any febrile patient with headache.
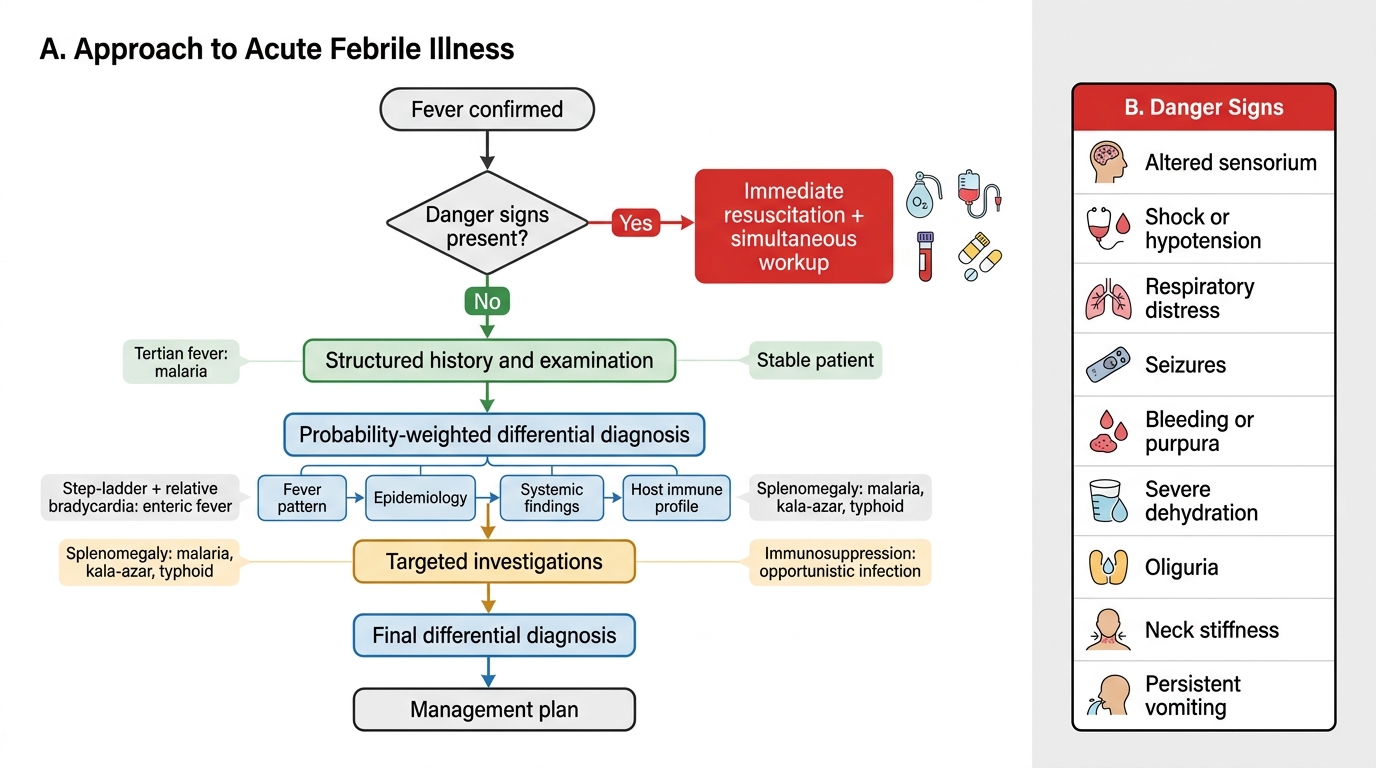
Approach to Acute Febrile Illness
The generation of a differential diagnosis should be probability-weighted by integrating four dimensions: (1) the fever pattern (intermittent tertian fever favours malaria; step-ladder fever with relative bradycardia favours enteric fever; quotidian double-spike favours Still's disease; continuous fever with minimal diurnal variation favours bacterial infection or TB), (2) the epidemiological profile (region, season, occupation, travel), (3) the accompanying systemic findings (splenomegaly: malaria, kala-azar, typhoid, brucellosis; hepatomegaly: viral hepatitis, amoebic liver abscess; lymphadenopathy: lymphoma, infectious mononucleosis, HIV, TB), and (4) the host immune profile. A prioritised differential diagnosis (most dangerous first, most likely first, most treatable first) should be formulated before ordering investigations, so that the investigation panel is targeted rather than reflexively comprehensive.
Sepsis Syndrome: Pathophysiology, Clinical Features, and Management
Sepsis is the most life-threatening manifestation of the febrile syndromes and warrants dedicated attention as a competency (IM4.7). The current definition — Sepsis-3 (Singer et al., JAMA 2016) — defines sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection, identified clinically by an acute increase in the SOFA score of ≥2 points in the context of infection. The older term SIRS (systemic inflammatory response syndrome) — defined as two or more of: temperature >38°C or <36°C, heart rate >90 bpm, respiratory rate >20 breaths/min or PaCO₂ <32 mmHg, WBC >12,000 or <4,000 or >10% bands — is no longer the required criterion but remains clinically useful for identifying early physiological perturbation. Septic shock is defined within Sepsis-3 as a subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are severe enough to substantially increase mortality; clinically identified as a MAP <65 mmHg requiring vasopressors despite adequate fluid resuscitation, with serum lactate >2 mmol/L in the absence of hypovolaemia.
The pathophysiology of sepsis is a dysregulated cytokine storm that progresses through four overlapping phases. In the hyper-inflammatory phase, the pattern-recognition receptor activation described above generates a massive systemic cytokine release — the so-called cytokine storm of TNF-α, IL-1β, IL-6, and IL-8. These cytokines cause widespread endothelial activation, upregulating adhesion molecules and increasing vascular permeability (capillary leak), which manifests as distributive shock (warm, vasodilated peripheries with low SVR in the early phase). Simultaneously, tissue factor expression on activated monocytes initiates disseminated intravascular coagulation (DIC) through the extrinsic coagulation pathway, leading to microvascular thrombi in end-organs even as systemic coagulation factors are consumed. In the organ dysfunction phase, the combination of microvascular thrombosis, capillary leak, hypoperfusion, and direct cytokine-mediated mitochondrial dysfunction converges to cause multi-organ failure — acute kidney injury (from renal hypoperfusion and direct tubular injury by inflammatory mediators), acute lung injury progressing to ARDS, hepatic dysfunction (conjugated hyperbilirubinaemia), cardiomyopathy (septic cardiomyopathy, often diagnosed by echocardiography as new global LV systolic dysfunction), and encephalopathy (altered consciousness disproportionate to metabolic derangements). The immunosuppression phase is less immediately apparent but clinically important: after the initial hyperinflammatory burst, a prolonged immunosuppressed state characterised by lymphocyte apoptosis and monocyte deactivation increases vulnerability to secondary infections, particularly with gram-negative organisms and fungi, and accounts for a significant proportion of late sepsis mortality.
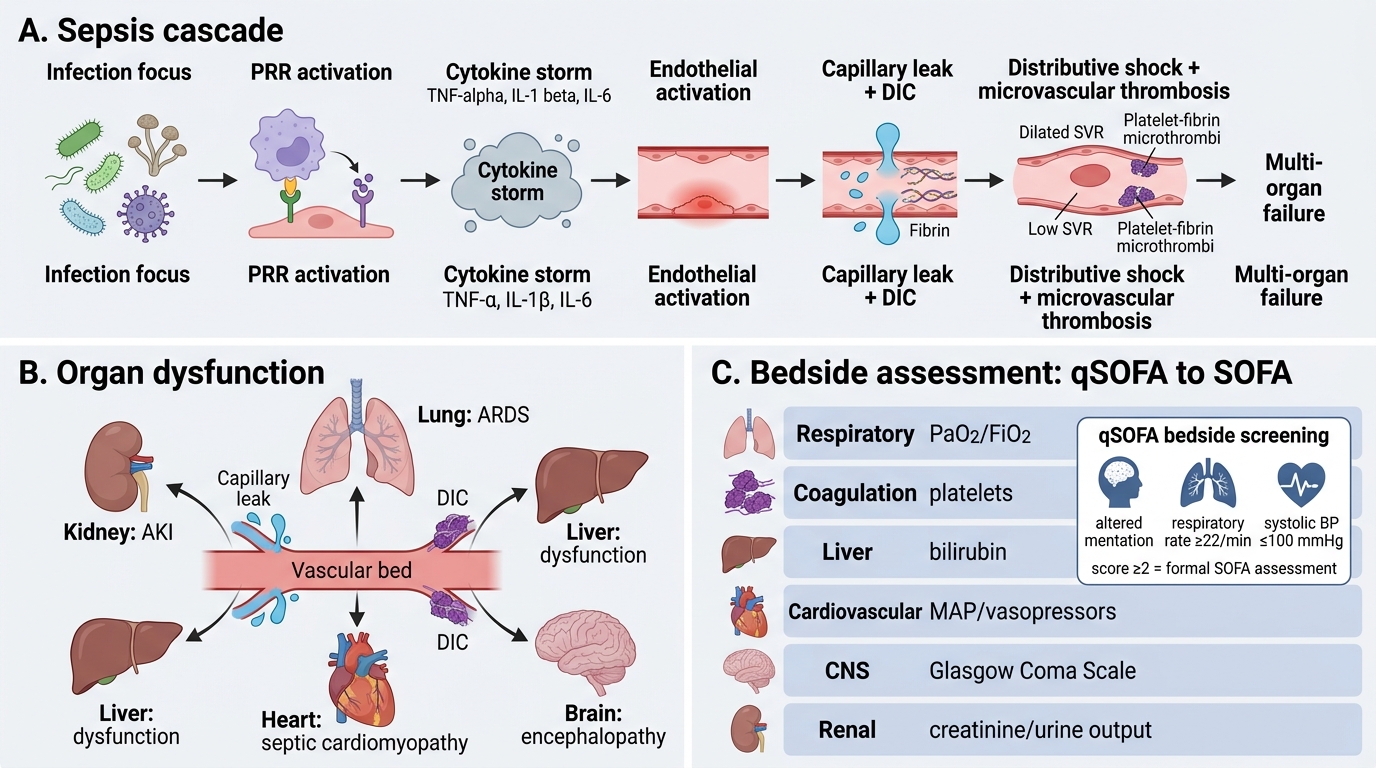
Sepsis Cascade and SOFA Organ Dysfunction
Management of sepsis follows the "Hour-1 Bundle" from the Surviving Sepsis Campaign (SSC 2018/2021 update): within the first hour of sepsis recognition, measure serum lactate (if ≥2 mmol/L, re-measure after 2 L resuscitation); obtain blood cultures (ideally two sets from different sites before antibiotics — do not delay antibiotics >45 minutes to obtain cultures); administer broad-spectrum IV antibiotics (empiric coverage guided by likely source and local antibiogram; in India, community-acquired sepsis often requires coverage for gram-negative Enterobacterales including cephalosporin-resistant organisms in healthcare-associated cases); begin 30 mL/kg IV crystalloid resuscitation for hypotension or lactate ≥4 mmol/L; and initiate vasopressors (noradrenaline is first-line) if hypotension does not respond to fluid resuscitation or MAP remains <65 mmHg. The quick-SOFA (qSOFA) score — comprising altered mentation, respiratory rate ≥22/min, and systolic BP ≤100 mmHg — each scoring 1 point, is a rapid bedside screening tool where a score of ≥2 should prompt the clinician to suspect sepsis and initiate formal SOFA assessment. Source control (drainage of abscess, removal of infected catheter) must be achieved within 6–12 hours when technically feasible.