Page 5 of 21
IM4.{9,14,18} | Fever of Unknown Origin — SDL Guide
Learning Objectives
- Define fever of unknown origin (FUO) using the classic Petersdorf-Beeson criteria and its modern adaptations for the normal host, neutropenic host, nosocomial host, and HIV-positive host
- Describe the major diagnostic categories of FUO — infectious, inflammatory/autoimmune, malignant, and miscellaneous — with India-relevant emphasis
- Explain the pathophysiology of each FUO category and how it differs from acute febrile illness
- Select and interpret appropriate diagnostic tests for the patient with prolonged fever, including inflammatory markers, specific serological tests, bone marrow aspiration, and HIV testing
- Develop a prioritised, cost-effective, stepwise diagnostic plan for a patient with prolonged fever based on clinical presentation and host context
INSTRUCTIONS
FUO is one of the most intellectually demanding presentations in medicine — it requires mastery of differential diagnosis, rational investigation sequencing, and the courage to reserve empiric therapy until a diagnosis is established. This module takes you through the definition, categories, pathophysiology, and a systematic investigative approach to FUO, with India-specific emphasis. Work through the clinical scenarios actively.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 11 — Fever of Unknown Origin (textbook)
- API Textbook of Medicine, 10th ed., Ch. 4 — Pyrexia of Unknown Origin (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 9 (textbook)
- Durack DT, Street AC. Fever of unknown origin — reexamined and redefined. Curr Clin Top Infect Dis. 1991 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old schoolteacher from Madhya Pradesh has had daily fever spiking to 39.5°C for the past five weeks. She has been treated empirically with three courses of antibiotics by three different physicians, none of which has produced sustained defervescence. Her haemoglobin is 9 g/dL, ESR 88 mm/hour, and CRP 56 mg/L. Blood cultures, urine cultures, Widal test, dengue NS1, and malaria RDT are all negative. A chest X-ray is normal. She is losing weight and feels increasingly fatigued. Her physician is frustrated; she is frightened. This is fever of unknown origin — not exotic or rare, but genuinely challenging precisely because the straightforward diagnoses have already been excluded. How do you approach this patient systematically so that you neither miss a curable cause nor harm her with untargeted empiric therapy? The answer lies not in more antibiotics, but in a structured diagnostic strategy that treats the investigation itself as the primary therapeutic intervention.
WHY THIS MATTERS
Fever of unknown origin is a presentation encountered in every general medicine ward in India. The spectrum of causes differs significantly from Western series — tuberculosis (particularly extrapulmonary), enteric fever with atypical presentation, visceral leishmaniasis (kala-azar), and autoimmune conditions such as SLE and adult-onset Still's disease predominate in Indian FUO series, as opposed to the higher proportion of lymphoma and connective tissue disease reported from North American and European studies. For the NMC final-year student, FUO tests the highest levels of clinical reasoning — not rote knowledge, but the ability to integrate clinical pattern, epidemiological context, and cost-conscious investigation design. Competencies IM4.9, IM4.14, and IM4.18 together demand that you can not only describe the FUO categories but develop and present a diagnostic plan at the bedside.
RECALL
Before proceeding, activate your prior knowledge from this cluster. The febrile response is driven by endogenous pyrogens — IL-1β, IL-6, TNF-α — acting via PGE2 on the hypothalamic thermostat. In acute febrile illness, the cause typically becomes apparent within days; in FUO, the same cytokine machinery is active but the source is occult. Recall the broad categories of fever aetiology from the Fever Foundations SDL: infectious (bacteria, viruses, fungi, parasites), inflammatory/autoimmune (SLE, Still's, vasculitis), malignant (lymphoma, leukaemia, solid tumours), and miscellaneous (drug fever, thromboembolic disease, factitious fever). Recall also that ESR (erythrocyte sedimentation rate) and CRP (C-reactive protein) are acute-phase reactants: ESR is driven by fibrinogen and immunoglobulins (slow to rise, slow to fall), while CRP is a direct hepatic acute-phase protein that rises within hours and falls rapidly when inflammation resolves. Both are non-specific but provide evidence of active systemic inflammation — their persistent elevation over weeks supports the biological reality of the FUO and argues against factitious fever.
Definition and Classification of Fever of Unknown Origin
Fever of unknown origin (FUO) was originally defined by Petersdorf and Beeson in 1961 as a temperature greater than 38.3°C (101°F) on multiple occasions over a period of at least 3 weeks, with no diagnosis established after 1 week of intensive in-hospital investigation. This definition was designed to exclude the vast majority of transient self-limiting febrile illnesses and to capture only those prolonged, unexplained fevers that genuinely challenge the clinician. The 1-week in-hospital investigation criterion was pragmatic in 1961 when outpatient testing was limited; modern adaptations by Durack and Street (1991) updated the definition to allow the 1-week investigation threshold to be fulfilled either in hospital or as thorough outpatient workup — reflecting the expanded availability of sophisticated ambulatory diagnostics.
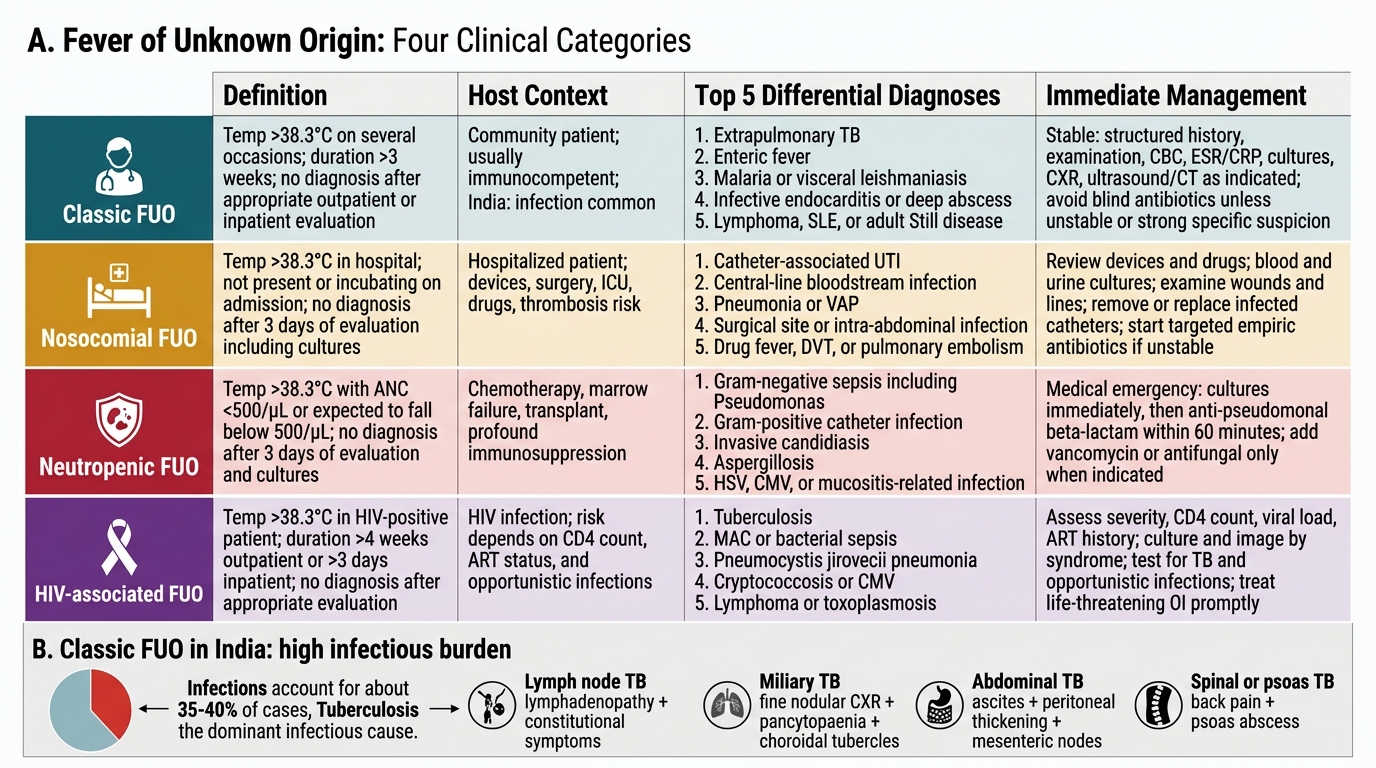
The updated classification by Durack and Street recognises four distinct FUO categories, each with its own differential diagnosis and investigative priorities:
1. Classic FUO (the original Petersdorf-Beeson category): temperature >38.3°C for ≥3 weeks, undiagnosed after at least 3 outpatient visits or 3 days of hospitalisation with appropriate investigation. This is the presentation seen in the immunocompetent, non-neutropenic, non-hospitalised patient. The differential is broad: infections (TB, brucellosis, infective endocarditis, visceral leishmaniasis, toxoplasmosis), autoimmune diseases (SLE, Still's, vasculitis, temporal arteritis, rheumatoid arthritis), malignancies (lymphoma, RCC, HCC), and miscellaneous causes (drug fever, factitious fever, pulmonary embolism, granulomatous diseases such as sarcoidosis and Crohn's).
2. Nosocomial FUO (hospital-acquired): temperature >38.3°C on multiple occasions in a hospitalised patient who was not febrile or incubating a condition at admission, remaining undiagnosed after 3 days of investigation. The differential shifts dramatically toward hospital-specific causes: Clostridioides difficile colitis (diarrhoea from recent antibiotics), catheter-associated bloodstream infection (every intravascular device is a suspect), surgical site infection (any post-operative fever beyond 5 days), drug fever from newly introduced medications, acalculous cholecystitis (particularly in ICU patients on prolonged fasting), Clostridium and gram-negative bacteraemia from GI sources, and deep venous thrombosis with pulmonary embolism. Nosocomial FUO is less about exotic diagnoses and more about systematic examination of every device, every recent drug, and every wound.
3. Neutropenic FUO (immune-deficient host): temperature >38.3°C in a patient with absolute neutrophil count <500 cells/mm³, remaining undiagnosed after 3 days with cultures pending. As discussed in Fever Foundations, neutropenic patients are at extreme risk of bacteraemia from gut flora translocation (gram-negative enteric organisms, gram-positive organisms from skin and intravascular devices) and from invasive fungal infections (Candida in the early neutropenic period; Aspergillus and moulds in prolonged neutropenia beyond 7–10 days). In practice, neutropenic FUO mandates empiric broad-spectrum antibiotics immediately; the diagnostic workup proceeds simultaneously rather than before therapy.
4. HIV-associated FUO: temperature >38.3°C on multiple occasions for ≥4 weeks as an outpatient or ≥3 days in hospital, in an HIV-positive patient with known or suspected HIV disease. The differential is dominated by opportunistic infections at the patient's CD4 count tier: at CD4 <200 cells/mm³ the most important causes are disseminated Mycobacterium avium complex (MAC), Pneumocystis jirovecii pneumonia (PJP), cryptococcal disease (meningitis, disseminated), and cytomegalovirus (CMV) disease; in India, disseminated tuberculosis is the single most common cause of HIV-associated FUO at any CD4 count. Lymphoma (particularly non-Hodgkin's lymphoma driven by EBV and Kaposi's sarcoma-associated herpesvirus) must also be considered.
Classification of Fever of Unknown Origin
Aetiology and Pathophysiology of Classic FUO in the Indian Context
The aetiology of classic FUO has been extensively studied in Indian hospital series, and the proportions differ meaningfully from Western case series. Understanding this epidemiological context is essential for building an India-appropriate differential diagnosis and investigation sequence. The general categories are infectious, inflammatory/autoimmune, malignant, and miscellaneous — but their relative proportions and the specific diagnoses within each category vary.
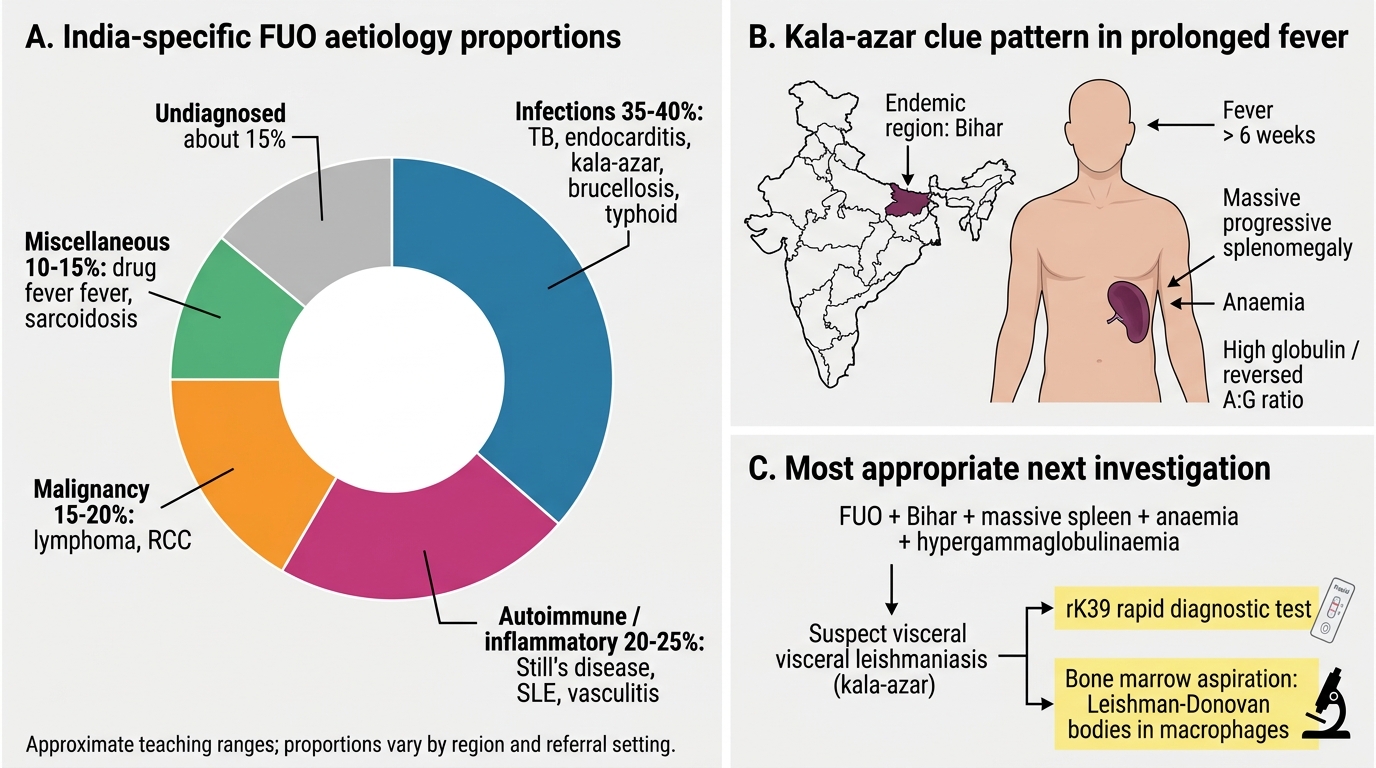
In Indian FUO series (published from AIIMS, JIPMER, CMC Vellore, and other major centres), infections account for approximately 35–40% of cases, significantly higher than the 15–20% reported in Western series. The most important infectious causes are: extrapulmonary tuberculosis — lymph node TB (the most common; presents with lymphadenopathy, constitutional symptoms, and elevated ESR), miliary TB (the most dangerous; bilateral fine nodular shadowing on CXR, bone marrow involvement causing pancytopaenia, and fundoscopic choroidal tubercles), abdominal TB (ascites, peritoneal thickening, mesenteric lymphadenopathy on imaging), and spinal/psoas TB (back pain, psoas abscess); infective endocarditis (prolonged fever with new or changing murmur, embolic phenomena, and positive blood cultures — the Duke criteria require specific microbiological and echocardiographic evidence); brucellosis (Brucella melitensis from unpasteurised milk or animal contact — undulant fever, hepatosplenomegaly, joint pain, and serology); visceral leishmaniasis or kala-azar (Leishmania donovani, endemic in Bihar/Jharkhand/West Bengal, presenting with prolonged fever, progressive splenomegaly that may be massive, anaemia, and hypergammaglobulinaemia — rK39 rapid test and bone marrow aspirate for amastigotes); and typhoid fever with atypical presentation (Salmonella typhi — the classic step-ladder fever with rose spots may be absent; prolonged fever with relative bradycardia and hepatosplenomegaly is the more common presentation in adults).
Inflammatory and autoimmune causes account for 20–25% of Indian FUO cases. The most important are: adult-onset Still's disease (AOSD) — a diagnosis of exclusion requiring the Yamaguchi criteria (fever ≥39°C for ≥1 week, arthralgia ≥2 weeks, typical rash, leucocytosis ≥10,000 with ≥80% granulocytes) alongside a markedly elevated serum ferritin, which is the most specific laboratory marker (ferritin >10,000 μg/L supports AOSD; ferritin >500 μg/L warrants AOSD consideration in the context of fever and arthritis); systemic lupus erythematosus (fever as the presenting feature, before rash and serological criteria are fully met — ANA is the key screening test, anti-dsDNA and complement levels for specificity); polyarteritis nodosa and ANCA-associated vasculitis (multi-system involvement, renal and pulmonary manifestations, ANCA serology); and giant cell arteritis in older patients (temporal headache, jaw claudication, elevated ESR >80 mm/hour, responding to steroids — temporal artery biopsy is definitive).
Malignancies account for 15–20% of Indian FUO cases. The most important are lymphoma (both Hodgkin's and non-Hodgkin's — lymphadenopathy, hepatosplenomegaly, elevated LDH and uric acid, weight loss, night sweats; diagnosis requires lymph node biopsy), leukaemia (pancytopaenia or blasts on peripheral smear, bone marrow biopsy), renal cell carcinoma (haematuria + flank pain + fever = classic triad; CT reveals the mass), and hepatocellular carcinoma (elevated AFP, liver mass on imaging in the context of chronic liver disease or hepatitis B/C infection). The miscellaneous category (approximately 10–15%) includes drug fever, granulomatous diseases (sarcoidosis — bilateral hilar lymphadenopathy, elevated ACE level, non-caseating granulomas), factitious fever, pulmonary embolism, and Munchausen syndrome.
India-Specific FUO Aetiology and Kala-Azar Diagnostic Clues
SELF-CHECK
A 32-year-old woman from Bihar has had fever for 6 weeks (temperature 39–40°C daily), progressive splenomegaly now reaching 14 cm below the left costal margin, haemoglobin 7.5 g/dL, and serum total protein 9.8 g/dL (albumin 2.8 g/dL, globulin 7.0 g/dL). Malaria RDT and blood cultures are negative. The MOST appropriate next investigation is:
A. Peripheral blood film for microfilariae
B. Bone marrow aspiration and rK39 rapid antigen test
C. Contrast CT abdomen to exclude lymphoma
D. Anti-nuclear antibody (ANA) and anti-dsDNA
Reveal Answer
Answer: B. Bone marrow aspiration and rK39 rapid antigen test
Progressive massive splenomegaly with prolonged fever, anaemia, and polyclonal hypergammaglobulinaemia (high globulin, reversed albumin:globulin ratio) in a patient from an endemic area (Bihar) is the classic presentation of visceral leishmaniasis (kala-azar). The rK39 rapid antigen test (based on a recombinant antigen from Leishmania donovani) has >90% sensitivity and specificity for kala-azar in the Indian subcontinent and is the first-line rapid diagnostic test. Bone marrow aspiration demonstrating Leishman-Donovan bodies (amastigotes within macrophages) is the gold standard for definitive diagnosis when serological tests are equivocal. Lymphoma can cause massive splenomegaly but the hypergammaglobulinaemia pattern and endemic context make kala-azar far more likely as the first diagnosis to establish. Microfilariae do not cause this clinical picture.
Diagnostic Tests in FUO: Selection and Interpretation
The investigation of FUO requires a disciplined, stepwise approach in which each test is ordered because it is likely to answer a specific clinical question — not because it belongs to a standard panel. Indiscriminate broad-spectrum investigation wastes resources and generates false-positive results that mislead rather than guide the clinician. The NMC competency IM4.14 specifies the categories of tests to understand: tests of inflammation, specific rheumatological tests, serological testing for pathogens including HIV, and bone marrow aspiration and biopsy. This section covers each in the context of FUO.
Tests of inflammation serve to confirm the biological reality of sustained inflammation and provide a baseline against which treatment response can be measured. ESR (Westergren method; normal <20 mm/hour in men, <30 mm/hour in women, both age-adjusted): in FUO, an ESR >50 mm/hour is consistent with active systemic inflammation; ESR >100 mm/hour is strongly associated with temporal arteritis, multiple myeloma, TB, or infective endocarditis. The ESR is heavily influenced by fibrinogen, immunoglobulins, and red cell morphology — it rises slowly (days) and falls slowly after inflammation resolves, making it useful for trend monitoring. CRP (high-sensitivity CRP; normal <10 mg/L in most labs): rises within 4–6 hours of an inflammatory stimulus and falls within 24–48 hours of its resolution. CRP is more useful for real-time monitoring of active inflammation than ESR. Procalcitonin (PCT): a precursor of calcitonin that is specifically induced by bacterial infections via pathogen-derived lipopolysaccharide; PCT >0.5 ng/mL suggests bacterial infection; PCT >2 ng/mL suggests severe bacterial sepsis; PCT is NOT elevated in viral infections or most autoimmune conditions, giving it specificity for bacterial aetiology. PCT is particularly valuable in distinguishing bacterial from non-bacterial causes of FUO. Serum ferritin: markedly elevated in HLH (>10,000 ng/mL), Adult-onset Still's disease (>5,000 μg/L is highly specific), and some infections (visceral leishmaniasis); a ferritin >500 μg/L in the context of fever should always prompt consideration of AOSD and HLH.
Specific rheumatological tests are ordered when the clinical picture or inflammatory marker pattern suggests an autoimmune aetiology. ANA (antinuclear antibody): a sensitive but non-specific screening test for SLE; titre >1:160 is significant; a negative ANA (low titre <1:40) makes SLE very unlikely. If ANA is positive, proceed to anti-dsDNA (specific for SLE, correlates with renal disease activity and complement consumption), anti-Smith (highly specific for SLE), and complement levels (C3, C4) (consumed in active SLE — low C3/C4 with high anti-dsDNA = active lupus nephritis). RF (rheumatoid factor) and anti-CCP antibodies are positive in rheumatoid arthritis; anti-CCP is more specific than RF. ANCA (anti-neutrophil cytoplasmic antibody): p-ANCA (anti-MPO) and c-ANCA (anti-PR3) — used in vasculitis diagnosis. Serum ACE (angiotensin-converting enzyme): elevated in sarcoidosis (sensitivity ~60%, specificity ~90%), but normal ACE does not exclude sarcoidosis.
Serological testing for pathogens should be targeted to clinical probability. Blood culture (most important single test in any FUO; three sets from different sites at different times, held for 5–14 days for slow-growing organisms like Brucella and Bartonella) is the foundation. HIV ELISA/Western blot (or fourth-generation HIV Ag/Ab combo test): must be ordered in ALL patients with unexplained prolonged fever; universal, not risk-stratified. Widal test for typhoid has significant limitations (false positives from previous vaccination, prior infection, and cross-reactivity with other Salmonella species; a single titre of ≥1:160 for TO antigen and ≥1:80 for TH antigen is conventionally significant but poorly predictive alone — blood culture during the first 10 days of illness is superior). Brucella serology (Standard Agglutination Test, SAT ≥1:160 is significant). Toxoplasma IgM/IgG: relevant in immunosuppressed patients and febrile lymphadenopathy. EBV VCA IgM and CMV IgM: for infectious mononucleosis syndrome. Mantoux/tuberculin skin test and IGRA (Interferon-Gamma Release Assay): for TB exposure; IGRA (QuantiFERON-TB Gold) is more specific than Mantoux in BCG-vaccinated individuals, but neither distinguishes active from latent TB. rK39 rapid test for kala-azar (as above).
Bone marrow aspiration and biopsy (IM4.14) is indicated in FUO when: haematological malignancy is suspected (cytopaenias, blast cells on peripheral smear, unexplained lymphadenopathy); visceral leishmaniasis is suspected (identify amastigotes within macrophages); disseminated TB or MAC is suspected in an immunosuppressed patient (culture of bone marrow is positive in 30–40% of miliary TB); or haemophagocytosis is suspected (HLH). The biopsy provides material for histology, culture, and immunophenotyping. Bone marrow examination is regarded as a second-tier investigation — not a first-line test — but is one of the highest-yield second-tier tests in Indian FUO series.
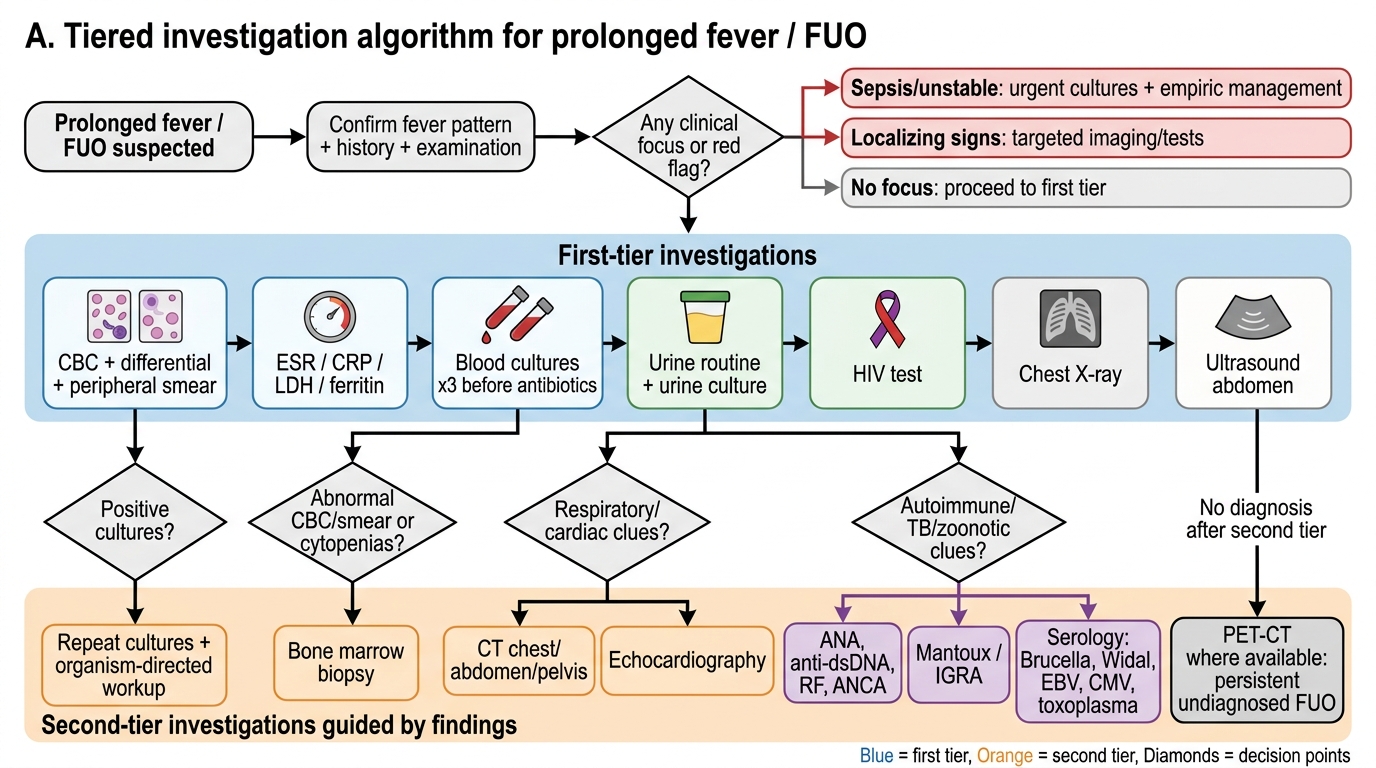
Tiered Investigation Algorithm for Prolonged Fever / FUO