Page 9 of 19
IM5.11-14 | Liver Disease Diagnostic Testing — SDL Guide (Part 2)
Ascitic Fluid Analysis and SAAG Interpretation
Ascitic fluid analysis — obtained by diagnostic paracentesis — is the single most important investigation when ascites is newly identified or when a cirrhotic patient with known ascites deteriorates clinically. The procedure is safe, minimally invasive, and provides diagnostic information that cannot be obtained by any other means. Failure to perform a diagnostic paracentesis in a deteriorating cirrhotic patient represents a serious clinical omission, because spontaneous bacterial peritonitis (SBP) — a common, life-threatening complication — may be asymptomatic or present with non-specific signs and can only be definitively excluded by ascitic fluid analysis.
Procedure: Diagnostic paracentesis is performed by inserting a needle or cannula (typically 18–20 gauge) into the peritoneal cavity under ultrasound guidance or in the left lateral abdominal quadrant (avoiding epigastric vessels, avoiding areas of bowel loops, avoiding the area of previous abdominal surgery). Ultrasound guidance improves safety and reduces failure rate. Contraindications: uncorrectable coagulopathy (INR >2.5, platelets <50,000/mm³ — relative contraindications; INR alone should not be a barrier in cirrhotic patients who need the procedure urgently), suspected bowel obstruction, or known abdominal adhesions. Collect 20–30 mL for diagnostic purposes; send for: cell count and differential (PMN count), total protein, albumin, LDH, glucose, culture (bedside inoculation into blood culture bottles directly from the paracentesis needle dramatically increases culture sensitivity — yield rises from 40–50% to ~70–80%), cytology (if malignant ascites suspected), and amylase (if pancreatic ascites suspected).
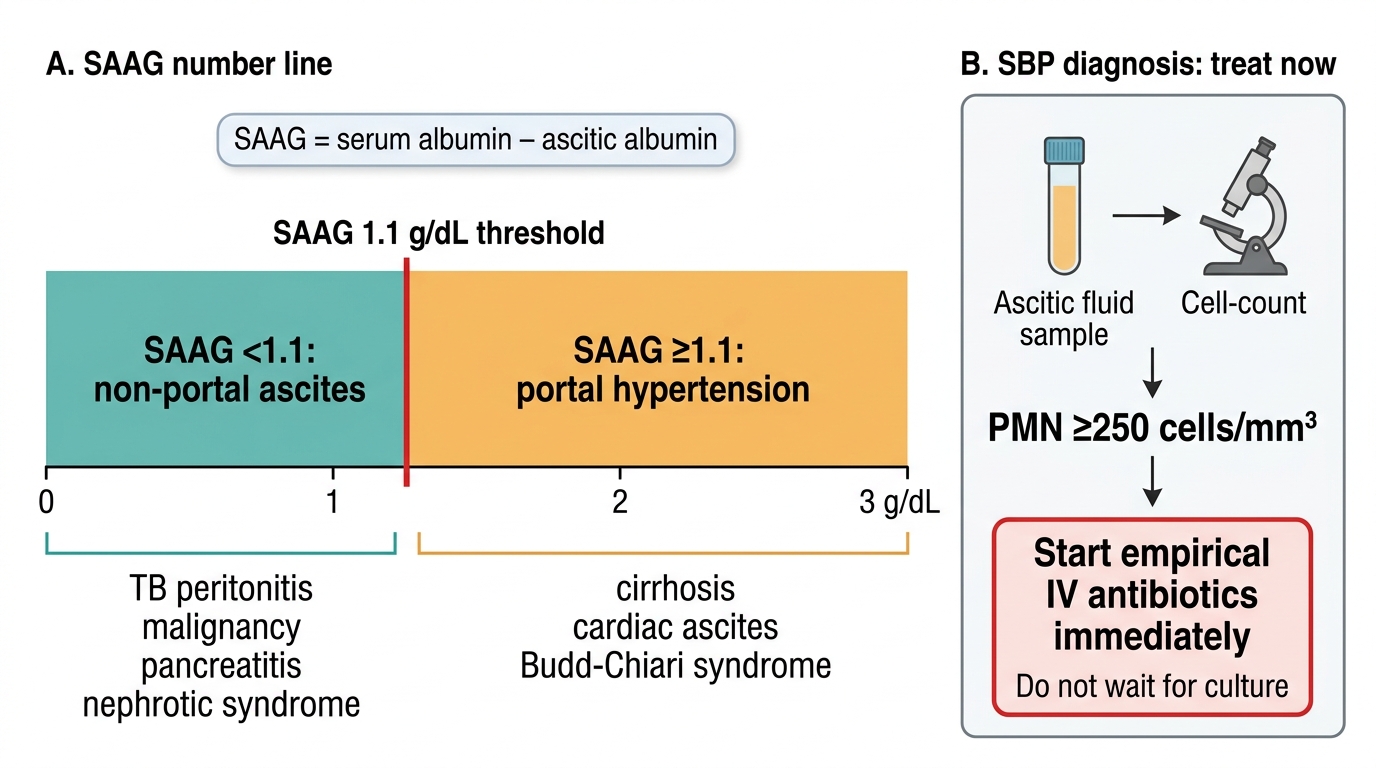
SAAG (Serum-Ascites Albumin Gradient): SAAG = serum albumin (g/dL) − ascites albumin (g/dL). This calculation must be performed using SIMULTANEOUSLY drawn samples (ascites and blood taken on the same day) to avoid error from fluctuating serum albumin. The SAAG reflects the difference in oncotic pressure between portal blood and ascitic fluid and is a reliable surrogate for portal pressure:
- SAAG ≥ 1.1 g/dL = high-gradient ascites = portal hypertension with sensitivity >97%. Causes: cirrhosis (85% of all ascites), right heart failure / cardiac ascites (distinguish by elevated JVP, hepatojugular reflux, bilateral pleural effusions), Budd-Chiari syndrome (hepatic vein thrombosis — palpable tender liver, hepatic Doppler absent/reversed flow), constrictive pericarditis.
- SAAG < 1.1 g/dL = low-gradient ascites = non-portal hypertension aetiology. Causes: peritoneal tuberculosis (most important in India — lymphocyte-predominant exudate, high protein, low glucose, ADA elevated, Ziehl-Neelsen/culture/PCR on ascitic fluid), peritoneal malignancy (cytology positive in 50–70% of malignant ascites), pancreatitis/pancreatic ascites (high amylase in ascitic fluid), nephrotic syndrome (low protein both serum and ascites — SAAG may be borderline).
A key interpretive point: SAAG is not the same as total ascitic protein. The older classification of ascites as 'transudate' (protein <25 g/L) vs 'exudate' (protein >25 g/L) is less accurate than SAAG for identifying portal hypertension, because cirrhotic patients often have low serum albumin that brings ascitic protein into the 'exudate' range even though the mechanism is portal hypertension. SAAG supersedes total protein classification.
Cell count and differential for SBP diagnosis:
- PMN (polymorphonuclear leucocyte) count ≥ 250 cells/mm³ is the diagnostic threshold for SBP, even before culture results are available. Culture is positive in only 40–50% of SBP cases (low bacterial load in peritoneal fluid makes culture insensitive). Therefore, PMN ≥250/mm³ = treat empirically with third-generation cephalosporin (ceftriaxone 1–2 g IV daily or cefotaxime 2 g IV three times daily) regardless of culture result.
- PMN < 250/mm³ with positive culture = bacterascites — culture is positive but cell count is below threshold. Clinical context determines treatment: if symptomatic, treat; if asymptomatic, repeat paracentesis.
- Lymphocyte-predominant fluid (>70% lymphocytes, low PMN): suggests TB peritonitis or malignant ascites. Order Ziehl-Neelsen stain, MGIT TB culture, ADA (adenosine deaminase) level (>30 IU/L is suggestive of TB peritonitis), and cytology.
- Total protein: protein <15 g/L in ascitic fluid is a risk factor for developing SBP (low opsonic activity) — these patients are candidates for primary SBP prophylaxis with norfloxacin.
In the hook scenario: ascitic fluid albumin 4 g/dL; serum albumin must be obtained to calculate SAAG. PMN 180 cells/mm³ = below 250 threshold — SBP not confirmed, but if patient is symptomatic, clinical judgement applies. Full culture result is pending.
SAAG Interpretation and SBP Treatment Threshold
SELF-CHECK
A 55-year-old cirrhotic patient develops fever and abdominal pain. Diagnostic paracentesis is performed. The results show: ascitic fluid PMN 320 cells/mm³, total protein 18 g/L, ascitic albumin 6 g/dL, serum albumin 2.8 g/dL. Culture is pending. What is the diagnosis and immediate management?
A. SAAG 2.8 − 6 = negative, indicating non-portal ascites; treat for TB peritonitis
B. SBP diagnosed (PMN ≥250/mm³); start empirical ceftriaxone IV immediately without waiting for culture
C. SAAG < 1.1 indicates malignant ascites; send cytology and defer antibiotics
D. PMN 320/mm³ is a normal finding; repeat paracentesis in 48 hours
Reveal Answer
Answer: B. SBP diagnosed (PMN ≥250/mm³); start empirical ceftriaxone IV immediately without waiting for culture
The PMN count of 320 cells/mm³ exceeds the diagnostic threshold of ≥250 cells/mm³ for SBP. This threshold alone justifies immediate empirical antibiotic treatment — do not wait for culture results, as culture is only positive in 40–50% of SBP cases. Start ceftriaxone (or cefotaxime) IV immediately. SAAG = serum albumin 2.8 − ascites albumin 6 would give a negative number — this is mathematically impossible in practice because SAAG is always serum albumin MINUS ascites albumin; if ascites albumin somehow exceeds serum albumin, re-check sample labelling (a common practical error). In portal hypertension, serum albumin is typically lower than ascites albumin only in cardiac ascites. For diagnosis purposes, the SBP diagnosis is made on PMN threshold alone.
Liver Imaging: Ultrasound, MRCP, ERCP, and CT
Imaging in liver disease serves three broad purposes: characterising the hepatic parenchyma (echotexture, size, focal lesions), evaluating the biliary system (intrahepatic or extrahepatic duct dilatation, stone burden, strictures), and assessing for portal hypertension and its complications (portal vein diameter, collateral vessels, spleen size, ascites). The choice of imaging modality follows a hierarchy that prioritises the least invasive, widely available, and highest-yield test first, escalating to more specific or invasive modalities when the first-line test is inadequate or when intervention is planned. Selecting the right imaging modality in the right sequence avoids both the risk of an unnecessary invasive procedure (ERCP ordered when MRCP would have been diagnostic) and the delay of an inadequate first test (plain X-ray ordered for suspected biliary obstruction when ultrasound would immediately show duct dilatation). Each modality answers a different question, and knowing which question you are asking before you order the scan is the core skill that IM5.12 assesses at the KH level.
Provided image
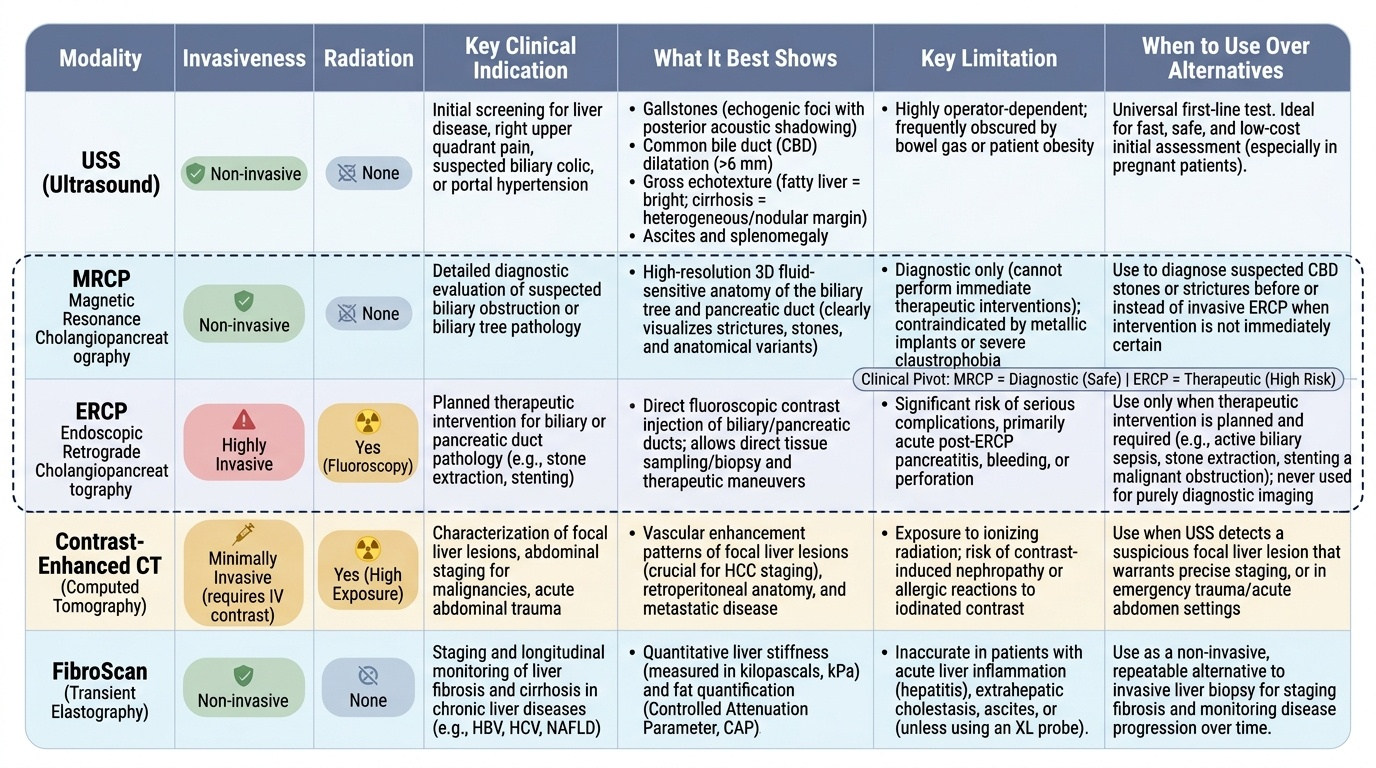
Ultrasound abdomen is the universal first-line liver imaging investigation. It is non-invasive, no ionising radiation, repeatable, and widely available at district hospital level in India. Ultrasound can:
- Assess hepatic echotexture: fatty liver appears bright (echogenic) compared to the kidney cortex; cirrhosis produces coarsened, heterogeneous echotexture with irregular surface (nodular or irregular margin = advanced fibrosis); acute hepatitis may show normal echotexture or mild heterogeneity.
- Detect focal liver lesions: hepatocellular carcinoma (HCC), metastases, haemangiomas, liver abscess, cysts. A hypoechoic or heterogeneous focal lesion in a cirrhotic liver warrants characterisation by contrast-enhanced CT or MRI for HCC staging.
- Evaluate the biliary system: normal common bile duct diameter ≤6 mm (up to 10 mm post-cholecystectomy). Dilatation indicates obstruction. Gallstones appear as echogenic foci with posterior acoustic shadowing (the most specific sonographic sign of stones).
- Assess portal hypertension: portal vein diameter >13 mm, splenomegaly (>12 cm longitudinal), ascites (even small amounts), collateral vessels (recanalized paraumbilical vein, spleno-renal collaterals).
- Doppler ultrasound adds assessment of portal vein flow direction (reversal = severe portal hypertension), hepatic vein flow (absent/reversed in Budd-Chiari syndrome), and hepatic artery resistive index.
Ultrasound limitations: operator-dependent, poor visualisation in obese patients and in the presence of large amounts of bowel gas, limited assessment of the distal common bile duct (behind duodenum), and limited characterisation of complex focal lesions.
MRCP (Magnetic Resonance Cholangiopancreatography): Non-invasive, high-resolution imaging of the biliary and pancreatic ductal systems without contrast or radiation. MRCP uses heavily T2-weighted sequences in which fluid appears bright, creating a 'cholangiogram' effect. It is the investigation of choice when extrahepatic biliary obstruction is suspected but therapeutic intervention is not immediately planned — it provides exquisite anatomical detail of the biliary tree (level and cause of obstruction, stricture characterisation, PSC beaded pattern, hilar cholangiocarcinoma, IPMN). Advantages over ERCP: no radiation, no risk of post-ERCP pancreatitis, no need for sedation or endoscopy. Limitation: MRCP is diagnostic only — it cannot provide treatment in the same session.
ERCP (Endoscopic Retrograde Cholangiopancreatography): A combined endoscopic and fluoroscopic procedure in which a side-viewing duodenoscope is advanced to the duodenum, the ampulla is cannulated, and contrast is injected into the biliary and pancreatic ducts under fluoroscopic guidance. ERCP is primarily a therapeutic procedure — it allows sphincterotomy (incision of the sphincter of Oddi to allow stone passage), stone extraction with a balloon or basket catheter, placement of biliary stents (for strictures from malignancy or post-surgical), and brush cytology of biliary strictures. ERCP is NOT indicated as a purely diagnostic procedure when MRCP is available. Complications: post-ERCP pancreatitis (3–5%), cholangitis, perforation, haemorrhage — all require active management.
CT abdomen (contrast-enhanced, triphasic): Used for: (a) characterisation of focal liver lesions — the hallmark of HCC on CT is arterial phase enhancement followed by portal-phase washout (contrast arrives early via aberrant arterial supply, then washes out, leaving lesion dark relative to liver in the portal phase — this pattern on dynamic CT is so specific for HCC that biopsy can be omitted in cirrhotic patients); (b) staging of hepatic and biliary malignancy (vascular involvement, lymph nodes, distant metastases); (c) diagnosis of complications (liver abscess — rim-enhancing fluid collection, often containing gas; Budd-Chiari — caudate lobe hypertrophy, absent hepatic veins); (d) pre-surgical planning. Not used as first-line imaging because of ionising radiation and cost.
FibroScan (transient elastography): Measures liver stiffness (kPa) as a surrogate for hepatic fibrosis. Normal liver stiffness <7.0 kPa; values >12.5 kPa suggest cirrhosis. Increasingly used to avoid liver biopsy in staging chronic hepatitis B and C, monitoring antiviral treatment response, and risk-stratifying NAFLD. Limitation: unreliable in obese patients (XL probe required) and in the presence of ascites, active inflammation (falsely elevated by acute hepatitis), and right heart failure.
Diagnostic Algorithm: Integrating LFTs, Serology, and Imaging
A structured diagnostic algorithm for liver disease prevents both under-investigation (missing a treatable cause) and over-investigation (ordering an undirected panel that produces noise without signal). The algorithm described here, aligned with IM5.13 competency, is built around the LFT pattern as the primary branch point, with subsequent branches determined by clinical context.
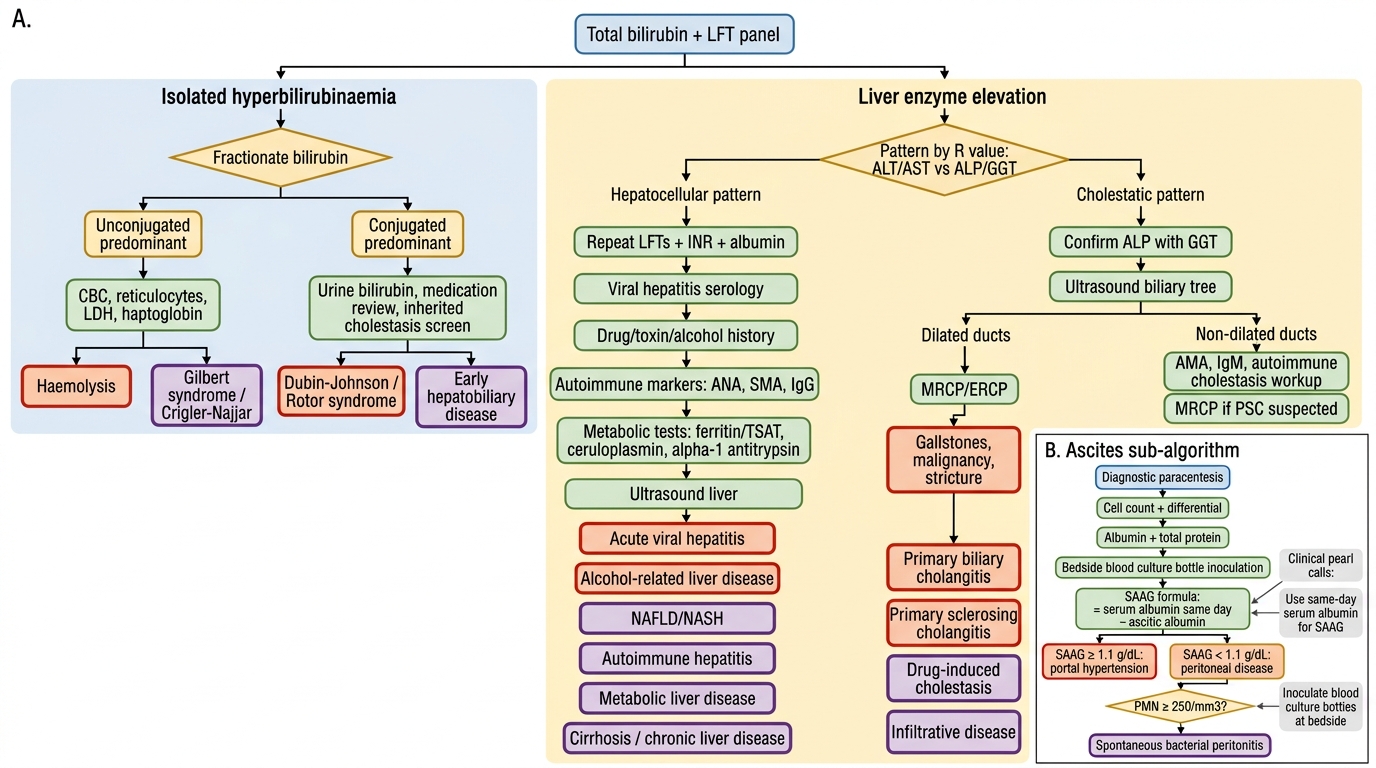
The IM5.13 algorithm — diagnostic approach based on hyperbilirubinaemia, LFT changes, and hepatitis serology:
Step 1 — Is this primarily a hyperbilirubinaemia problem or a liver enzyme problem?
Measure total bilirubin, direct bilirubin, and indirect bilirubin. If bilirubin is elevated but ALT, AST, and ALP are all within normal limits → isolated hyperbilirubinaemia pathway: check CBC and reticulocyte count (haemolysis?); if haemolysis excluded, consider Gilbert syndrome (unconjugated, mild, exacerbated by fasting/illness — benign), Dubin-Johnson, or Rotor syndrome (conjugated/mixed, benign).
Step 2 — Determine the LFT pattern: hepatocellular vs cholestatic.
As established above. This single determination creates two distinct investigation pathways.
Hepatocellular pattern pathway:
- Check ALT and AST levels (absolute magnitude matters: ALT >20× ULN = acute severe hepatitis — acute viral, ischaemic, or toxic; ALT 3–20× ULN = active hepatitis — viral or autoimmune; ALT <3× ULN = mild/chronic injury — NAFLD, chronic viral, drug).
- Calculate AST:ALT ratio: >2:1 with alcohol history = ALD; <2:1 = viral, autoimmune, or NAFLD.
- Order hepatitis serology based on risk factors: HBsAg + anti-HBc IgM (acute HBV) + anti-HAV IgM (acute HAV) + anti-HCV → HCV RNA if positive.
- If serology negative: check autoimmune markers (anti-smooth muscle antibody ASMA, anti-nuclear antibody ANA for autoimmune hepatitis; AMA for PBC), serum caeruloplasmin (Wilson disease in patients <40 years), iron studies (ferritin + transferrin saturation for haemochromatosis), alpha-1-AT level.
- Ultrasound abdomen: assess for fatty liver (NAFLD), hepatomegaly, focal lesions.
Cholestatic pattern pathway:
- Confirm hepatic origin: check GGT alongside ALP — if ALP elevated but GGT normal, source is bone (check bone ALP isoenzyme, consider bone disease, growth in adolescents, pregnancy).
- If hepatic cholestasis confirmed: ultrasound abdomen immediately — is the common bile duct dilated (>6 mm)? If yes → extrahepatic obstruction → proceed to MRCP (first) or ERCP (if intervention planned). If no duct dilatation → intrahepatic cholestasis pathway: order AMA (PBC), anti-smooth muscle Ab/ANA (autoimmune hepatitis with cholestatic overlap), drug history review, serum IgG4 (autoimmune cholangiopathy).
Ascites pathway (when ascites is present):
- Diagnostic paracentesis immediately: SAAG, PMN count, protein, culture.
- SAAG ≥1.1 + cirrhotic context: portal hypertension ascites — assess for SBP (PMN threshold), then manage per SBP protocol or standard ascites management.
- SAAG <1.1: investigate for TB peritonitis (ADA, ZN stain, culture), malignancy (cytology, CT for primary), pancreatitis (amylase).
The algorithm is iterative — subsequent test results redirect the pathway. The key operational principle is to test the leading hypothesis first (the cheapest, most available, most likely test), then escalate to more specific tests only when the first test is equivocal or negative.
Diagnostic Algorithm for Liver Disease Investigation
CLINICAL PEARL
When interpreting ascitic fluid, the SAAG calculation must use serum albumin measured on the same day as the paracentesis. Using a serum albumin from a week earlier — as often happens when the blood result is retrieved from old records — introduces significant error because albumin can change rapidly in decompensating liver disease. This is a common clinical mistake: always check the dates of both values before computing SAAG.
A second pearl: bedside inoculation of ascitic fluid into blood culture bottles (rather than sending the fluid in a plain tube to the laboratory) increases SBP culture sensitivity from ~40% to ~70–80%. The reason is simple — the culture medium in blood culture bottles provides immediate nutrient support for the low-density bacterial inoculum in SBP. This is a practical tip that costs nothing and substantially improves diagnostic yield. Every diagnostic paracentesis in a cirrhotic should inoculate blood culture bottles directly at the bedside.